


Hypersensitivity pneumonitis is a syndrome of cough, dyspnea, and fatigue caused by sensitization and subsequent hypersensitivity to environmental (frequently occupational or domestic) antigens. Acute, subacute, and chronic forms exist; all are characterized by acute interstitial inflammation and development of granulomas and fibrosis with long-term exposure. Diagnosis is based on a combination of history, physical examination, imaging tests, bronchoalveolar lavage, and biopsy. Short-term treatment is with corticosteroids; long-term treatment is antigen avoidance and, if fibrosis is present, often immunosuppression.
(See also Overview of Interstitial Lung Disease.)
Etiology of Hypersensitivity Pneumonitis
Over 300 antigens have been identified as triggers for hypersensitivity pneumonitis. Antigens encountered through farming, birds, and water contamination account for about 75% of cases.
Antigens are commonly categorized by type and occupation (see table Examples of Hypersensitivity Pneumonitis); farmer’s lung, caused by inhalation of hay dust containing thermophilic actinomycetes, is the prototype. Substantial overlap exists between hypersensitivity pneumonitis and chronic bronchitis in farmers, in whom chronic bronchitis is far more common, occurs independently of smoking status, is linked to thermophilic actinomycete exposure, and leads to findings similar to those of hypersensitivity pneumonitis on diagnostic testing.
Pathophysiology of Hypersensitivity Pneumonitis
The disorder seems to represent a type IV hypersensitivity reaction, in which repeated exposure to antigen in genetically susceptible people leads to acute neutrophilic and mononuclear alveolitis, followed by interstitial lymphocytic infiltration and granulomatous reaction. Fibrosis with bronchiolar obliteration occurs with continued exposure.
Circulating precipitins (antibodies sensitized to antigen) seem not to have a primary etiologic role, and clinical history of allergy (such as asthma and seasonal allergies) is not a predisposing factor. Cigarette smoking seems to delay or prevent development, perhaps through down-regulation of the lung’s immune response to inhaled antigens. However, smoking may exacerbate the disease once established.
Hypersensitivity pneumonitis has clinical similarities to other disorders that have different pathophysiologies.
Organic dust toxic syndrome (pulmonary mycotoxicosis, grain fever), for example, is a syndrome consisting of fever, chills, myalgias, and dyspnea that does not require prior sensitization and is thought to be caused by inhalation of toxins produced by fungi or other contaminants of organic dust.
Silo filler’s disease may lead to respiratory failure, acute respiratory distress syndrome (ARDS), and bronchiolitis obliterans or bronchitis but is caused by inhalation of toxic nitrogen oxides produced by freshly fermented corn or alfalfa silage.
Occupational asthma causes dyspnea in people previously sensitized to an inhaled antigen, but features such as airflow obstruction, airway eosinophilia, and differences in triggering antigens distinguish it from hypersensitivity pneumonitis.
Symptoms and Signs of Hypersensitivity Pneumonitis
Symptoms and signs tend to depend on whether onset is
Acute
Chronic
Subacute
Only a small proportion of exposed people develop symptoms and in most cases only after weeks to months of exposure and sensitization.
Acute hypersensitivity pneumonitis
Acute disease occurs in previously sensitized people with acute high-level antigen exposure and manifests as fever, chills, cough, bilateral vice-like chest tightness (as can occur in asthma), and dyspnea 4 to 8 hours after exposure. Anorexia, nausea, and vomiting may also be present. Physical examination shows tachypnea, diffuse fine-to-medium inspiratory crackles, and, in almost all cases, absence of wheezing.
Chronic hypersensitivity pneumonitis
Chronic disease occurs in people with long-term low-level antigen exposure (such as owners of birds) and manifests as onset over months to years of exertional dyspnea, productive cough, fatigue, and weight loss. There are few physical findings; clubbing uncommonly occurs, and fever is absent. In advanced cases, pulmonary fibrosis causes symptoms and signs of right heart failure, respiratory failure, or both.
Subacute hypersensitivity pneumonitis
Subacute disease falls between the acute and chronic forms and manifests either as cough, dyspnea, fatigue, and anorexia that develops over days to weeks or as acute symptoms superimposed on chronic ones.
Diagnosis of Hypersensitivity Pneumonitis
High-resolution CT (HRCT)
Pulmonary function tests
Bronchoalveolar lavage
Histologic examination and serologic tests
Diagnosis of hypersensitivity pneumonitis requires a high index of suspicion in patients with compatible symptoms and a compatible occupational, avocational, or domestic exposure history. Hypersensitivity pneumonitis must be considered in patients with newly identified interstitial lung disease (1). HRCT and pulmonary function tests are done routinely. Bronchoalveolar lavage and lung biopsy may be necessary if results are inconclusive. The differential diagnosis is broad and includes environmental pulmonary diseases, sarcoidosis, bronchiolitis obliterans, systemic rheumatic–associated pulmonary disease, and other interstitial lung diseases.
