

Submandibular space infection is acute cellulitis of the soft tissues below the mouth. Symptoms include pain, dysphagia, and potentially fatal airway obstruction. Diagnosis usually is clinical. Treatment includes airway management, surgical drainage, and IV antibiotics.
Submandibular space infection is a rapidly spreading, bilateral, indurated cellulitis occurring in the suprahyoid soft tissues, the floor of the mouth, and both sublingual and submaxillary spaces without abscess formation. Although not a true abscess, it resembles one clinically and is treated similarly.
The condition usually develops from an odontogenic infection, especially of the 2nd and 3rd mandibular molars. Contributing factors may include poor dental hygiene, tooth extractions, and trauma (eg, fractures of the mandible, lacerations of the floor of the mouth).
Symptoms and Signs of Submandibular Space Infection

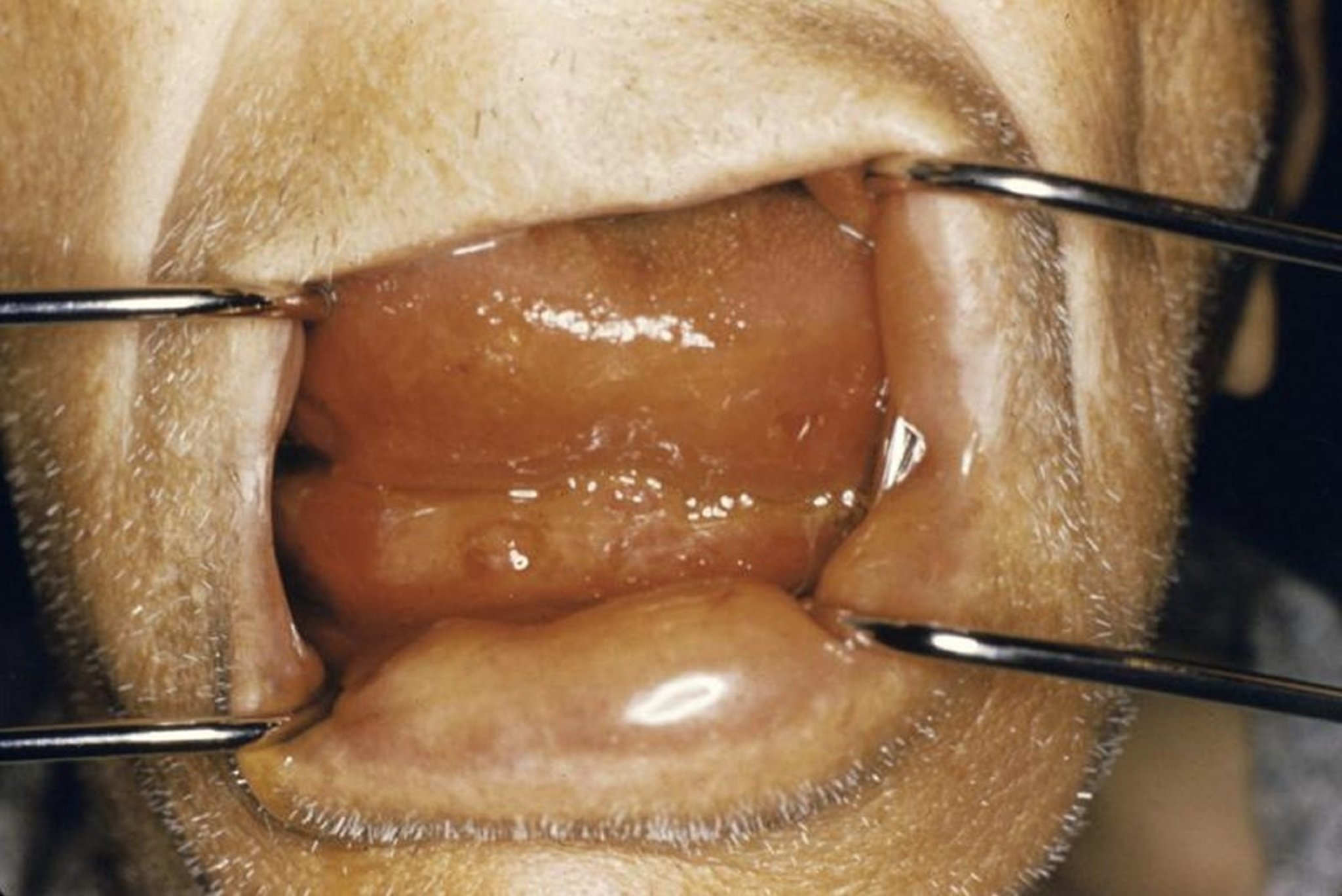
Ludwig angina can cause swelling below the tongue that can block the airway.
Photo provided by Clarence T. Sasaki, MD.
Early manifestations of submandibular space infection are pain in any involved teeth, with severe, tender, localized submental and sublingual induration. Boardlike firmness of the floor of the mouth and brawny induration of the suprahyoid soft tissues may develop rapidly. Drooling, trismus, dysphagia, stridor caused by laryngeal edema, and elevation of the posterior tongue against the palate may be present. Fever, chills, and tachycardia are usually present as well. The condition can cause airway obstruction within hours and does so more often than do other neck infections. The overall mortality rate is approximately 0.3% (1).
General reference
1. McDonnough JA, Ladzekpo DA, Yi I, et al: Epidemiology and resource utilization of ludwig angina ED visits in the United States 2006-2014. Laryngoscope 129 (9):2041–2044, 2019. doi: 10.1002/lary.27734
Diagnosis of Submandibular Space Infection
Clinical evaluation and sometimes CT
Submandibular space infection usually is obvious during clinical evaluation. If not, CT is done to confirm the diagnosis.
Treatment of Submandibular Space Infection
Maintenance of airway patency
Surgical incision and drainage
Antibiotics active against oral flora
Maintaining airway patency is of the highest priority. Because swelling makes oral endotracheal intubation difficult, fiberoptic nasotracheal intubation done with topical anesthesia in the operating room or intensive care unit with the patient awake is preferable. Some patients require a tracheotomy. Patients without immediate need for intubation require intense observation and may benefit temporarily from a nasal trumpet.
Incision and drainage with placement of drains deep into the mylohyoid muscles relieve the pressure. Antibiotics should be chosen to cover both oral anaerobes and aerobes (eg, clindamycin, ampicillin/sulbactam, and/or high-dose penicillin).Incision and drainage with placement of drains deep into the mylohyoid muscles relieve the pressure. Antibiotics should be chosen to cover both oral anaerobes and aerobes (eg, clindamycin, ampicillin/sulbactam, and/or high-dose penicillin).
Drug Information for the Topic





