


Pain is an unpleasant sensation signaling actual or possible injury.
Pain is the most common reason people seek medical care.
Pain may be sharp or dull, intermittent or constant, or throbbing or steady. Sometimes pain is very difficult to describe. Pain may be felt at a single site or over a large area. The intensity of pain can vary from mild to intolerable.
People differ remarkably in their ability to tolerate pain. One person has difficulty tolerating the pain of a small cut or bruise, but another person can tolerate pain caused by a major accident or knife wound. The ability to withstand pain varies according to mood, personality, and circumstance. In a moment of excitement during an athletic match, an athlete may not notice a severe bruise but is likely to be very aware of the pain after the match, particularly if the team lost.
Spotlight on Aging: Pain
Conditions that cause pain are common among older people. However, as people age, they complain less of pain. The reason may be a decrease in the body’s sensitivity to pain or a more stoical attitude toward pain. Some older people mistakenly think that pain is an unavoidable part of aging and thus minimize it or do not report it. The most common cause of pain is a musculoskeletal disorder. However, many older people have chronic pain, which may have many causes. Effects of pain may be more serious for older people:
Older People and Pain Relievers Older people are more likely than younger people to have side effects from pain relievers (analgesics), and some side effects are more likely to be severe. Analgesics may stay in the body longer, and older people may be more sensitive to them. Many older people take several drugs, increasing the chances that a drug will interact with the analgesic. Such interactions may reduce the effectiveness of one of the drugs or increase the risk of side effects. Older people are more likely to have health problems that increase the risk of side effects from analgesics. Nonsteroidal anti-inflammatory drugs (NSAIDs) NSAIDs can damage the kidneys. This risk is higher for older people because the kidneys tend to function less well as people age. This risk of kidney damage is also higher in people with a kidney disorder, heart failure, or a liver disorder, which are more common among older people. Older people are more likely to develop ulcers or bleeding in the digestive tract when they take NSAIDs. Doctors may prescribe a drug that helps protect the digestive tract from such damage. These drugs include proton pump inhibitors When older people take NSAIDs, they should tell their doctor, who then evaluates them periodically for side effects. Doctors also recommend the following for older people if possible:
Opioids are more likely to cause problems in older people, who appear to be more sensitive to these drugs than younger people. When some older people take an opioid for a short time, it reduces pain and enables them to function better physically, but it may impair mental functioning, sometimes causing confusion. Opioids also increase the risk of falls, and taking opioids for a long time can increase the risk of osteoporosis and fractures. Opioids cause constipation and urinary retention, which tend to cause more problems in older people. Older people are more likely to have conditions or take drugs that can make them more likely to have side effects from opioids, such as the following:
Opioids may also cause dependence and addiction. Doctors usually treat pain with analgesics less likely to have side effects in older people. For example, Nondrug treatments and support from caregivers and family members can sometimes help older people manage pain and reduce the need for analgesics. |
Pain pathways
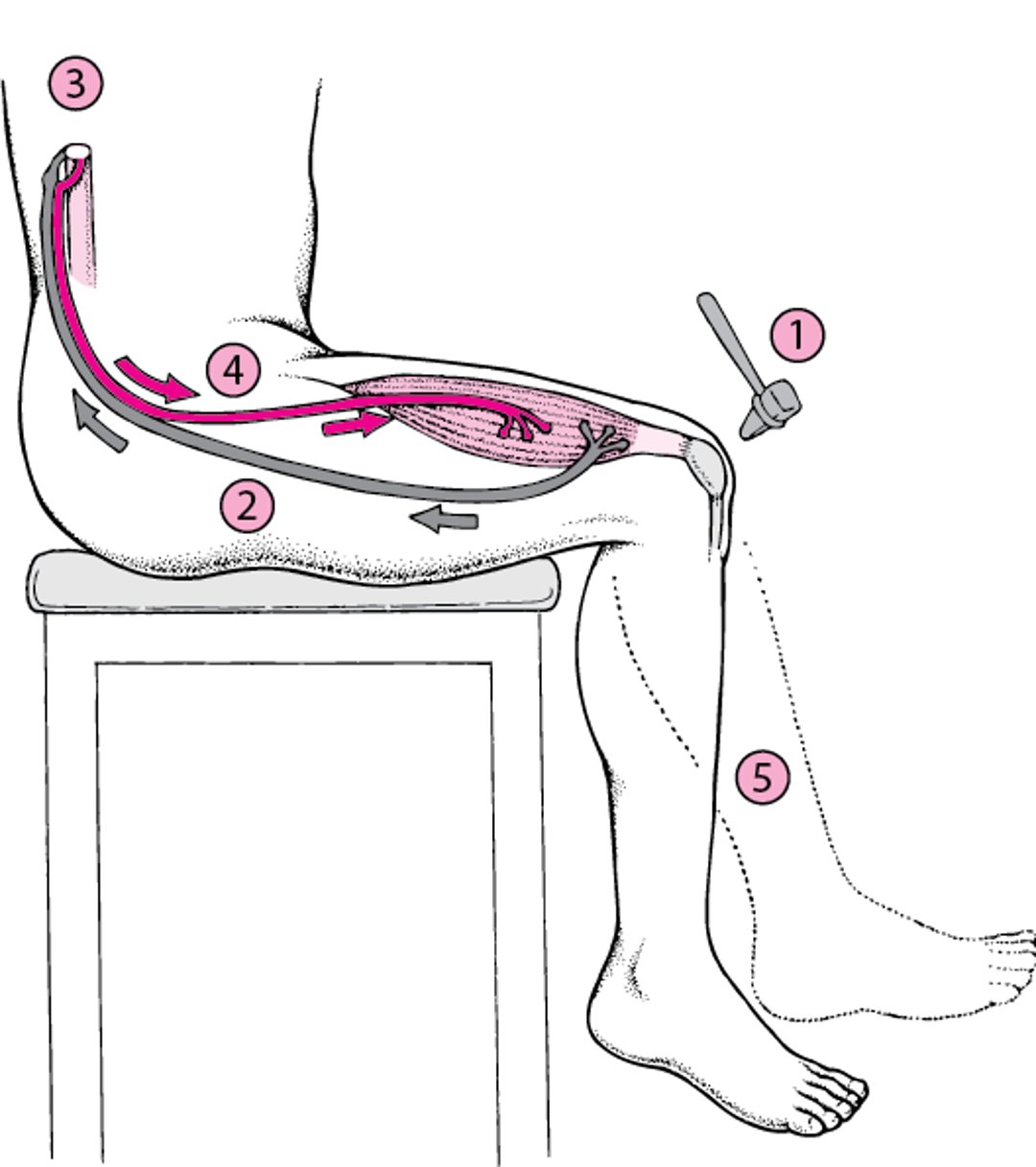
Pain due to injury begins at special pain receptors scattered throughout the body. These pain receptors transmit signals as electrical impulses along nerves to the spinal cord and then upward to the brain. Sometimes the signal evokes a reflex response (see figure Reflex Arc: A No-Brainer). When the signal reaches the spinal cord, a signal is immediately sent back along motor nerves to the original site of the pain, triggering the muscles to contract without involving the brain. For example, when people inadvertently touch something very hot, they immediately pull away. This reflex reaction helps prevent permanent damage. The pain signal is also sent to the brain. Only when the brain processes the signal and interprets it as pain do people become aware of the pain.
Pain receptors and their nerve pathways differ in different parts of the body. For this reason, pain sensation varies with the type and location of injury. For example, pain receptors in the skin are plentiful and capable of transmitting precise information, including where an injury is located and whether the source was sharp, such as a knife wound, or dull, such as pressure, heat, cold, or itching. In contrast, pain receptors in internal organs, such as the intestine are limited and imprecise. The intestine can be pinched, cut, or burned without generating a pain signal. However, stretching and pressure can cause severe intestinal pain, even from something as relatively harmless as a trapped gas bubble. The brain cannot identify the precise source of intestinal pain, which is difficult to locate and is likely to be felt over a large area.
