



Peripheral ulcerative keratitis is inflammation and ulceration of the cornea that often occurs with chronic systemic rheumatic diseases. Irritation and decreased vision result.
Peripheral ulcerative keratitis is a serious corneal ulceration; it often occurs with systemic rheumatic diseases that are active, long-standing, or both, such as rheumatoid arthritis (RA), granulomatosis with polyangiitis (formerly called Wegener granulomatosis), and relapsing polychondritis.
Patients often have decreased visual acuity, photophobia, and foreign body sensation. A crescentic area of opacification develops in the periphery of the cornea due to infiltration by white blood cells (WBCs). Ulceration, which stains with fluorescein, develops shortly after opacification. This is the opposite to the usual infectious ulcer that begins with an epithelial defect and later develops opacification. Infectious causes, such as bacteria, fungi, and herpes simplex virus, must be ruled out by culturing the ulcer and eyelid margins.

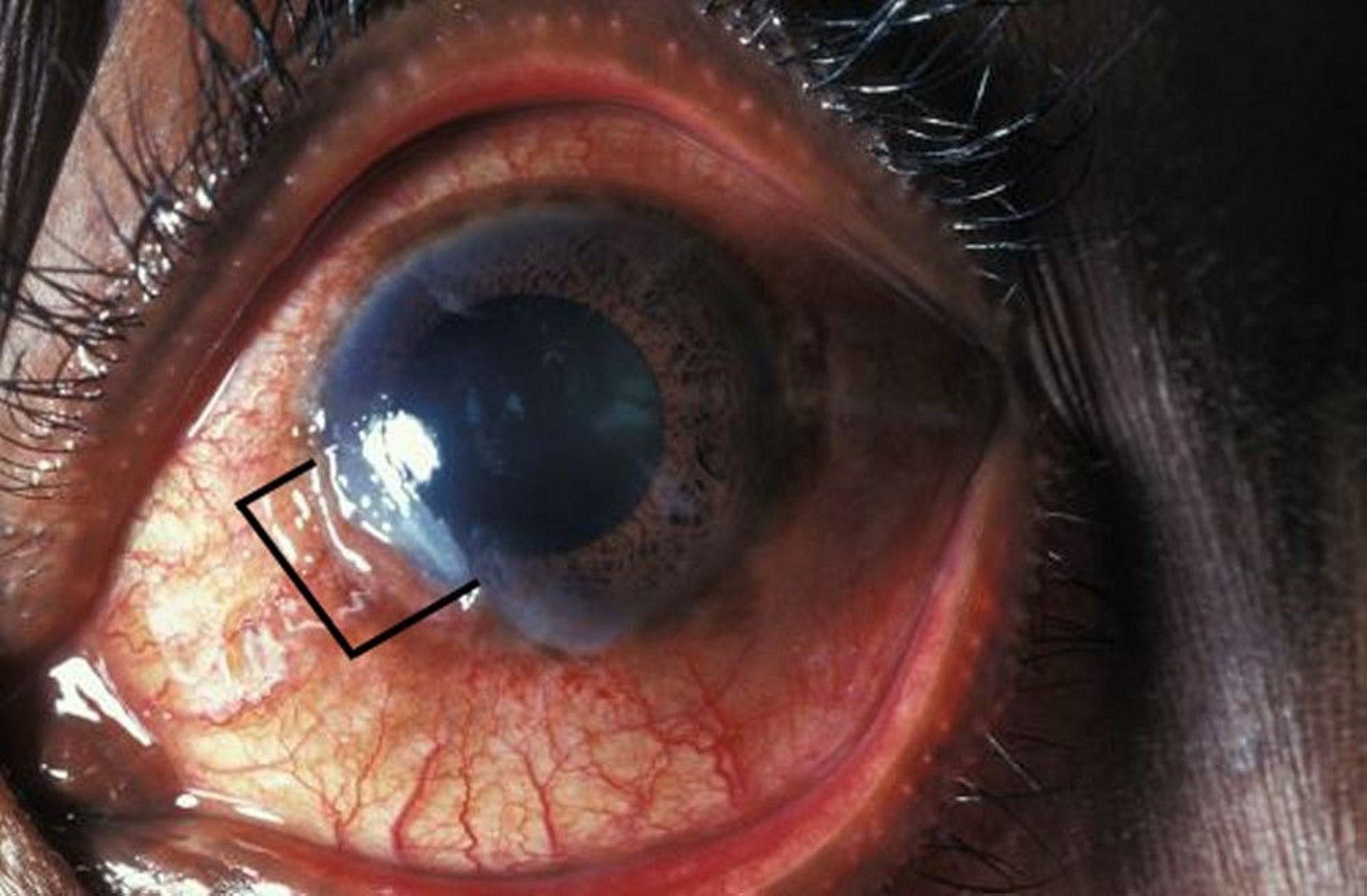
Peripheral ulcerative keratitis starts as opacification (gray area from 6:30 to 9 o'clock) with white cell infiltrate in the corneal periphery, followed by ulceration.
DR M.A. ANSARY/SCIENCE PHOTO LIBRARY
Among patients with systemic rheumatic disease and peripheral ulcerative keratitis, the 10-year mortality rate had been approximately 40 to 50% (usually due to myocardial infarction) without treatment and approximately 8% with systemic cytotoxic therapy (1); however, the prognosis is better now with immunosuppressive therapy.
Any patient with peripheral ulcerative keratitis should be promptly referred to an ophthalmologist. Systemic cyclophosphamide, other immunosuppressants, or biologics such as rituximab and etanercept treat the keratitis, life-threatening vasculitis, and underlying systemic rheumatic disease. Treatment also includes local approaches to control inflammation (eg, tissue adhesive and bandage contact lenses) and repair damage (eg, patch grafts). Other possibly helpful medications include collagenase inhibitors, such as systemic tetracycline or topical 20% N-acetylcysteine (2).
References
1. Foster CS, Forstot SL, Wilson LA. Mortality rate in rheumatoid arthritis patients developing necrotizing scleritis or peripheral ulcerative keratitis. Effects of systemic immunosuppression. Ophthalmology. 1984;91(10):1253-1263. doi: 10.1016/s0161-6420(84)34160-4
2. Hassanpour K, H ElSheikh R, Arabi A, et al. Peripheral ulcerative keratitis: A review. J Ophthalmic Vis Res. 2022;17(2):252-275. doi: 10.18502/jovr.v17i2.10797.
Drug Information for the Topic





