



Necrotizing soft-tissue infection is typically caused by a mixture of aerobic and anaerobic organisms that cause necrosis of subcutaneous tissue, usually including the fascia. This infection most commonly affects the extremities and perineum. Affected tissues become erythematous, warm, and swollen, resembling severe cellulitis, and pain develops out of proportion to clinical findings. During surgical exploration, there is a gray exudate, friable superficial fascia, and absence of pus. Without timely treatment, the area becomes gangrenous. Patients are acutely ill. Diagnosis is by history and examination and is supported by evidence of overwhelming infection. Treatment involves antibiotics and surgical debridement. Prognosis is poor without early, aggressive treatment.
Necrotizing soft-tissue infection (NSTI) is a severe, rapidly spreading bacterial infection that is often polymicrobial (aerobic and/or anaerobic) but sometimes monomicrobial (eg, streptococcal). It causes extensive necrosis of the subcutaneous tissues and fascia. NSTIs frequently arise from bacterial invasion after a breach in skin integrity; however, in approximately 20% of cases, no identifiable portal of entry is found (1).
In one meta-analysis, the overall global mortality rate due to NSTI was 23.1% and did not vary by region (2).
Innate (eg, HLA DQA1 allele) and/or acquired patient factors (eg, diabetes mellitus, immunosuppression, chronic kidney disease, cancer, alcohol use disorder, injection drug use) can contribute to the development of NSTI in some patients (3). (See also Overview of Bacterial Skin Infections.)
General references
1. Stevens DL, Bryant AE. Necrotizing Soft-Tissue Infections. N Engl J Med. 2017;377(23):2253-2265. doi:10.1056/NEJMra1600673
2. Dhanasekara CS, Marschke B, Morris E, Kahathuduwa CN, Dissanaike S. Global patterns of necrotizing soft tissue infections: A systematic review and meta-analysis. Surgery. 2021;170(6):1718-1726. doi:10.1016/j.surg.2021.06.036
3. Hua C, Urbina T, Bosc R, et al. Necrotising soft-tissue infections. Lancet Infect Dis. 2023;23(3):e81-e94. doi:10.1016/S1473-3099(22)00583-7
Etiology of Necrotizing Soft-Tissue Infection
There are 2 subtypes of NSTI:
Type I (polymicrobial)
Type II (monomicrobial)
Type I NSTI typically involves the torso and perineum and results from a polymicrobial infection that usually includes group A streptococci (eg, Streptococcus pyogenes) and a mixture of aerobic and anaerobic bacteria (eg, Bacteroides species). These organisms typically extend to subcutaneous tissue from a contiguous ulcer or infection, or after trauma. Streptococci can translocate from a remote site of infection via the bloodstream. Perineal involvement (also called Fournier gangrene) is usually a complication of recent surgery, perirectal abscess, periurethral gland infection, or retroperitoneal infection resulting from perforated abdominal viscera. Patients with diabetes are at particular risk of type I NSTI. Type I NSTIs often produce gas in the soft tissue, manifesting similarly to that of gas gangrene (clostridial myonecrosis), which is a monomicrobial (type II) infection (1).


This photo shows life-threatening infection of the subcutaneous fat and muscles by streptococci (group A), causing widespread necrosis involving the lower back.
This photo shows life-threatening infection of the subcutaneous fat and muscles by streptococci (group A), causing wide
© Springer Science+Business Media


This photo shows a patient who has a necrotizing subcutaneous infection with discoloration and swelling of the scrotum.
This photo shows a patient who has a necrotizing subcutaneous infection with discoloration and swelling of the scrotum.
LIVING ART ENTERPRISES, LLC/SCIENCE PHOTO LIBRARY


This photo shows Fournier gangrene, which is necrotizing fasciitis of the perineum.
This photo shows Fournier gangrene, which is necrotizing fasciitis of the perineum.
Image courtesy of Noel Armenakas, MD.


