



Onchocerciasis is a filarial nematode (worm) infection with Onchocerca volvulus. Blackflies are responsible for transmission. Symptoms are subcutaneous nodules, pruritus, dermatitis, adenopathy, atrophy and scarring of skin, and eye lesions that may lead to blindness. Diagnosis is by finding microfilariae in skin samples, the cornea, or the anterior chamber of the eye; identifying adult worms in subcutaneous nodules; or using polymerase chain reaction (PCR) to detect parasite DNA. Treatment is with ivermectin.
An estimated 21 million people are infected with onchocerciasis worldwide; approximately 14.6 million have skin disease and 1.15 million have visual impairment or loss (1). Onchocerciasis is the second leading cause of infectious blindness worldwide (after trachoma).
Onchocerciasis is most common in tropical and sub-Saharan regions of Africa. Small foci exist in Yemen and along the Venezuelan border with the Brazilian Amazon. Blindness due to onchocerciasis is fairly rare in the Americas; Colombia, Ecuador, Mexico, and Guatemala have been declared free of onchocerciasis by the World Health Organization (WHO).
People who live or work near rapidly flowing streams or rivers are the most likely to be infected. In addition to residents, long-term travelers (eg, missionaries, aid workers, field researchers) are at risk.
(See also Approach to Parasitic Infections and Overview of Filarial Nematode Infections.)
General reference
1. GBD 2017 Disease and Injury Incidence and Prevalence Collaborators. Global, regional, and national incidence, prevalence, and years lived with disability for 354 diseases and injuries for 195 countries and territories, 1990-2017: a systematic analysis for the Global Burden of Disease Study 2017 [published correction appears in Lancet. 2019 Jun 22;393(10190):e44. doi: 10.1016/S0140-6736(19)31047-5]. Lancet. 2018;392(10159):1789-1858. doi:10.1016/S0140-6736(18)32279-7
Pathophysiology of Onchocerciasis
Onchocerciasis is spread by female blackflies (Simulium genus) that breed in swiftly flowing streams (hence, the term "river blindness"). Many blackfly bites are needed before disease develops.
Infective larvae inoculated into the skin during the bite of a blackfly develop into adult worms in 12 to 18 months. Adult female worms may live up to 15 years in subcutaneous nodules. Females are 33 to 50 cm long; males are 19 to 42 mm long. Mature female worms produce microfilariae that migrate mainly through the skin and invade the eyes.


1. During a blood meal, an infected blackfly transmits filarial larvae onto the skin of the human host, where the larvae enter the bite wound.
2. The larvae migrate to subcutaneous tissues.
3. There, the larvae develop into adult filariae, which commonly reside in subcutaneous nodules for up to 15 years.
4. After mating, female worms produce unsheathed microfilariae, which are typically present in the skin and the lymphatics of connective tissues but are occasionally present in peripheral blood, urine, and sputum.
5. A blackfly ingests the microfilariae during a blood meal.
6. After ingestion, the microfilariae penetrate the blackfly's midgut and migrate to the thoracic muscles.
7–8. There, the microfilariae develop into first-stage (L1) larvae and subsequently into third-stage (L3) infective larvae.
9. Larvae migrate to the blackfly's proboscis and can infect another human when the fly takes a blood meal.
Image from the Centers of Disease Control and Prevention, Global Health, Division of Parasitic Diseases and Malaria.
Symptoms and Signs of Onchocerciasis
Onchocerciasis typically affects
Skin (nodules, dermatitis)
Eyes
Nodules
The subcutaneous (or deeper) nodules (onchocercoma) that contain adult worms may be visible or palpable but are otherwise asymptomatic. They are composed of inflammatory cells and fibrotic tissue in various proportions. Old nodules may caseate or calcify.
Patients may have enlargement of inguinal, femoral, or other lymph nodes. Localized swelling of the genitalia and inguinal hernias can develop.
Skin disease
Onchocercal dermatitis is caused by the microfilarial stage of the parasite. Intense pruritus may be the only symptom in lightly infected people.
Skin lesions usually consist of a nondescript maculopapular rash with secondary excoriations, scaling ulcerations and lichenification, and mild to moderate lymphadenopathy. Other skin abnormalities can include premature wrinkling, atrophy, patchy hypopigmentation, and loss of elasticity. In severe cases, patients may develop folds of atrophic skin in the lower abdomen and upper medial thighs ("hanging groin").
Onchocercal dermatitis is generalized in most patients, but a localized and sharply delineated form of eczematous dermatitis with hyperkeratosis, scaling, and pigment changes (Sowdah) is common in Yemen and Sudan.
Eye disease
Ocular involvement ranges from mild visual impairment to complete blindness. Lesions of the anterior portion of the eye include
Punctate (snowflake) keratitis (an acute inflammatory infiltrate surrounding dying microfilariae that resolves without causing permanent damage)
Sclerosing keratitis (an ingrowth of fibrovascular scar tissue that may cause subluxation of the lens and blindness)
Anterior uveitis or iridocyclitis (which may deform the pupil)
Chorioretinitis, optic neuritis, and optic atrophy may also occur.

