



The term temporomandibular disorders is an umbrella term for a group of musculoskeletal and neuromuscular conditions that involve the temporomandibular joint (TMJ), the masticatory muscles (eg, temporalis, masseter, and pterygoids), and the surrounding nerves and ligaments. Temporomandibular disorders (previously known as temporomandibular joint dysfunction or temporomandibular joint [TMJ] syndrome) often present with pain in the jaw, face, and neck and/or with dysfunction of the jaw joint (often joint sounds and/or a decreased range of motion) that is often accompanied by other comorbidities including headache or ear pain. People are considered to have a temporomandibular disorder (TMD) when the pain or dysfunction is severe enough to make them seek professional care.
Temporomandibular disorders typically are multifactorial in origin, but most are related to problems with masticatory muscles and ligaments of the temporomandibular joints or internal derangements within the joints themselves. Joint hypermobility (laxity) can also contribute.
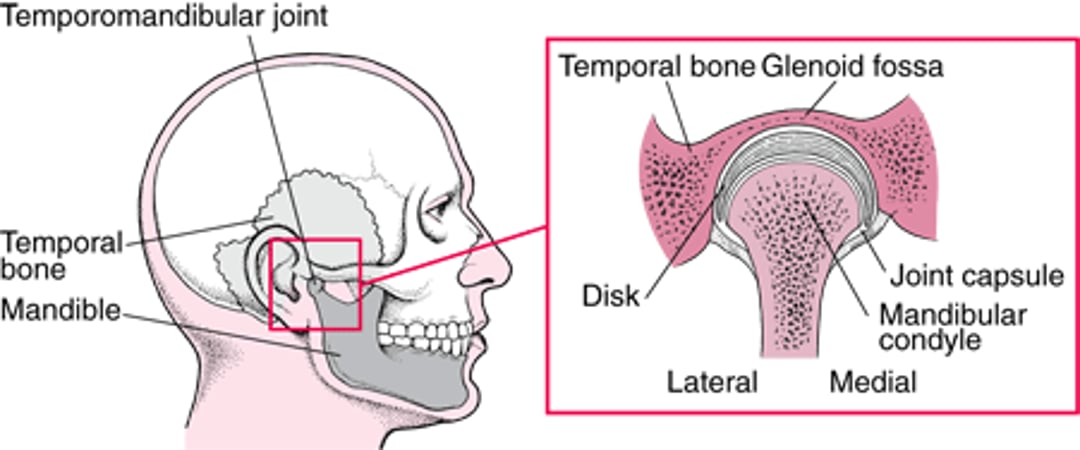
Internal derangements of the TMJ are a result of altered or disturbed movement of the condyle in the glenoid fossa or against the articular disc (see figure ). The disc, which is composed of dense fibrous connective tissue and shaped like a mature red blood cell, serves as a cushion between the bone surfaces. Unlike most joints, which are lined with hyaline cartilage, the TMJ bone surfaces are lined with fibrocartilage. Causes for the altered or disturbed movement include direct or indirect macrotrauma (eg, flexion-extension injury of the neck—also known as whiplash—which can cause referred pain), microtrauma (eg, due to parafunctional behaviors such as awake/sleep clenching and grinding of the teeth and/or bracing or thrusting of the mandible or persistent gum chewing), systemic disorders (eg, rheumatoid arthritis, juvenile idiopathic arthritis), local or systemic infections, and acute malocclusion (eg, from blunt trauma).
(See also Mandibular Dislocation, Temporal Bone Fractures and Jaw Tumors.)
The Temporomandibular Joint
The joint is formed by the mandibular condyle and the glenoid fossa of the temporal bone; a fibrocartilaginous articular disc functions as a cushion between the joint surfaces. |

Diagnosis of Temporomandibular Disorders
Primarily history and physical examination
Sometimes imaging
Disorders of the temporomandibular joint (TMJ) must be distinguished from the many conditions that mimic them (see table ). Pain exacerbated by finger pressure on the joint when the mouth is opened implicates a TMJ disorder.
Some Conditions That Mimic Temporomandibular Disorders
Symptom | Condition |
|---|---|
Headaches | Giant cell (temporal) arteritis Tension and migraine headaches, and trigeminal autonomic cephalalgias (eg, cluster headaches) Parafunctional behavior (eg, bruxism) causing muscle tension/pain in the temporalis and masseter regions Referred pain originating from neck disorders |
Pain | Postherpetic neuralgia Complex regional pain syndrome type I (formerly reflex sympathetic dystrophy) or traumatic neuroma after head or neck surgery Head and neck trauma Cardiac pain Salivary gland disorders |
Pain accompanied by hearing problems | Obstruction of the ear canals or eustachian tubes |
Pain in the head, neck, and other areas of the body | Myofascial pain syndrome |
Pain, numbness | Metastatic tumors |
Pain that radiates to the temporomandibular joint region | Flexion/extension (whiplash) injuries affecting muscle or cervical spine |
Pain that worsens when the patient swallows or turns the head | Cervical spine or muscle disorders Eagle syndrome (calcified stylohyoid ligament or an elongated styloid process) |
Trismus | Depressed fracture of the zygomatic arch Odontogenic infections Osteochondroma of the coronoid process Pericoronitis Tetanus |
Patients are asked to describe the pain and identify painful areas. Typically, muscles of mastication (temporalis, masseter, and medial pterygoids) and the cervical and occipital muscles are palpated for general tenderness and trigger points (hyperirritable spots that when palpated cause referred pain to another area). The lateral pterygoids cannot be directly palpated.
Patients are observed opening the mouth as wide as is comfortable. When patients open their mouth, the mandible typically deviates toward the painful side. Auscultation with a stethoscope and palpation of the joint during opening and closing may reveal tenderness and catching often accompanied by intracapsular sounds such as clicking, popping, or crepitus.
Condylar motion can best be palpated by bilaterally placing the middle fingers on the preauricular areas (lateral poles of the condyle) and exerting gentle medial pressure or by placing the 5th fingers into the external ear canals and exerting very gentle forward pressure as patients move their jaw. The average-sized patient can open the mouth at least 40 mm (measured between the incisal edges of the upper and lower central incisors). To account for differences in patient size, a patient should typically be able to fit their 3 fingers (second, third, and fourth) vertically into the mouth up to the distal interphalangeal joints.
Imaging is usually not needed to establish the diagnosis, but may be performed in cases of diagnostic uncertainty or when it is necessary to confirm intraarticular pathology (eg, disc displacement, degenerative joint disease) (1).
Diagnosis reference
1. Schiffman E, Ohrbach R. Executive summary of the Diagnostic Criteria for Temporomandibular Disorders for clinical and research applications. J Am Dent Assoc. 2016;147(6):438-445. doi:10.1016/j.adaj.2016.01.007