Reflex Arc: A No-Brainer
A reflex arc is the pathway that a nerve reflex, such as the knee jerk reflex, follows.
|

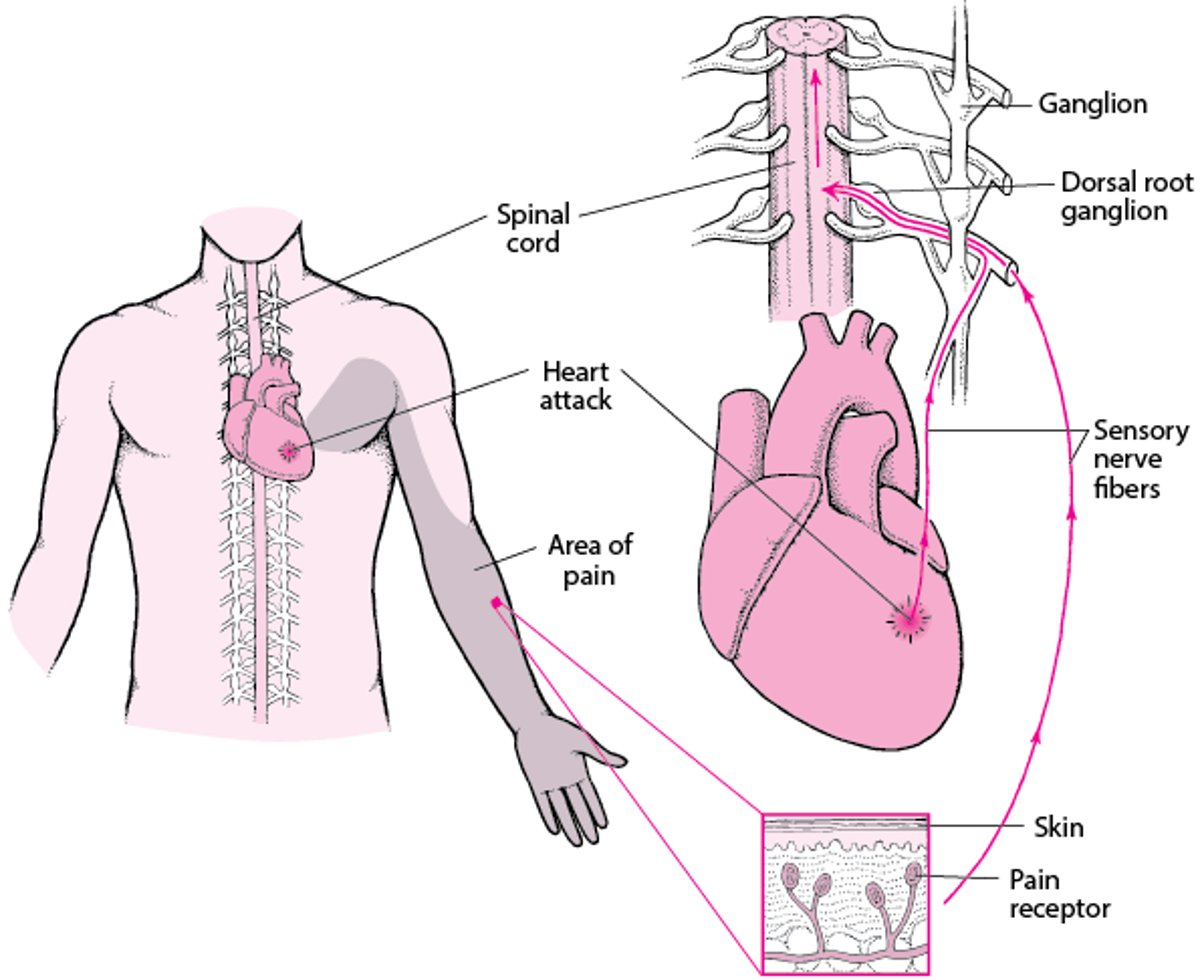
Sometimes pain felt in one area of the body does not accurately represent where the problem is because the pain is referred there from another area. Pain can be referred because signals from several areas of the body often travel through the same nerve pathways in the spinal cord and brain. For example, pain from a heart attack may be felt in the neck, jaws, arms, or abdomen. Pain from a gallbladder attack may be felt in the back of the shoulder.
What Is Referred Pain?
Pain felt in one area of the body does not always represent where the problem is because the pain may be referred there from another area. For example, pain produced by a heart attack may feel as if it is coming from the arm because sensory information from the heart and the arm converge on the same nerve pathways in the spinal cord. |

Acute versus chronic pain
Pain may be acute or chronic. Acute pain means pain that begins suddenly and does not last long (days or weeks). Chronic pain lasts for many months or years.