Clues in the history include
Recurring atypical pneumonias
Symptom onset after moving to a new job or home
A hot tub, a sauna, a swimming pool, or other sources of standing water or water damage in the home or regular exposure to them elsewhere
Having birds as pets
Exacerbation and relief of symptoms in and away from specific settings
Examination often is not useful in making the diagnosis, although abnormal lung sounds and clubbing may be present.
Imaging tests
Imaging tests are typically done for patients with appropriate history, symptoms, and signs.
Chest x-ray is neither sensitive nor specific for detecting disease and is frequently normal in patients with acute and subacute forms. It may show reticular or nodular opacities, usually when symptoms are present. Chest x-rays of patients with chronic disease are more likely to show reticular or nodular opacities in the upper lobes with reduced lung volumes and honeycombing, similar to that of idiopathic pulmonary fibrosis.

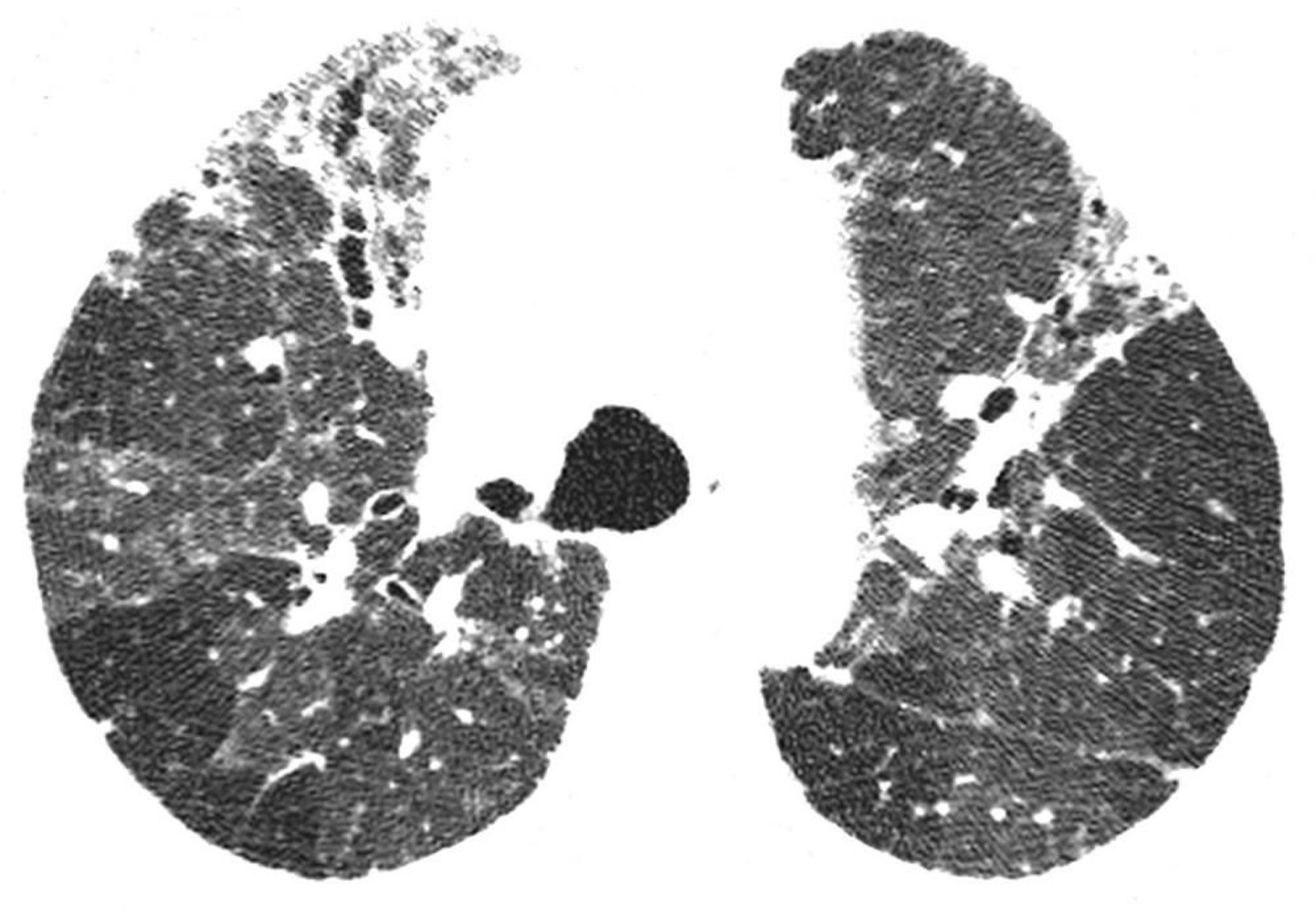
Image courtesy of Harold R. Collard, MD.
High-resolution CT is far more likely to show abnormalities and is considered standard for evaluating parenchymal changes in hypersensitivity pneumonitis. The most typical HRCT finding in acute and subacute disease is the presence of profuse, poorly defined centrilobular micronodules. Occasionally, ground-glass opacification (attenuation) is the predominant or only finding. It is usually diffuse but sometimes spares the periphery of the secondary lobule. Focal areas of hyperlucency, similar to those present in bronchiolitis obliterans, may be a prominent feature in some patients (eg, mosaic attenuation with air trapping on expiratory HRCT).
