

Women may have infertility if the ovaries do not release an egg each month, as usually occurs during a menstrual cycle.
Ovulation may not occur at all or may occur irregularly if certain hormones are not released from the brain or ovaries in a typical monthly pattern.
Women can determine whether ovulation is occurring and estimate when it occurs by measuring body temperature or using home ovulation prediction kits.
Doctors use ultrasonography or blood or urine tests to evaluate ovulation problems.
Medications, usually clomiphene or letrozole, can be used to stimulate ovulation.Medications, usually clomiphene or letrozole, can be used to stimulate ovulation.
(See also Overview of Infertility.)
Ovulation is the release of an egg from the ovary. This usually occurs in the middle of the menstrual cycle. A normal cycle occurs every 24 to 38 days. A problem with ovulation is a common cause of infertility in women.
Causes of Ovulation Problems
The female reproductive system is controlled by hormones produced by areas of the brain, including the hypothalamus (an area of the brain that coordinates and controls hormonal activity) and the pituitary gland, and by the ovaries. The hormonal interactions that control ovulation and menstruation occur in the following sequence:
Gonadotropin-releasing hormone (GnRH) is released from the hypothalamus.
The pituitary gland (also located in the brain) is stimulated by GnRH.
Luteinizing hormone (LH) and follicle-stimulating hormone (FSH) are released by the pituitary gland.
The ovaries are stimulated by LH and FSH, the hormones that control ovulation.
The ovaries produce the female hormones estrogen and progesteroneprogesterone, which control menstruation.
Problems with ovulation (release of an egg) result when one part of this system does not function properly. Ovulation can be affected if any of these steps or hormones are not normal. Ovulation may also be affected by abnormalities in other hormonal glands, such as the adrenal glands or thyroid gland.
Problems with ovulation may be due to many disorders.
The most common cause of chronic ovulation problems is
Polycystic ovary syndrome, which usually causes irregular periods and often also causes excess weight gain, acne, and/or excess body hair (due to excess production of male hormones by the ovaries)
Other causes of ovulation problems include
Excessive exercise
Certain medications (including estrogens and progestins and certain antidepressants)
Excessive weight loss
Rarely, the cause is premature menopause—when the supply of eggs in the ovaries is low at a younger than average age (the average age of menopause is 51 years old).