When severe, acute pain may cause anxiety, a rapid heart rate, an increased breathing rate, elevated blood pressure, sweating, and dilated pupils. Usually, chronic pain does not have these effects, but it may result in other problems, such as depression, disturbed sleep, decreased energy, a poor appetite, weight loss, decreased sex drive, and loss of interest in activities.
Causes of Pain
Different types of pain have different causes.
Nociceptive pain results from stimulation of pain receptors. It is caused by an injury to body tissues. Most pain, particularly acute pain, is nociceptive pain.
Neuropathic pain results from damage to or dysfunction of the brain or spinal cord (central nervous system) or the nerves outside the brain and spinal cord (peripheral nervous system). It may occur when
Pressure is put on a specific nerve—for example, by a tumor or a ruptured disk in the spine, causing low back pain and/or pain radiating down the leg. Pressure on a nerve in the wrist can cause carpal tunnel syndrome.
Nerves are damaged, as occurs in diabetes mellitus or postherpetic neuralgia (pain after shingles).
The brain and spinal cord do not process pain signals normally or something disrupts this processing, as occurs in phantom limb pain and complex regional pain syndrome.
In diabetes, nerves outside the brain and spinal cord (peripheral nerves) are damaged. Symptoms include numbness, tingling, and pain in the toes, feet, and sometimes hands.
In postherpetic neuralgia, the area where the rash first occurred becomes painful and tender to the touch.
Nociceptive or neuropathic pain or both may be involved in acute or chronic pain. For example, chronic low back pain and most cancer pain are caused mainly by ongoing stimulation of pain receptors (nociceptive pain). But in these disorders, pain can also result from nerve damage (neuropathic pain).
Psychologic factors, such as depression, can also contribute to pain. Psychologic factors often affect how people feel pain and how intense it seems, but these factors are rarely the only cause of pain.
Evaluation of Pain
To evaluate a person with pain, doctors ask the person about the history and characteristics of the pain and its effect on how well the person can function. The person’s answers help them identify the cause and develop a treatment strategy. Questions can include the following:
Where is the pain?
What is the pain like (for example, is it sharp, dull, crampy)?
When did the pain start? Was there any injury?
How did the pain start? Did it begin suddenly or gradually?
Is the pain always present, or does it come and go?