The first photo on the left shows a preoperative image of the dorsal right arm with hemorrhagic bullae and cyanotic skin lesions.
The second photo from the left shows erupted vesicles on the medial arm.
The third and fourth photos show postoperative changes with extensive skin necrosis on the dorsal side and myonecrosis and cyanotic changes of underlying flexor muscles on the medial aspect.
The first photo on the left shows a preoperative image of the dorsal right arm with hemorrhagic bullae and cyanotic ski
© Springer Science+Business Media
This photo shows life-threatening infection of the subcutaneous fat and muscles by streptococci (group A), causing widespread necrosis involving the lower back.
This photo shows life-threatening infection of the subcutaneous fat and muscles by streptococci (group A), causing wide
© Springer Science+Business Media
This photo shows a patient who has a necrotizing subcutaneous infection with discoloration and swelling of the scrotum.
This photo shows a patient who has a necrotizing subcutaneous infection with discoloration and swelling of the scrotum.
LIVING ART ENTERPRISES, LLC/SCIENCE PHOTO LIBRARY
This photo shows Fournier gangrene, which is necrotizing fasciitis of the perineum.
This photo shows Fournier gangrene, which is necrotizing fasciitis of the perineum.
Image courtesy of Noel Armenakas, MD.
The first photo on the left shows a preoperative image of the dorsal right arm with hemorrhagic bullae and cyanotic skin lesions.
The second photo from the left shows erupted vesicles on the medial arm.
The third and fourth photos show postoperative changes with extensive skin necrosis on the dorsal side and myonecrosis and cyanotic changes of underlying flexor muscles on the medial aspect.
The first photo on the left shows a preoperative image of the dorsal right arm with hemorrhagic bullae and cyanotic ski
© Springer Science+Business Media
Type II NSTI is monomicrobial and is most commonly caused by group A beta-hemolytic streptococci; Staphylococcus aureus is the second most common pathogen (2). Patients tend to be younger with few documented health problems but may have a history of injection drug use, trauma, or recent surgery. The infection has the potential for rapid local spread and systemic complications such as toxic shock. A subgroup of type II NSTI usually occurs with aquatic injuries sustained in warmer coastal areas, particularly in patients with chronic liver disease (eg, cirrhosis), diabetes, and immunocompromise (3). Vibrio vulnificus is the usual pathogen.
Clostridial myonecrosis (gas gangrene) may develop spontaneously or after a deep, traumatic injury. Similar to type I NSTI, gas often develops in the tissue; however, as in type II NSTI, clostridial myonecrosis is typically a monomicrobial infection.


The skin over the infected area develops a bronze appearance. The skin is edematous, tense, and exquisitely tender with overlying bullae on the dorsum of the wrist and hand.
© Springer Science+Business Media
Etiology references
1. Stevens DL, Bryant AE. Necrotizing soft-tissue infections. N Engl J Med. 2017;377(23):2253–2265. doi:10.1056/NEJMra1600673
2. Centers for Disease Control and Prevention (CDC). Clinical Guidance for Type II Necrotizing Fasciitis. August 5, 2025. Accessed January 23, 2026.
3. CDC. Severe Vibrio vulnificus Infections in the United States Associated with Warming Coastal Waters. September 1, 2023. Accessed January 23, 2026.
Pathophysiology of Necrotizing Soft-Tissue Infection
NSTI causes tissue ischemia by widespread occlusion of small subcutaneous vessels. Bacterial virulence factors, particularly from group A streptococci, prevent neutrophil recruitment and killing while triggering coagulation activation that produces microthrombi and tissue infarction (1). Microthrombi and vessel occlusion result in skin infarction and necrosis, which facilitate the growth of obligate anaerobes (eg, Bacteroides) while promoting anaerobic metabolism by facultative organisms (eg, Escherichia coli), resulting in gangrene. Anaerobic metabolism (eg, secondary to clostridial infection) produces hydrogen and nitrogen, relatively insoluble gases that may accumulate in subcutaneous tissues.
Pathophysiology reference
1. Hua C, Urbina T, Bosc R, et al: Necrotising soft-tissue infections. Lancet Infect Dis. 2023;23(3):e81–e94. doi:10.1016/S1473-3099(22)00583-7
Symptoms and Signs of Necrotizing Soft-Tissue Infection
The primary symptom of NSTI is intense pain. However, in areas denervated by peripheral neuropathy (eg, patients with diabetes mellitus), pain may be minimal or absent.
Affected tissue is warm, erythematous, and/or violaceous and swollen and may rapidly become discolored. Bullae, crepitus (resulting from soft-tissue gas), and gangrene may develop. Subcutaneous tissues (including adjacent fascia) necrose, with widespread undermining of surrounding tissue. Muscles may be spared initially but can be involved as the infection progresses.
Patients are acutely ill, with high fever, tachycardia, altered mental status ranging from confusion to obtundation, and hypotension. Patients may become bacteremic or septic and may require aggressive hemodynamic support.
Streptococcal toxic shock syndrome may develop.
Diagnosis of Necrotizing Soft-Tissue Infection
History and physical examination
Imaging studies (eg, radiography, CT, MRI)
Blood and wound cultures
The diagnosis of NSTI is primarily clinical and is suggested by pain that appears out of proportion to clinical findings (1). Surgical exploration is considered the gold standard, during which gray exudate and friable superficial fascia can be encountered and absence of pus is noted (2). The diagnosis is supported by laboratory and other clinical findings including leukocytosis, elevated C-reactive protein, soft-tissue gas on radiography, positive blood cultures, and deteriorating metabolic and hemodynamic status.
CT and MRI can be used to identify the extent of disease, but treatment should not be delayed while awaiting imaging results.
Tools have been developed to help predict the risk of NSTIs, but they should not be used to rule out disease because of limited sensitivity. The Laboratory Risk Indicator for Necrotizing Fasciitis (LRINEC) score uses C-reactive protein, white blood cell count, hemoglobin, sodium, creatinine, and glucose values to differentiate NSTI from other soft-tissue infections. The LRINEC score has moderate specificity, but its use is limited by poor sensitivity (3). The NECROSIS score is another clinical risk index that uses systolic blood pressure measurement, violaceous skin discoloration, and white blood cell count to identify NSTI in high-risk settings (4, 5). This score is characterized by very high specificity but requires further external validation.
Differentiation from clostridial myonecrosis is made using microbiologic testing, but because treatment should occur immediately, it is aimed at both NSTI and clostridial myonecrosis.