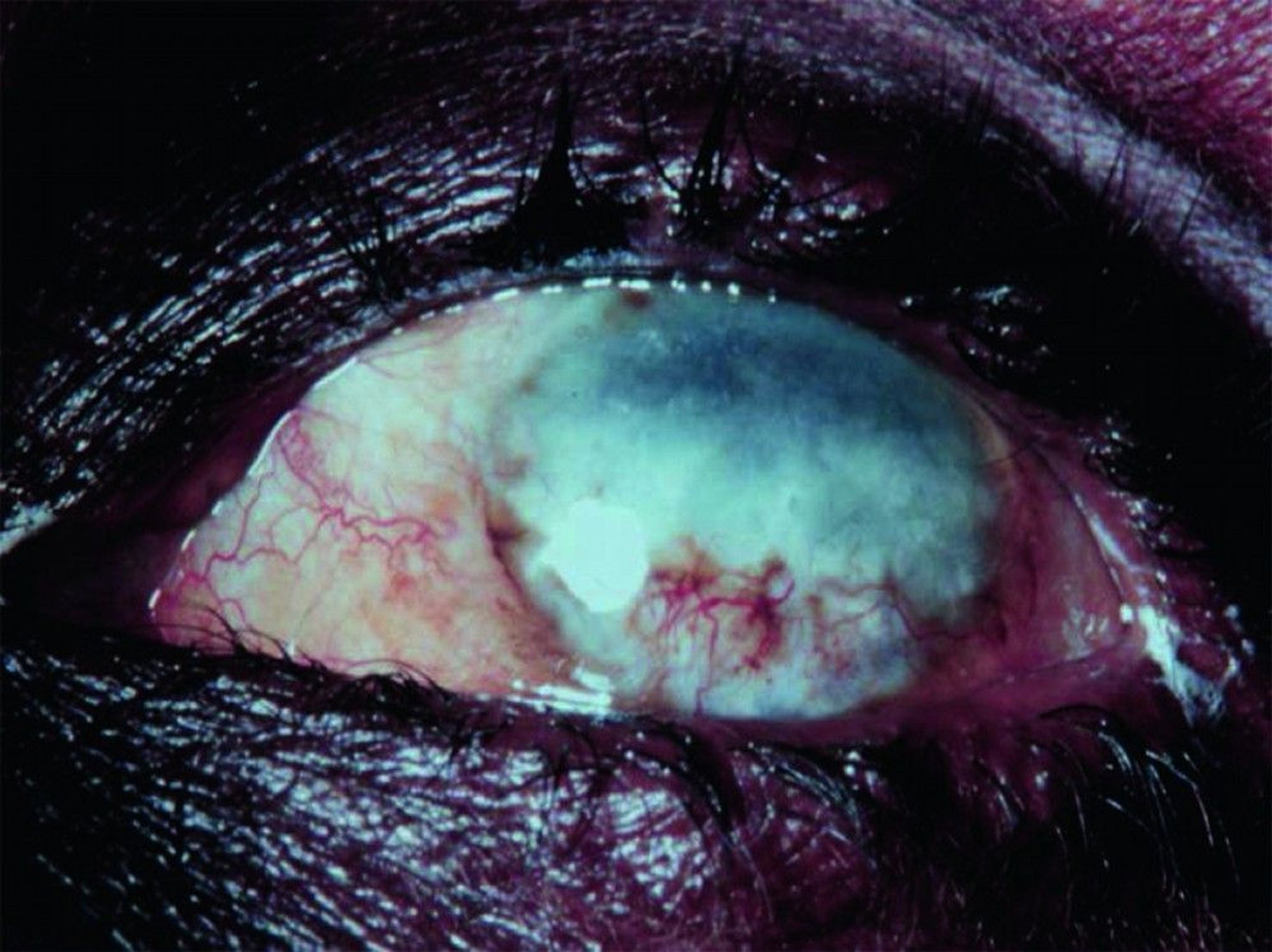
© Springer Science+Business Media
Diagnosis of Onchocerciasis
Microscopic examination of skin snips or biopsies
Slit-lamp examination of the cornea and anterior chamber of the eye
Demonstration of microfilariae in skin snips or biopsies is the traditional diagnostic method for onchocerciasis; multiple samples are usually taken (see table ). PCR-based methods to detect parasite DNA in skin samples are more sensitive than standard techniques but are available only in research settings.
Microfilariae may also be visible in the cornea and anterior chamber of the eye during slit-lamp examination.
Antibody detection is of limited value; there is substantial antigenic cross-reactivity among O. volvulus and other filaria and different helminths, and a positive serologic test does not distinguish between past and current infection.
Palpable nodules (or deep nodules detected by ultrasound or MRI) can be excised and examined for adult worms, but this procedure is rarely necessary.