Does it occur predictably after certain activities (such as meals or physical exertion) or in certain body positions? What else makes the pain worse?
What, if anything, helps relieve the pain?
Does pain affect the ability to do daily activities or to interact with other people? Does it affect sleep, appetite, and bowel and bladder function? If so, how?
Does pain affect mood and sense of well-being? Is the pain accompanied by feelings of depression or anxiety?
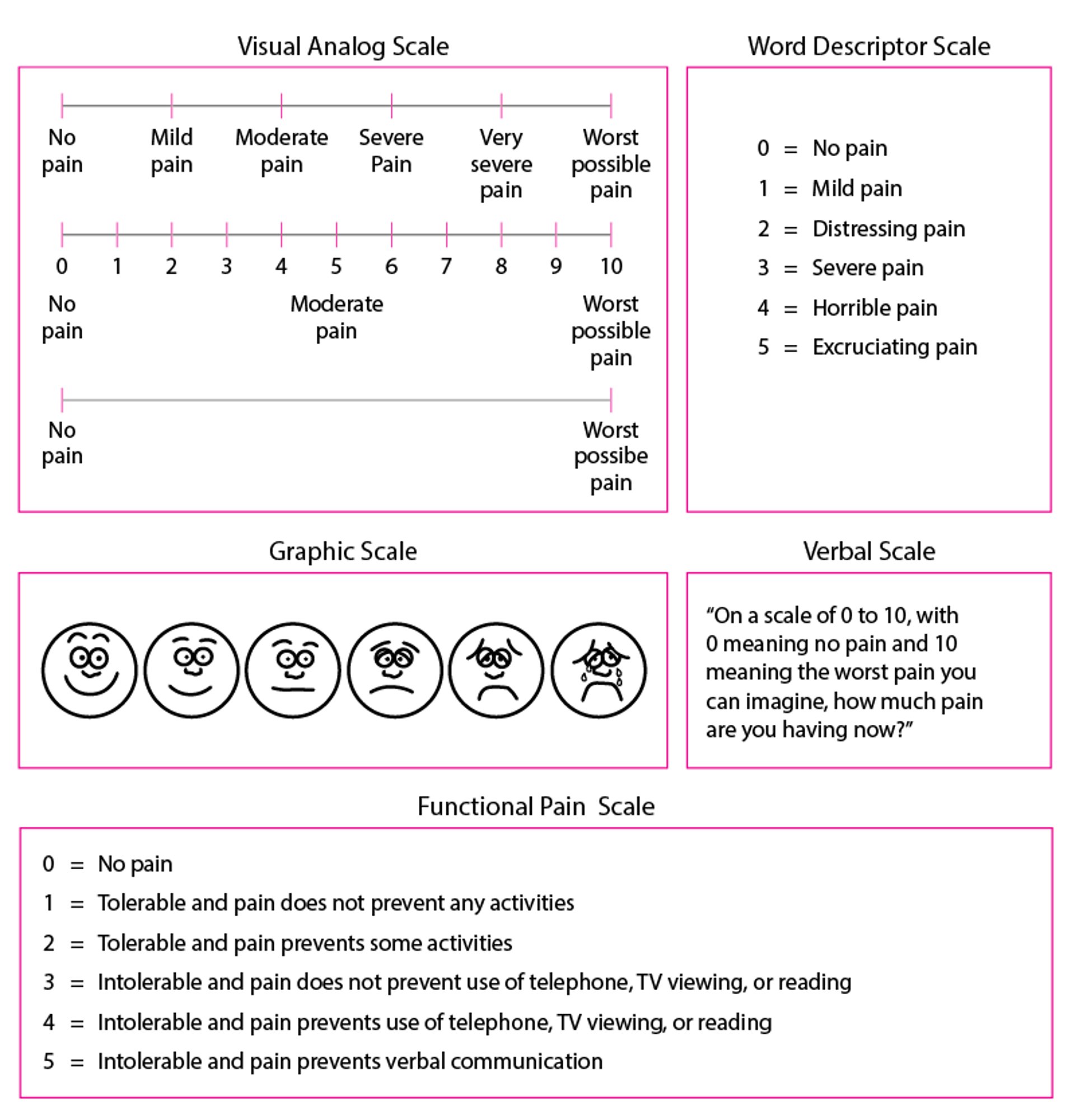
To evaluate the severity of pain, doctors sometimes use a scale of 0 (none) to 10 (severe) or ask the person to describe the pain as mild, moderate, severe, or excruciating. For children or for people who have difficulty communicating (for example, because of a stroke), drawings of faces in a series—from smiling to frowning and crying—can be used to determine the severity of pain.
Pain Scales: How Bad Is the Pain?
Because severity of pain is difficult to communicate, doctors often use a pain scale to help people indicate how severe the pain is. |

Doctors always try to determine whether a physical disorder is causing the pain. Many chronic disorders (such as cancer, arthritis, sickle cell anemia, and inflammatory bowel disease) cause pain, as do acute disorders (such as wounds, burns, torn muscles, broken bones, sprained ligaments, appendicitis, kidney stones, and a heart attack).
Doctors use specific techniques to check for sources of pain. Doctors move the person’s arms and legs through their normal range of motion to see if these motions cause pain. Injury, repetitive stress, chronic pain, and other disorders can make certain areas of the body (called trigger points) become hypersensitive. Doctors touch various spots to see whether they are trigger points for pain. Different objects (such as a blunt key and a sharp pin) may be touched to the skin to check for loss of sensation or abnormal perceptions.
Doctors also consider emotional or mental health causes. Mental health conditions (such as depression and anxiety) can worsen pain. Because depression and anxiety may result from chronic pain, distinguishing cause and effect may be difficult. Sometimes in people with pain, there is evidence of psychologic disturbances but no evidence of a disorder that could account for the pain or its severity. Such pain is called psychogenic or psychophysiologic pain.
Doctors ask about which drugs (including over-the-counter drugs) and other treatments the person has used to treat the pain and whether they are effective. If misuse of opioids or other substances is suspected, further evaluation is required.







