




Autoimmune hemolytic anemia is caused by autoantibodies that react with red blood cells at temperatures 37 C (warm antibody hemolytic anemia) or 37 C (cold agglutinin disease). Hemolysis is predominantly extravascular. The direct antiglobulin (direct Coombs) test establishes the diagnosis and may suggest the cause. Treatment depends on the cause and may include corticosteroids, splenectomy, IV immune globulin, immunosuppressants, avoidance of triggers (eg, cold), and withdrawal of medications.
(See also Overview of Hemolytic Anemia.)
Etiology of Autoimmune Hemolytic Anemia
Autoimmune hemolytic anemia is caused by abnormalities extrinsic to the red blood cell (RBC).
Warm antibody hemolytic anemia
Warm antibody hemolytic anemia is the most common form of autoimmune hemolytic anemia (AIHA); it is more common among females. Autoantibodies in warm antibody hemolytic anemia react at temperatures ≥ 37° C. Autoimmune hemolytic anemia may be classified as
Primary (idiopathic)
Secondary (occurring in association with an underlying disorder such as systemic lupus erythematosus (SLE), lymphoma, or chronic lymphocytic leukemia or after use of certain medications)
Medications That Cause Warm Antibody Hemolytic Anemia) stimulate production of autoantibodies against Rh antigens (methyldopa-type of autoimmune hemolytic anemia). Other medications stimulate production of autoantibodies against an antibiotic–RBC-membrane complex as part of a transient hapten mechanism; the hapten may be stable (eg, high-dose penicillin, cephalosporins) or unstable (eg, quinidine, sulfonamides).
In warm antibody hemolytic anemia, hemolysis occurs primarily in the spleen and is not due to direct lysis of RBCs. It may be severe and can be fatal. Most of the autoantibodies in warm antibody hemolytic anemia are IgG. Most are panagglutinins and have limited Rh specificity.
Cold agglutinin disease
Cold agglutinin disease (cold antibody disease) is caused by autoantibodies that react at temperatures < 37° C, but some autoantibodies have a higher thermal amplitude (eg, >30° C most likely to cause clinical manifestations). Antibody thermal amplitude is more important than its titer; the higher the temperature (ie, the closer to normal body temperature) at which these antibodies react with the RBC, the greater the hemolysis.
Causes include
Idiopathic (usually associated with a monoclonal B-cell population)
Infections, especially mycoplasmal pneumonias or infectious mononucleosis (with antibodies directed against the I [mycoplasma] or i [Epstein Barr virus] antigens)
Lymphoproliferative disorders (antibodies are usually directed against the I antigen)
Infections tend to cause acute disease, whereas idiopathic disease (the common form in older adults) tends to be chronic. The chronic hemolysis occurs largely in the extravascular mononuclear phagocyte system of the liver and spleen, but intravascular hemolysis can occur when a complement-amplifying condition, such as infection, is present. The anemia is usually mild (hemoglobin > 7.5 g/dL [70.5 g/L]). Autoantibodies in cold agglutinin disease are almost always IgM.
Paroxysmal cold hemoglobinuria
Paroxysmal cold hemoglobinuria (PCH; Donath-Landsteiner syndrome) is a rare type of cold agglutinin disease. PCH is more common in children. Hemolysis results from exposure to cold, which may even be localized (eg, from drinking cold water, from washing hands in cold water). An IgG antibody binds to the P antigen on RBCs at low temperatures and causes intravascular hemolysis and hemoglobinuria after warming. It occurs most often after a nonspecific viral illness or in otherwise healthy patients, although it occurs in some patients with congenital or acquired syphilis. The severity and rapidity of development of the anemia varies and may be fulminant. In children, this disease is often self-resolving.
Symptoms and Signs of Autoimmune Hemolytic Anemia
Symptoms of warm antibody hemolytic anemia tend to be due to the anemia. If the disorder is severe, fever, chest pain, syncope, or liver or heart failure may occur. Mild splenomegaly is typical. Venous thromboembolic events are common in patients with warm autoimmune hemolytic anemia (1).
Cold agglutinin disease manifests as an acute or chronic hemolytic anemia. Other symptoms or signs include acrocyanosis, Raynaud syndrome, cold-associated occlusive changes. Cold agglutinin disease is also associated with elevated thrombotic risk (2).
Symptoms of PCH may include severe pain in the back and legs, headache, vomiting, diarrhea, and passage of dark brown urine; hepatosplenomegaly may be present.