Women with an ovulation problem may have no periods (amenorrhea) or irregular bleeding, called abnormal uterine bleeding.
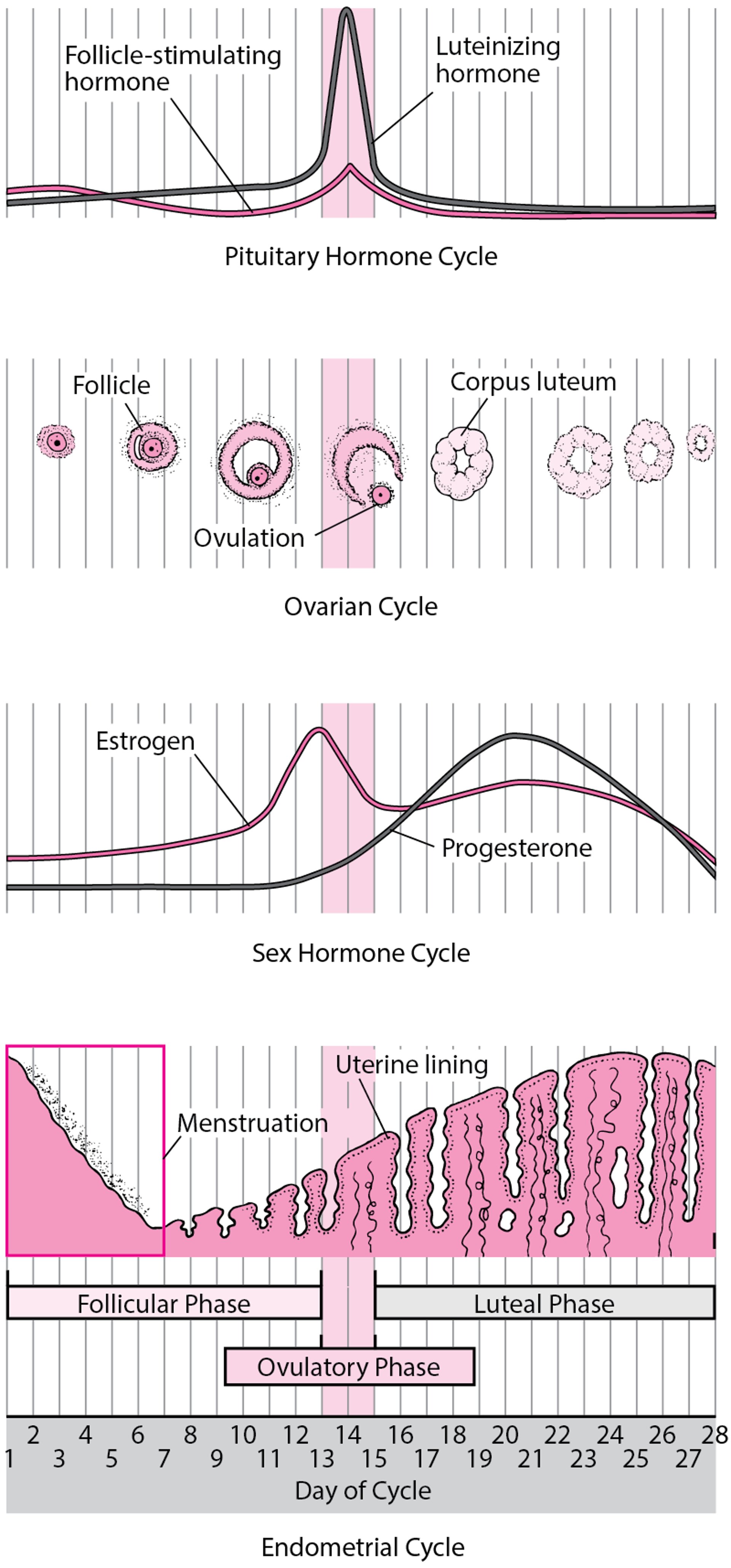
Changes During the Menstrual Cycle
The menstrual cycle is regulated by the complex interaction of hormones: luteinizing hormone, follicle-stimulating hormone, and the female sex hormones estrogen and progesterone. The menstrual cycle has three phases:
The menstrual cycle begins with menstrual bleeding (menstruation), which marks the first day of the follicular phase. When the follicular phase begins, levels of estrogen and progesterone are low. As a result, the top layers of the thickened lining of the uterus (endometrium) break down and are shed, and menstrual bleeding occurs. About this time, the follicle-stimulating hormone level increases slightly, stimulating the development of several follicles in the ovaries. Each follicle contains an egg. Later in this phase, as the follicle-stimulating hormone level decreases, only one follicle continues to develop. This follicle produces estrogen. As the follicular phase continues, the increasing levels of estrogen cause the lining of the uterus to thicken. The ovulatory phase begins with a surge in luteinizing hormone and follicle-stimulating hormone levels. Luteinizing hormone stimulates egg release (ovulation), which usually occurs 32 to 36 hours after the surge begins. The estrogen level peaks during the surge, and the progesterone level starts to increase. During the luteal phase, luteinizing hormone and follicle-stimulating hormone levels decrease. The ruptured follicle closes after releasing the egg and forms a corpus luteum, which produces progesterone. During most of this phase, the estrogen level is high. Progesterone and estrogen cause the lining of the uterus to thicken more and thus prepare for possible fertilization. If the egg is not fertilized, the corpus luteum degenerates and no longer produces progesterone, the estrogen level decreases, the top layers of the lining break down and are shed, and menstrual bleeding occurs (the start of a new menstrual cycle). |

Diagnosis of Ovulation Problems
A record of the timing of menstrual periods
A home ovulation prediction kit
Sometimes daily measurement of body temperature
Ultrasonography
Blood or urine tests
Doctors ask women to describe their menstrual periods (menstrual history), including how often periods occur and how long they last. Based on this information, doctors may be able to determine whether women are ovulating.
