



Papilledema is swelling of the optic disc due to increased intracranial pressure. Optic disc swelling resulting from causes that do not involve increased intracranial pressure (eg, malignant hypertension, central retinal vein occlusion) is not considered papilledema. There are often no early visual symptoms, although vision may darken for a few seconds intermittently (transient visual obscurations). Papilledema requires a search for the cause. Diagnosis is by ophthalmoscopy with further tests, usually brain imaging and often subsequent lumbar puncture, to determine cause. Treatment is directed at the underlying condition.
Papilledema is a sign of elevated intracranial pressure and is almost always bilateral. Causes include the following:
Idiopathic intracranial hypertension (pseudotumor cerebri, the most common cause [1]), a condition with elevated cerebrospinal fluid (CSF) pressure and no mass lesion
Arachnoidal adhesions
Cavernous or dural sinus thrombosis
Obstructive hydrocephalus
General reference
1. Crum OM, Kilgore KP, Sharma R, et al. Etiology of papilledema in patients in the eye clinic setting. JAMA Netw Open. 2020;3(6):e206625. doi:10.1001/jamanetworkopen.2020.6625
Symptoms and Signs of Papilledema
In patients with papilledema, vision is usually not affected initially, but seconds-long graying out of vision, flickering, or blurred or double vision may occur. Patients may have symptoms of increased intracranial pressure, such as headache, pulsatile tinnitus, or nausea and vomiting.
Ophthalmoscopic examination reveals engorged and tortuous retinal veins, a hyperemic and swollen optic disc (optic nerve head), and retinal hemorrhages around the disc but not into the retinal periphery. Disc edema (eg, caused by optic neuritis or ischemic optic neuropathy) without increased intracranial pressure is not considered papilledema.

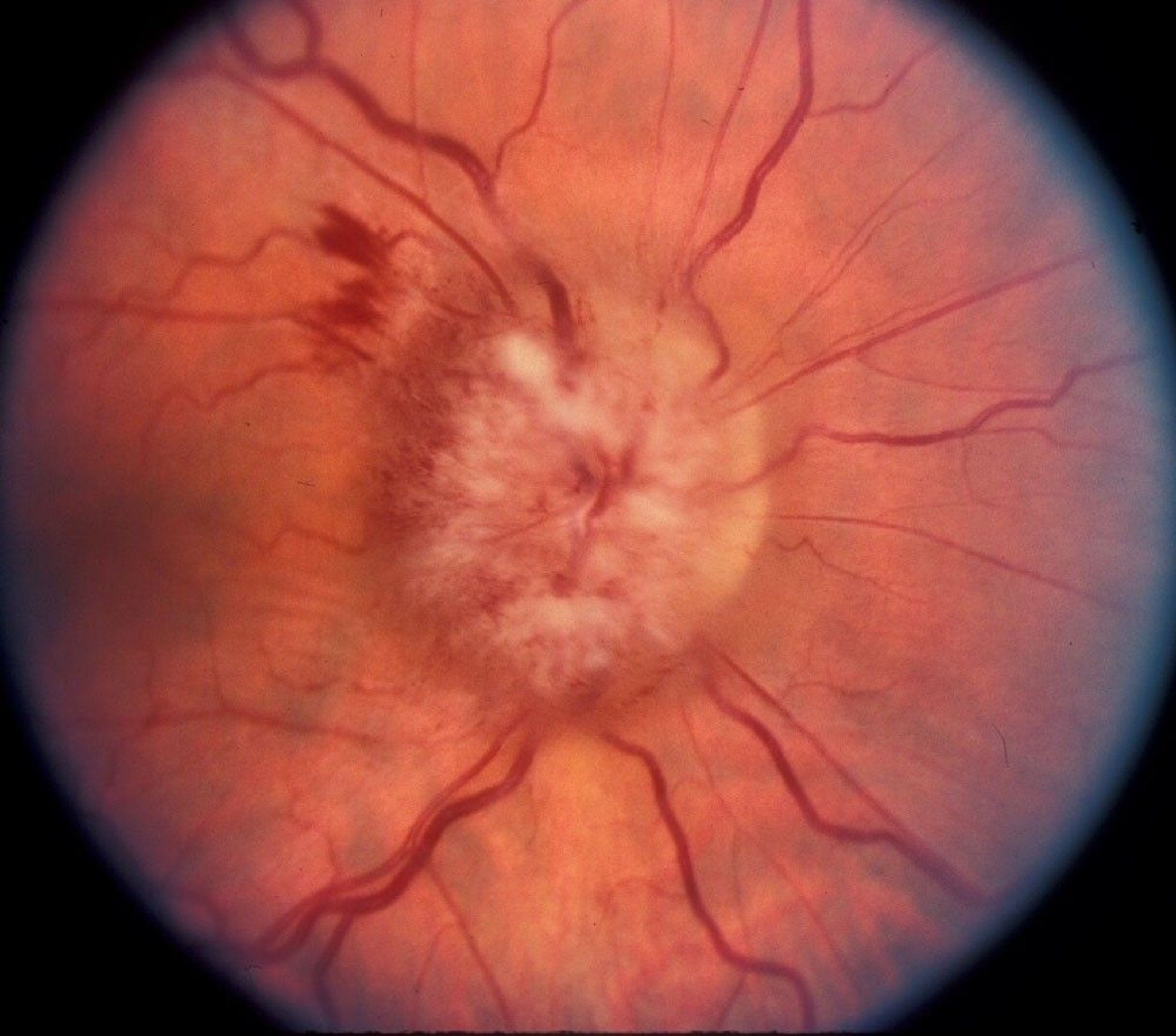
Funduscopic findings of papilledema include engorged and tortuous retinal veins, a hyperemic and swollen optic disc, and retinal hemorrhages around the disc. A swollen optic disc is suggested by disc elevation, loss of the optic cup, and obscuration of the fine vessels on the optic nerve surface.
Image provided by James Garrity, MD.
In the early stages of papilledema, visual acuity and pupillary response to light are usually normal and become abnormal only after the condition is well advanced. Visual field testing may detect an enlarged blind spot. Later, visual field testing may show peripheral vision loss with arcuate defects that follow the nerve fiber bundle defects.
Diagnosis of Papilledema
Clinical evaluation
Immediate neuroimaging