Symptoms and signs references
1. Audia S, Bach B, Samson M, et al. Venous thromboembolic events during warm autoimmune hemolytic anemia. PLoS One 2018;13(11):e0207218. Published 2018 Nov 8. doi:10.1371/journal.pone.0207218
2. Broome CM, Cunningham JM, Mullins M, et al. Increased risk of thrombotic events in cold agglutinin disease: A 10-year retrospective analysis. Res Pract Thromb Haemost 2020;4(4):628-635. Published 2020 Apr 9. doi:10.1002/rth2.12333
Diagnosis of Autoimmune Hemolytic Anemia
Peripheral smear, reticulocyte count, lactic dehydrogenase (LDH), haptoglobin, indirect bilirubin
Direct antiglobulin test
Thermal amplitude testing in cold agglutinin disease
Autoimmune hemolytic anemia should be suspected in any patient with a hemolytic anemia (as suggested by the presence of anemia and reticulocytosis). In warm autoimmune hemolytic anemia, the peripheral smear usually shows microspherocytes (see photo Spherocytes) and a high reticulocyte count with few or no schistocytes, indicating extravascular hemolysis. Laboratory tests typically indicate hemolysis (eg, elevated LDH and indirect bilirubin and decreased haptoglobin). A high mean corpuscular volume (MCV) may occur due to extreme reticulocytosis or agglutination in cold agglutinin disease. Hemolytic anemia in the setting of a low reticulocyte count is rare but can occur due to factors such as renal insufficiency, infection, or bone marrow failure and constitutes a medical emergency requiring prompt transfusions.
Autoimmune hemolytic anemia is diagnosed by detection of autoantibodies with the direct antiglobulin (direct Coombs) test (see figure Direct Antiglobulin Test). Antiglobulin serum is added to washed RBCs from the patient; agglutination indicates the presence of immunoglobulin or complement (C) bound to the RBCs. In warm antibody hemolytic anemia, IgG is nearly always present, and C3 (C3b and C3d) may be present as well. In cold antibody disease, C3 is present while IgG is usually absent. The test is highly sensitive for autoimmune hemolytic anemia with an estimated ~5% of AIHA cases being direct antiglobulin test-negative (1); false-negative results can occur if antibody density is very low or, rarely, if the autoantibodies are IgA.
The indirect antiglobulin (indirect Coombs) test is a complementary test that consists of mixing the patient’s plasma with normal RBCs to determine whether such antibodies are free in the plasma (see figure Indirect Antiglobulin Test). A positive result on an indirect antiglobulin test and a negative result on a direct test generally indicate an alloantibody caused by pregnancy, prior transfusions, or lectin cross-reactivity rather than immune hemolysis. Even identification of a warm antibody does not define hemolysis, because 1/10,000 healthy blood donors has a positive test result.
Once autoimmune hemolytic anemia has been identified by the antiglobulin test, testing should differentiate between warm antibody hemolytic anemia and cold agglutinin disease as well as the mechanism responsible for warm antibody hemolytic anemia. This determination can often be made by observing the pattern of the direct antiglobulin reaction. Three patterns are possible:
The reaction is positive with anti-IgG and anti-C3. This pattern is common in patients with systemic lupus erythematosus (SLE) and idiopathic AIHA, usually warm antibody hemolytic anemia, and is rare in drug-associated cases.
The reaction is positive with anti-C3 but negative with anti-IgG. This pattern occurs in cold agglutinin disease (where the antibody is most commonly an IgM). It can also occur in warm antibody hemolytic anemia when the IgG antibody is of low affinity, in some drug-associated cases, and in PCH.
