


( See also Herpes Simplex Virus (HSV) Infections in adults and Overview of Neonatal Infections.)
Neonatal herpes simplex virus (HSV) infection has high mortality and significant morbidity. Incidence estimates range from 1/3,000 to 1/20,000 births. HSV type 2 causes more cases than HSV type 1.
HSV is usually transmitted during delivery through an infected maternal genital tract. Transplacental transmission of virus and hospital-acquired spread from one neonate to another by hospital personnel or family may account for some cases. Mothers of neonates with HSV infection tend to have newly acquired genital infection, but many have not had symptoms at the time of delivery.
Symptoms and Signs of Neonatal HSV Infection
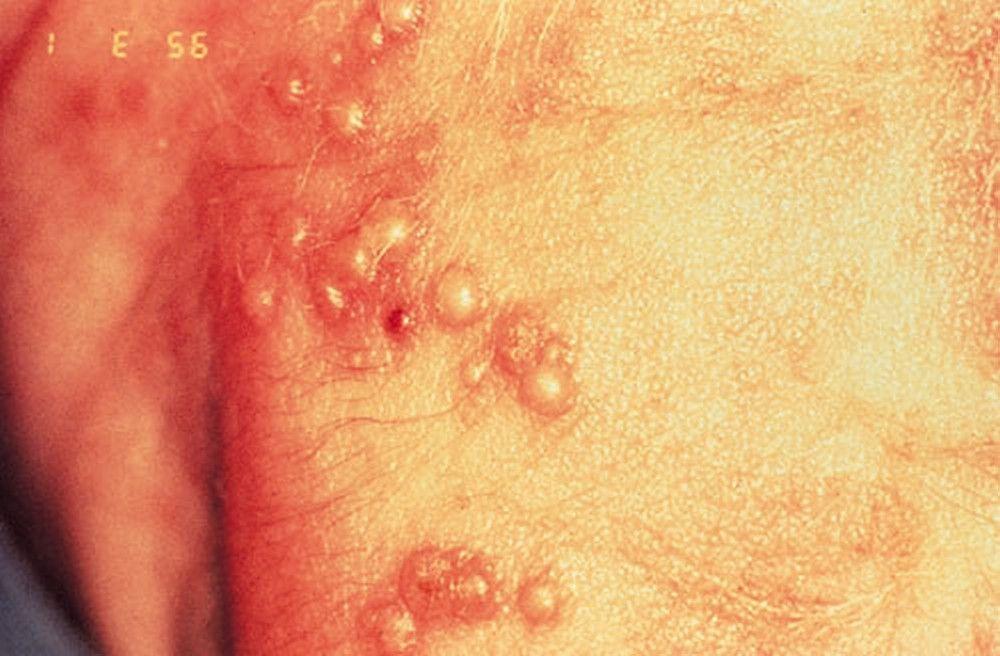
Manifestations generally occur between the 1st and 3rd weeks of life but rarely may not appear until as late as the 4th week. Neonates may present with local or disseminated disease. Skin vesicles are common with either type, occurring in about 70% overall. Neonates with no skin vesicles usually present with localized central nervous system (CNS) disease. In neonates with isolated skin or mucosal disease, progressive or more serious forms of disease frequently follow within 7 to 10 days if left untreated.

DR P. MARAZZI/SCIENCE PHOTO LIBRARY

DR M.A. ANSARY/SCIENCE PHOTO LIBRARY

By permission of the publisher. From Demmler G: Congenital and perinatal infections. In Atlas of Infectious Diseases: Pediatric Infectious Diseases. Edited by CM Wilfert. Philadelphia, Current Medicine, 1998.


DR P. MARAZZI/SCIENCE PHOTO LIBRARY


DR M.A. ANSARY/SCIENCE PHOTO LIBRARY

By permission of the publisher. From Demmler G: Congenital and perinatal infections. In Atlas of Infectious Diseases: Pediatric Infectious Diseases. Edited by CM Wilfert. Philadelphia, Current Medicine, 1998.
Localized disease
Neonates with localized disease can be divided into 2 groups. One group has encephalitis manifested by neurologic findings, cerebrospinal fluid pleocytosis, and elevated protein concentration, with or without concomitant involvement of the skin, eyes, and mouth. The other group has only skin, eye, and mouth involvement and no evidence of CNS or organ disease.
Disseminated disease
Neonates with disseminated disease and visceral organ involvement have hepatitis, pneumonitis, disseminated intravascular coagulation, or a combination, with or without encephalitis or skin disease.
Other signs, which can occur singly or in combination, include temperature instability, lethargy, hypotonia, respiratory distress, apnea, and seizures.
Diagnosis of Neonatal HSV Infection
HSV culture or polymerase chain reaction (PCR) testing
Sometimes immunofluorescent testing of lesions or electron microscopy
Rapid diagnosis by viral culture or HSV PCR is essential. The most common site of retrieval is skin vesicles. The nasopharynx, eyes, rectum, blood, and cerebrospinal fluid should also be tested. In some neonates with encephalitis, virus is present only in the CNS. Diagnosis of neonatal HSV also can be made by immunofluorescence of lesion scrapings, particularly with use of monoclonal antibodies, and electron microscopy.
If no diagnostic virology facilities are available, a Tzanck test of the lesion base may show characteristic multinucleated giant cells and intranuclear inclusions, but this test is less sensitive than culture, and false-positives can occur.
Prognosis for Neonatal HSV Infection
Death is uncommon in neonates with local disease limited to the skin, eyes, or mouth. However, without treatment, many of these neonates will progress to disseminated disease or CNS disease that may be unrecognized.
Treatment of Neonatal HSV Infection
Supportive therapy
acyclovir 300 mg/m2 3 times a day for 6 months; this long-term regimen improves neurodevelopmental outcomes at 1 year of age but may cause neutropenia.
Vigorous supportive therapy is required, including appropriate IV fluids, alimentation, respiratory support, correction of clotting abnormalities, and control of seizures.
For localized disease (skin, mouth, or conjunctivae), treatment is acyclovirtreatment of herpetic keratoconjunctivitis).
Prevention of Neonatal HSV Infection
Efforts to prevent neonatal transmission have not been very effective. Universal screening has not been recommended or shown to be effective, and most maternal infections with risk of transmission are asymptomatic. However, women with genital lesions at term should have testing and serology to diagnose HSV and determine the risk of transmission as well as to direct the care of the exposed but asymptomatic neonate. Cesarean delivery for women known to have a high risk of transmission (eg, active genital lesions present at term) has been shown to decrease transmission and is recommended even if the membranes have ruptured. Also, fetal scalp monitors should not be used during labor on infants whose mothers have suspected active genital herpes. Asymptomatic neonates born to women with active genital lesions at the time of delivery should be evaluated and tested for HSV infection. Additional information is available from the American Academy of Pediatrics (1).
Prevention reference
1. Kimberlin DW, Baley J, Committee on infectious diseases, Committee on fetus and newborn: Guidance on management of asymptomatic neonates born to women with active genital herpes lesions. Pediatrics 131(2):e635-646, 2013. doi: 10.1542/peds.2012-3216
Key Points
Neonatal herpes may be localized to the skin, eyes, or mouth, the central nervous system, or may be disseminated.
Encephalitis and disseminated disease have a high mortality rate, and neurologic sequelae are common among survivors.
In suspected cases, presumptive therapy and rapid diagnosis by HSV PCR of cerebrospinal fluid, blood, or lesions are essential to optimize outcomes.
Do cesarean delivery if the mother has active genital herpes lesions present at term.