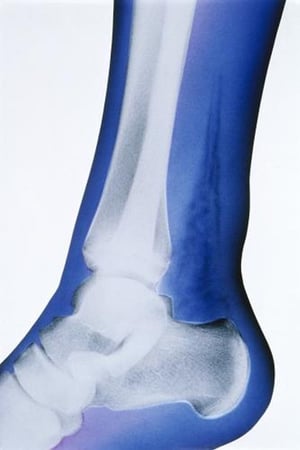
In this artificially colored radiograph, the salient finding is the presence of soft-tissue gas, indicated by the highly radiolucent densities (in black) superior to the calcaneus and posterior to the tibia and fibula.
In this artificially colored radiograph, the salient finding is the presence of soft-tissue gas, indicated by the highl
CHRIS BJORNBERG/SCIENCE PHOTO LIBRARY


This radiograph shows soft-tissue gas in the right hemiscrotum (arrows).
This radiograph shows soft-tissue gas in the right hemiscrotum (arrows).
© Springer Science+Business Media


This abdominal radiograph shows an extension of soft-tissue gas from the left hemiscrotum (*) to the left abdominal wall (arrows).
This abdominal radiograph shows an extension of soft-tissue gas from the left hemiscrotum (*) to the left abdominal wal
© Springer Science+Business Media
In this artificially colored radiograph, the salient finding is the presence of soft-tissue gas, indicated by the highly radiolucent densities (in black) superior to the calcaneus and posterior to the tibia and fibula.
In this artificially colored radiograph, the salient finding is the presence of soft-tissue gas, indicated by the highl
CHRIS BJORNBERG/SCIENCE PHOTO LIBRARY
This radiograph shows soft-tissue gas in the right hemiscrotum (arrows).
This radiograph shows soft-tissue gas in the right hemiscrotum (arrows).
© Springer Science+Business Media
This abdominal radiograph shows an extension of soft-tissue gas from the left hemiscrotum (*) to the left abdominal wall (arrows).
This abdominal radiograph shows an extension of soft-tissue gas from the left hemiscrotum (*) to the left abdominal wal
© Springer Science+Business Media
Diagnosis references
1. Stevens DL, Bryant AE. Necrotizing soft-tissue infections. N Engl J Med. 2017;377(23):2253–2265. doi:10.1056/NEJMra1600673
2. Hua C, Urbina T, Bosc R, et al: Necrotising soft-tissue infections. Lancet Infect Dis. 2023;23(3):e81–e94. doi:10.1016/S1473-3099(22)00583-7
3. Fernando SM, Tran A, Cheng W, et al. Necrotizing Soft Tissue Infection: Diagnostic Accuracy of Physical Examination, Imaging, and LRINEC Score: A Systematic Review and Meta-Analysis. Ann Surg. 2019;269(1):58-65. doi:10.1097/SLA.0000000000002774
4. Kim DY, Lavasile A, Kaji AH, et al. Prospective derivation and validation of a necrotizing soft tissue infections score: An EASTmulticenter trial. J Trauma Acute Care Surg. 2024;97(6):910-917. doi:10.1097/TA.0000000000004374
5. McDermott J, Kao LS, Keeley JA, Grigorian A, Neville A, de Virgilio C. Necrotizing Soft Tissue Infections: A Review. JAMA Surg. 2024;159(11):1308-1315. doi:10.1001/jamasurg.2024.3365
Treatment of Necrotizing Soft-Tissue Infection
Surgical debridement (including, rarely, amputation)
Antibiotics
Supportive care
Treatment of early NSTI including clostridial myonecrosis is primarily surgical (which should not be delayed by diagnostic studies) combined with empiric broad-spectrum antibiotics and intensive supportive care (1, 2).