The degree of disc swelling can be quantified by comparing the plus lens numbers needed to focus an ophthalmoscope on the most elevated portion of the disc and on the unaffected portion of the retina. Swelling can also be quantified by measuring nerve fiber layer thickness using optical coherence tomography (OCT); OCT is performed to quantify the degree of papilledema so that changes can be monitored.
Differentiating papilledema due to elevated intracranial pressure from other causes of a swollen optic disc, such as optic neuritis, ischemic optic neuropathy, hypotony (intraocular pressure ≤ 5 mm Hg), central retinal vein occlusion, uveitis, or pseudo swollen discs (eg, optic nerve drusen), requires a thorough ophthalmologic evaluation.
B-scan ultrasound, OCT, and fundus autofluorescence are the best diagnostic tools for the pseudo disc edema of optic nerve drusen. If papilledema is suspected clinically, MRI of the brain with gadolinium contrast or CT with contrast is performed immediately to exclude causes such as an intracranial mass. MR venogram or CT venogram is often performed to exclude a dural venous sinus thrombosis.
Lumbar puncture with measurement of CSF pressure and analysis of CSF should be performed following neuroimaging if a mass lesion has been ruled out. Lumbar puncture in patients with intracranial mass lesions can result in brain stem herniation. If no mass is seen on MRI, the opening pressure is elevated and other causes of raised intracranial pressure have been ruled out, the diagnosis is idiopathic intracranial hypertension (IIH), which is the most common cause of raised intracranial pressure.
Treatment of Papilledema
Treatment of underlying disorder
Urgent treatment of the underlying disorder is indicated to decrease intracranial pressure. For idiopathic intracranial hypertension, weight loss and medications, such as acetazolamide or topiramate, are first-line therapies (1). Surgery, usually reserved for severe vision-threatening papilledema that is not responsive to medications, includes ventriculo-peritoneal shunt, optic nerve sheath fenestration, and cerebral venous sinus stenting. If intracranial pressure is not reduced, secondary optic nerve atrophy and vision loss can occur.
Treatment reference
1. Raoof N, Hoffmann J. Diagnosis and treatment of idiopathic intracranial hypertension. Cephalalgia. 2021;41(4):472-478. doi:10.1177/0333102421997093
Key Points
Papilledema is disc edema due to increased intracranial pressure.
In addition to bilateral hyperemic and swollen optic discs (optic nerve heads), patients typically have engorged and tortuous retinal veins, and retinal hemorrhages around the disc but not into the retinal periphery.
Fundoscopic abnormalities usually precede visual disturbances.
Perform immediate neuroimaging and, if no mass lesion is seen, obtain CSF for analysis and measure CSF pressure with a lumbar puncture.
Treat the underlying disorder.
Drug Information for the Topic