The most accurate method that can be done at home is with an ovulation prediction kit, but they are not 100% accurate so some ovulations may be missed. This kit detects an increase in luteinizing hormone in the urine 24 to 36 hours before ovulation. To provide a more accurate result, some kits also measure by-products of estrogen. Urine is tested on several consecutive days during the middle of the menstrual cycle.
Another method to determine if or when ovulation is occurring is for a woman to take her temperature at rest (basal body temperature) each day. Usually, the best time is immediately after awakening and before getting out of bed. A decrease in basal body temperature suggests that ovulation is about to occur. If possible, she should use a basal body temperature thermometer designed for women who are trying to become pregnant, or a digital or mercury thermometer can be used. An increase of 0.9° F (0.5° C) or more in temperature usually indicates that ovulation has just occurred. However, this method is time-consuming and is not reliable or precise.
Doctors can accurately determine whether and when ovulation occurs. Methods include
Ultrasonography
Measurement of the level of progesterone in the blood or the level of one of its by-products in the urine
A marked increase in levels of progesterone or its by-products indicates that ovulation has occurred.
Doctors may do other tests to check for disorders that can cause ovulation problems. For example, they may measure testosterone levels in the blood to check for polycystic ovary syndrome.
Treatment of Ovulation Problems
Treatment of the cause, if identified
A medication to stimulate ovulation
Underlying disorders (such as polycystic ovary syndrome or too much prolactin), if identified, are treated.
A medication, such as letrozole, clomiphene, or human gonadotropins, can usually stimulate ovulation. The particular medication is selected based on the specific problem. If the cause of infertility is A medication, such as letrozole, clomiphene, or human gonadotropins, can usually stimulate ovulation. The particular medication is selected based on the specific problem. If the cause of infertility ispremature menopause, neither clomiphene nor human gonadotropins can stimulate ovulation., neither clomiphene nor human gonadotropins can stimulate ovulation.
Letrozole
Letrozole is often the first choice of medication used to stimulate ovulation, as Letrozole is often the first choice of medication used to stimulate ovulation, asletrozole has fewer side effects than clomiphene, another commonly used fertility medication. The most common side effects of has fewer side effects than clomiphene, another commonly used fertility medication. The most common side effects ofletrozole are fatigue and dizziness.
Letrozole is an aromatase inhibitor. Aromatase inhibitors block the production of estrogen. They are also used to treat breast cancer in women who have gone through menopause.
For women with polycystic ovary syndrome and obesity, letrozole is more likely to stimulate ovulation than clomiphene. For other women, research has not shown that is more likely to stimulate ovulation than clomiphene. For other women, research has not shown thatletrozole is more effective than clomiphene.
Letrozole is started a few days after menstrual bleeding begins, and women take it by mouth for 5 days. If ovulation does not occur, a higher dose is used in each cycle until ovulation occurs or the maximum dose is reached.Letrozole is started a few days after menstrual bleeding begins, and women take it by mouth for 5 days. If ovulation does not occur, a higher dose is used in each cycle until ovulation occurs or the maximum dose is reached.
Letrozole is used only after a pregnancy test is negative because birth defects may result when it is used early in pregnancy.
Clomiphene
Another medication doctors may use is clomiphene. Clomiphene is most effective when the cause of ovulation problems is polycystic ovary syndrome.
A few days after menstrual bleeding begins, a woman takes clomiphene by mouth for 5 days. Before the medication is started, a woman usually needs to be given hormones to induce menstrual bleeding. Usually, she ovulates 5 to 10 days after clomiphene is stopped, and she has a menstrual period 14 to 16 days after ovulation.A few days after menstrual bleeding begins, a woman takes clomiphene by mouth for 5 days. Before the medication is started, a woman usually needs to be given hormones to induce menstrual bleeding. Usually, she ovulates 5 to 10 days after clomiphene is stopped, and she has a menstrual period 14 to 16 days after ovulation.