In chronic hypersensitivity pneumonitis, there are findings of lung fibrosis (eg, lobar volume loss, linear or reticular opacities, or honeycombing), and centrilobular nodules may be absent. Some nonsmoking patients with chronic hypersensitivity pneumonitis have findings of upper lobe emphysema. Mediastinal lymphadenopathy is uncommon, thereby distinguishing hypersensitivity pneumonitis from sarcoidosis.
Pulmonary function tests
Pulmonary function tests should be done as part of the standard evaluation of suspected cases of hypersensitivity pneumonitis. The syndrome can cause obstructive, restrictive, or a mixed pattern of airway changes. Advanced disease most commonly causes a restrictive defect (decreased lung volumes), a decreased diffusing capacity for carbon monoxide (DLCO), and hypoxemia. Airway obstruction is unusual in acute disease but may develop in chronic disease.
Bronchoalveolar lavage
Results of bronchoalveolar lavage are rarely specific for the hypersensitivity pneumonitis but are often a component of the diagnostic assessment for chronic respiratory symptoms and pulmonary function abnormalities. A lymphocytosis in lavage fluid (> 40%) with CD4+/CD8+ ratio < 1.0 (the normal ratio ± standard error of the mean = 2.3 ± 0.2) is characteristic of the disorder; by contrast, lymphocytosis with CD4+ predominance (ratio > 1.0) is more characteristic of sarcoidosis. Other findings may include mast cells > 1% (after acute exposure) and increased neutrophils and eosinophils.
Lymphocyte transformation testing is an in vitro test of sensitization and is particularly useful in detecting sensitization to metals. The test can be done on peripheral blood but is better done on bronchial lavage fluid. In this test, the patient's lymphocytes are exposed to potential antigens. If the lymphocytes transform into blasts and proliferate, they (and hence the patient) were previously sensitized to that antigen.
Lung biopsy
Transbronchial or surgical lung biopsy may be indicated when noninvasive testing is inconclusive. Findings vary but typically include peribronchiolar metaplasia, poorly formed non-necrotizing granulomas, and organizing pneumonia. Interstitial fibrosis may be present in chronic cases.
Other tests
Further testing is indicated when additional support for the diagnosis is required or to detect other causes of interstitial lung disease. Circulating precipitins (specific precipitating antibodies to the suspected antigen) are suggestive of an exposure that may be the cause of the illness. However, the presence of circulating precipitins is neither sensitive nor specific. Identification of a specific precipitating antigen may require that industrial hygiene specialists do detailed aerobiologic and/or microbiologic assessment of the workplace, but workplace assessments usually are guided by known sources of inciting antigens (eg, Bacillus subtilis in detergent factories).
Skin tests are not helpful, and eosinophilia is absent.
Tests helpful in detecting other disorders include serologic tests and cultures (for psittacosis and other pneumonias) and autoantibodies (for systemic rheumatic disease). Elevated eosinophil levels may suggest chronic eosinophilic pneumonias. Hilar and paratracheal lymph node enlargement is more characteristic of sarcoidosis.
Diagnosis reference
1. Raghu G, Remy-Jardin M, Ryerson CJ, et al: Diagnosis of hypersensitivity pneumonitis in adults. An Official ATS/JRS/ALAT Clinical Practice Guideline. Am J Respir Crit Care Med 202(3):e36–e69, 2020. doi: 10.1164/rccm.202005-2032ST
Treatment of Hypersensitivity Pneumonitis
Corticosteroids
Prognosis for Hypersensitivity Pneumonitis
Pathologic changes of acute hypersensitivity pneumonitis are completely reversible if detected early and if antigen exposure is eliminated. Acute disease is self-limiting with antigen avoidance; symptoms usually lessen within hours. Chronic disease has a more complicated prognosis: fibrosis is usually irreversible but may not progress if the patient is no longer exposed to the antigen.
Prevention of Hypersensitivity Pneumonitis
The most important aspect of long-term management of hypersensitivity pneumonitis is avoidance of exposure to antigens. A complete change of environment is rarely realistic, especially for farmers and other workers, in which case dust control measures (such as wetting down compost before disturbing it) or using air filters or protective masks may be effective. Fungicides may be used to prevent the growth of antigenic microorganisms (eg, in hay or on sugar cane), but the long-term safety of this approach is unknown. Extensive cleaning of wet ventilation systems, removal of moist carpets, and maintenance of low humidity are also effective in some settings. Patients must be told, however, that these measures may be inadequate if exposure continues.
Key Points
Hypersensitivity pneumonitis is a type IV hypersensitivity reaction that can be triggered with a wide variety of allergens.
In patients at risk and who have compatible symptoms, elicit a thorough history of occupational, avocational, and domestic exposure.
Do high-resolution CT and pulmonary function tests and, if the diagnosis is unclear, possibly bronchoalveolar lavage and biopsy.