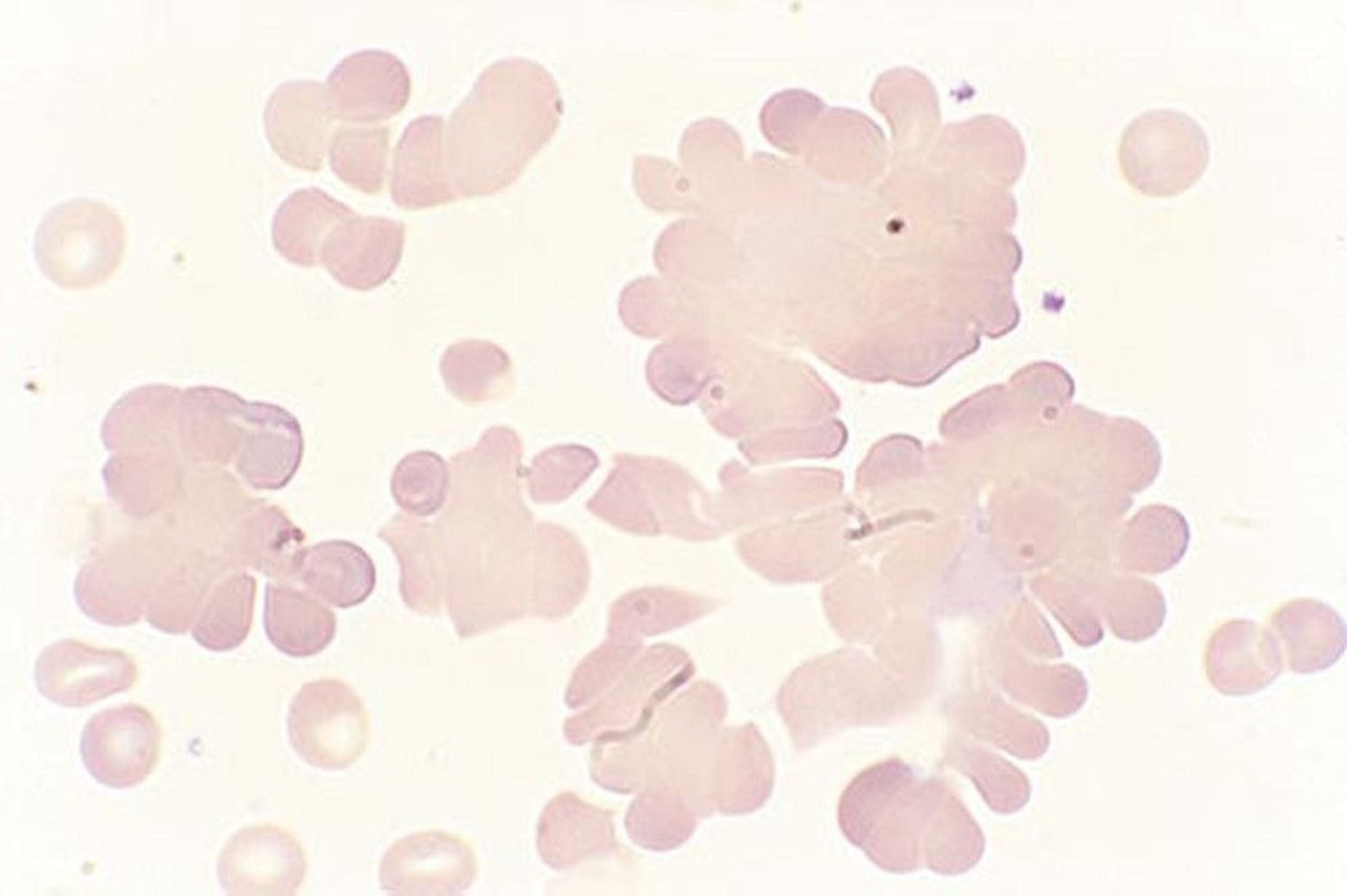
Other studies can suggest the cause of AIHA but are not definitive. In cold agglutinin disease, when unwarmed blood is used, RBCs clump on the peripheral smear, and automated cell counts often reveal an increased mean corpuscular volume and spuriously low hemoglobin due to such clumping; hand warming of the tube and recounting results in values significantly closer to normal. Warm antibody hemolytic anemia can often be differentiated from cold agglutinin disease by the temperature at which the direct antiglobulin test is positive; a test that is positive at temperatures ≥ 37° C indicates warm antibody hemolytic anemia, whereas a test that is positive at lower temperatures indicates cold agglutinin disease.
Thermal amplitude testing in cold agglutinin disease measures the temperature range in which a cold autoantibody binds to its antigen. Cold antibodies that can bind to antigen above 30° C are considered potentially clinically significant and the closer to core body temperature, the greater the chance that the antibody will cause symptoms and more significant hemolysis.

By permission of the publisher. From Tefferi A, Li C. In Atlas of Clinical Hematology. Edited by JO Armitage. Philadelphia, Current Medicine, 2004.
If paroxysmal cold hemoglobinuria (PCH) is suspected, the Donath-Landsteiner test, which is specific for PCH, should be done (2). In this test, the patient's serum is incubated with normal RBCs at 4° C for 30 minutes to allow for fixation of complement and then warmed to body temperature. Hemolysis of the RBCs during this test is indicative of PCH. Because the PCH antibody fixes complement at low temperatures, the direct antiglobulin (direct Coombs) test is positive for C3 and negative for IgG. However, the antibody in PCH is an IgG against the P antigen.
Diagnosis references
1. Sachs UJ, Röder L, Santoso S, Bein G. Does a negative direct antiglobulin test exclude warm autoimmune haemolytic anaemia? A prospective study of 504 cases. Br J Haematol 2006;132(5):655-656. doi:10.1111/j.1365-2141.2005.05955.x
2. Tiwari AK, Aggarwal G, Mitra S, et al. Applying Donath-Landsteiner test for the diagnosis of paroxysmal cold hemoglobinuria. Asian J Transfus Sci 2020;14(1):57-59. doi:10.4103/ajts.AJTS_132_17
Treatment of Autoimmune Hemolytic Anemia
Blood transfusion for severe anemia (usually with inappropriate reticulocyte response)
For drug-induced warm antibody hemolytic anemia, drug withdrawal and sometimes IV immune globulin
For cold agglutinin disease, avoidance of cold and treatment of underlying disorder
For PCH, avoidance of cold, immunosuppressants, and treatment of syphilis if present. In children, this disease is often self-resolving.