If a woman does not have a period after treatment with clomiphene, she takes a pregnancy test. If she is not pregnant, the treatment cycle is repeated. A higher dose of clomiphene is used in each cycle until ovulation occurs or the maximum dose is reached. When the dose that stimulates ovulation is determined, a woman takes that dose for up to 4 more treatment cycles. Most women who become pregnant do so by the fourth cycle in which ovulation occurs. Although about 75 to 80% of women treated with clomiphene ovulate, only about 40 to 50% of those who ovulate become pregnant. About 5% of pregnancies in women treated with clomiphene involve more than 1 fetus (multiple gestation), usually twins.
Side effects of clomiphene include hot flashes, abdominal bloating, breast tenderness, nausea, vision problems, and headaches.
Ovarian hyperstimulation syndrome occurs in fewer than 1% of women treated with clomiphene. In this syndrome, the ovaries enlarge greatly and a large amount of fluid moves out the bloodstream into the abdomen. This syndrome may be life threatening. To try to prevent it, doctors prescribe the lowest effective dose of clomiphene, and if the ovaries enlarge, they stop the medication.
Clomiphene is used only after a pregnancy test is negative because birth defects may result if it is used early in pregnancy.
Metformin
Doctors may treat some women with metformin (a medication also used to treat people with diabetes) to stimulate ovulation. Metformin is often used for women with Doctors may treat some women with metformin (a medication also used to treat people with diabetes) to stimulate ovulation. Metformin is often used for women withpolycystic ovary syndrome, especially for those who also have obesity (with a body mass index of 30 or higher) and/or diabetes or prediabetes (blood sugar levels that are high but not high enough to be labeled diabetes). However, even in these women, clomiphene is usually more effective than or prediabetes (blood sugar levels that are high but not high enough to be labeled diabetes). However, even in these women, clomiphene is usually more effective thanmetformin and just as effective as metformin plus clomiphene for stimulating ovulation.
Human gonadotropins
If a woman does not ovulate or become pregnant during treatment with clomiphene or letrozole, hormone therapy with human gonadotropins, injected into a muscle or under the skin, can be tried. Human gonadotropins contain follicle-stimulating hormone and sometimes luteinizing hormone. These hormones stimulate the follicles of the ovaries to mature and thus make ovulation possible. If a woman does not ovulate or become pregnant during treatment with clomiphene or letrozole, hormone therapy with human gonadotropins, injected into a muscle or under the skin, can be tried. Human gonadotropins contain follicle-stimulating hormone and sometimes luteinizing hormone. These hormones stimulate the follicles of the ovaries to mature and thus make ovulation possible.Follicles are fluid-filled cavities, each of which contains an egg. Ultrasonography can detect when the follicles are mature.
When the follicles are mature, a woman is given an injection of a different hormone, human chorionic gonadotropin, to stimulate ovulation. Human chorionic gonadotropin is produced during pregnancy and is similar to luteinizing hormone, which is normally released in the middle of the menstrual cycle. Or, a gonadotropin-releasing hormone (GnRH) agonist can be used to stimulate ovulation, especially in women at high risk of ovarian hyperstimulation syndrome. GnRH agonists are synthetic forms of a hormone produced by the body (GnRH).
When human gonadotropins are used appropriately, more than 95% of women treated with them ovulate, but only approximately 50% of those who ovulate become pregnant. About 10 to 30% of pregnancies in women treated with human gonadotropins involve more than 1 fetus, primarily twins.
Human gonadotropins are expensive and can have severe side effects, so doctors closely monitor a woman during treatment. About 10 to 20% of women treated with human gonadotropins develop moderate to severe ovarian hyperstimulation syndrome.
If a woman has a high risk of having more than 1 fetus or of developing ovarian hyperstimulation syndrome, it is safer not to use a medication to stimulate ovulation. However, if it is necessary to stimulate ovulation, using a GnRH agonist is safer than using human chorionic gonadotropin.
Other medications
If the hypothalamus does not secrete gonadotropin-releasing hormone, a synthetic version of this hormone (called gonadorelin acetate), given intravenously, may be useful. This medication, like the natural hormone, stimulates the pituitary gland to produce the hormones that stimulate ovulation. The risk of ovarian hyperstimulation is low with this treatment, so close monitoring is not needed. However, this medication is not available in the United States.
Drug Information for the Topic