Immediate surgical exploration and debridement are done when there is evidence of bullae, ecchymosis, fluctuance, crepitus, and systemic spread of infection. The initial incision should be extended until an instrument or finger can no longer separate the skin and subcutaneous tissue from the deep fascia. The most common error is insufficient surgical intervention; serial debridement every 1 to 2 days, with further incision and debridement as needed, should be carried out routinely. Negative-pressure wound therapy (NPWT), also called vacuum-assisted closure (VAC), applies suction to the wound and has been used as an adjunct for care between debridements.
Because serial debridements should be continued until no further necrosis is identified, amputation of an extremity may sometimes be necessary.
IV antibiotics are typically initiated immediately after diagnosis, usually including 2 or more medications. An empiric regimen should include antibiotics effective against aerobic and anaerobic organisms. The Infectious Diseases Society of America (IDSA) recommends vancomycin, linezolid, or daptomycin combined with piperacillin/tazobactam, a carbapenem, ceftriaxone plus metronidazole, or a fluoroquinolone plus metronidazole (3). Clindamycin and linezolid are also often administered to inhibit toxin production. Antibiotic coverage should be narrowed based on blood and tissue culture results once they become available.
Supportive care includes IV fluids, which may be needed in large volumes before and after surgery.
IV immune globulin (IVIG) has been suggested as adjunctive therapy for streptococcal toxic shock syndrome with NSTI, but robust clinical data are lacking.
Pearls & Pitfalls
|
Treatment references
1. Stevens DL, Bryant AE. Necrotizing soft-tissue infections. N Engl J Med. 2017;377(23):2253–2265. doi:10.1056/NEJMra1600673
2. Hua C, Urbina T, Bosc R, et al: Necrotising soft-tissue infections. Lancet Infect Dis. 2023;23(3):e81–e94. doi:10.1016/S1473-3099(22)00583-7
3. Stevens DL, Bisno AL, Chambers HF, et al. Practice guidelines for the diagnosis and management of skin and soft tissue infections: 2014 update by the Infectious Diseases Society of America. Clin Infect Dis. 2014;59(2):e10-e52. doi:10.1093/cid/ciu444
Prognosis for Necrotizing Soft-Tissue Infection
All-cause mortality rate in treated patients with NSTI is approximately 20 to 30% (1).
Old age, chronic medical disorders, delayed diagnosis and therapy, severe NSTI, and insufficient surgical debridement worsen prognosis.
Prognosis reference
1. Hua C, Urbina T, Bosc R, et al. Necrotising soft-tissue infections. Lancet Infect Dis. 2023;23(3):e81–e94. doi:10.1016/S1473-3099(22)00583-7
Key Points
Necrotizing soft-tissue infection (NSTI) can develop from a contiguous ulcer or infection, hematogenous spread, or after trauma.
Consider NSTI in patients with characteristic findings or pain out of proportion to clinical findings, particularly patients with diabetes or other risk factors.
Arrange surgical therapy while instituting IV fluid and antibiotic therapy and without delaying for testing.
Drug Information for the Topic