Treatment of Onchocerciasis
Ivermectin
Ivermectin, the primary therapeutic option, reduces microfilariae in the skin and eyes and decreases production of microfilariae for many months. It does not kill adult female worms, but cumulative doses decrease their fertility. Ivermectin is given as a single oral dose of 150 mcg/kg, repeated at 6- to 12-month intervals. The optimal duration of therapy is uncertain. Although treatment could theoretically be continued for the life span of female worms (10 to 14 years), it is usually stopped after several years if pruritis has resolved and no evidence of microfilariae is detected by skin biopsy or eye examination.
Adverse effects of ivermectin are qualitatively similar to those of diethylcarbamazine (DEC) but are much less common and less severe. DEC is not used for onchocerciasis because it can cause a severe hypersensitivity (Mazzotti) reaction to released filarial antigens, which can further damage skin and eyes and lead to cardiovascular collapse. Mild Mazzotti reactions are a frequent complication during treatment, and severe reactions can be managed with low-dose corticosteroids rapidly tapered (1).
Before treatment with ivermectin, patients should be assessed for coinfection with Loa loa, another filarial parasite, if they have been in areas of central Africa where both parasites are transmitted because ivermectin can cause severe reactions in patients with heavy Loa loa coinfection.
Pearls & Pitfalls
|
A randomized trial found a single oral dose of moxidectin 8 mg was superior in reducing microfilariae relative to a single dose of ivermectin (2).
Doxycycline can kill the endosymbiont bacteria Wolbachia, which O. volvulus requires for survival and embryogenesis. This antibiotic kills > 60% of adult female worms and sterilizes or decreases the fertility of those that survive, but it does not kill microfilariae. Doxycycline 100 mg orally once or twice a day for 6 weeks can be started 1 week after the initial single dose of ivermectin (150 mcg/kg). In a randomized clinical trial, doxycycline, given with or without ivermectin, was associated with increased clearance of microfilariae (3), but, in a systematic review, clear improvement in clinical and vision-related outcomes were not identified (4).
Doxycycline is a potential alternative for treatment of onchocerciasis in patients in Loa loa-endemic areas, but it has not been evaluated in patients with heavy Loa loa infection (> 8000 microfilariae/mL blood) (3).
Surgical removal of accessible onchocercomas can reduce skin microfilaria counts, but it has been replaced by ivermectin therapy.
Treatment references
1. Stingl P, Pierce PF, Connor DH, et al. Does dexamethasone suppress the Mazzotti reaction in patients with onchocerciasis?. Acta Trop. 1988;45(1):77-85.
2. Opoku NO, Bakajika DK, Kanza EM, et al. Single dose moxidectin versus ivermectin for Onchocerca volvulus infection in Ghana, Liberia, and the Democratic Republic of the Congo: a randomised, controlled, double-blind phase 3 trial [published correction appears in Lancet. 2018 Oct 6;392(10154):1196. doi:10.1016/S0140-6736(18)32403-6]. Lancet. 2018;392(10154):1207-1216. doi:10.1016/S0140-6736(17)32844-1
3. Turner JD, Tendongfor N, Esum M, et al. Macrofilaricidal activity after doxycycline only treatment of Onchocerca volvulus in an area of Loa loa co-endemicity: a randomized controlled trial. PLoS Negl Trop Dis. 2010;4(4):e660. Published 2010 Apr 13. doi:10.1371/journal.pntd.0000660
4. Abegunde AT, Ahuja RM, Okafor NJ. Doxycycline plus ivermectin versus ivermectin alone for treatment of patients with onchocerciasis. Cochrane Database Syst Rev. 2016;2016(1):CD011146. Published 2016 Jan 15. doi:10.1002/14651858.CD011146.pub2
Prevention of Onchocerciasis
No medication has been shown to protect against infection with O. volvulus. However, annual or semiannual administration of ivermectin to the population in endemic areas effectively controls subclinical and undiagnosed disease and may thus decrease transmission.
Onchocerciasis was virtually eradicated in participating West African countries (except Sierra Leone) by aerial insecticide spraying of Simulium breeding sites and by ivermectin therapy of patients in the World Health Organization (WHO)–sponsored Onchocerciasis Control Programme that concluded in 2002. Large-scale treatment with ivermectin has resulted in the elimination of onchocerciasis from some endemic areas and is continuing in areas where disease persists (1).
Simulium bites can be minimized by avoiding fly-infested areas, by wearing protective clothing, and possibly by liberally applying insect repellents.
Prevention reference
1. World Health Organization (WHO): Onchocerciasis. Accessed October 22, 2024.
Key Points
Onchocerciasis is a filarial infection that causes skin lesions, rash, and, more importantly, eye disease, leading to visual impairment and sometimes blindness.
Diagnose by slit-lamp examination of the eye and microscopic examination of a skin snip; where available, polymerase chain reaction (PCR) testing may be helpful.
Treat with ivermectin to kill microfilaria and reduce the fertility of female worms; ivermectin does not kill adult worms.
Before treatment with ivermectin, patients should be assessed for coinfection with Loa loa if they have been in areas of central Africa where both parasites are transmitted.
Drug Information for the Topic