Blood transfusion is the most important treatment for patients who have symptoms and who rapidly develop severe, life-threatening anemia. In this situation, transfusion should never be withheld due to lack of "compatible" units. In general, patients who have not had a previous blood transfusion or been pregnant are at low risk for hemolysis of ABO-compatible blood. Even if transfused cells are hemolyzed, blood transfusion can be life-saving until more definitive therapy can be done. Erythropoietin may be given if the reticulocyte response is inadequate.
More specific treatment depends on the mechanism of the hemolysis.
Warm antibody hemolytic anemias
In drug-induced warm antibody hemolytic anemias,> 1 year. With hapten-mediated AIHA, hemolysis ceases when the medication is cleared from the plasma. Corticosteroids and/or infusions of immune globulin may be used as second-line therapies.
In idiopathic warm antibody AIHA,1, 2, 3
4).
The presence of panagglutinating antibodies in warm antibody hemolytic anemia makes cross-matching of donor blood difficult. In addition, transfusions could superimpose an alloantibody on the autoantibody, accelerating hemolysis. Thus, transfusions should be administered judiciously when anemia is not severe but should not be withheld in patients with severe or progressive autoimmune hemolytic anemia, particularly when the reticulocyte count is insufficient to compensate.
Because rates of venous thromboembolism are increased in patients with warm AIHA, patients should be maintained on pharmacologic prophylaxis while hospitalized.
Cold agglutinin disease
In many cases, avoidance of cold environments and other triggers of hemolysis may be all that is needed to prevent symptomatic anemia.
5). It is a treatment option in patients with severe anemia, but vaccination against infectious agents is recommended first or concurrent antimicrobial prophylaxis should be administered.
In severe cases, plasmapheresis is an effective temporary treatment. Transfusions should be given for severe anemia, with the blood warmed through an on-line warmer.
Splenectomy is usually of no value, and immunosuppressants have only modest effectiveness.
Paroxysmal cold hemoglobinuria
In paroxysmal cold hemoglobinuria (PCH), therapy consists of strict avoidance of exposure to cold. Immunosuppressants have been effective, but use should be restricted to patients with progressive or idiopathic cases.
Splenectomy is of no value.
Treatment of concomitant syphilis may cure PCH.
Treatment references
1. Abdallah GEM, Abbas WA, Elbeih EAS, Abdelmenam E, Mohammed Saleh MF. Systemic corticosteroids in the treatment of warm autoimmune hemolytic anemia: A clinical setting perspective. Blood Cells Mol Dis 2021;92:102621. doi:10.1016/j.bcmd.2021.102621
2. Birgens H, Frederiksen H, Hasselbalch HC, et alBr J Haematol 2013;163(3):393-399. doi:10.1111/bjh.12541
3. Zupańska B, Sylwestrowicz T, Pawelski S. The results of prolonged treatment of autoimmune haemolytic anaemia. Haematologia (Budap) 1981;14(4):425-433.
4. Maskal S, Al Marzooqi R, Fafaj A, et al. Clinical and surgical outcomes of splenectomy for autoimmune hemolytic anemia. Surg Endosc 2022;36(8):5863-5872. doi:10.1007/s00464-022-09116-x
5. Roth A, Barcellini W, D'Sa S, et al: Sutimlimab in cold agglutinin disease. N Engl J Med 384(14):1323–1334, 2021. doi: 10.1056/NEJMoa2027760
Key Points
Autoimmune hemolytic anemia is divided into warm antibody hemolytic anemia and cold agglutinin disease based on the temperature at which the autoantibodies react with red blood cells (RBCs).
Hemolysis tends to be more severe in warm antibody hemolytic anemia and can be fatal if reticulocytopenia is also present.
Immunoglobulin and/or complement bound to the patient's RBCs is demonstrated by the occurrence of agglutination after antiglobulin serum is added to washed RBCs (positive direct antiglobulin test).
The pattern of the direct antiglobulin reaction can help distinguish warm antibody hemolytic anemia from cold agglutinin disease.
Treatment is directed at the cause (including stopping medications, avoiding cold, treating the underlying disorder).
Corticosteroids remain the first-line treatment for idiopathic warm antibody hemolytic disease.






