



Fasciolopsiasis is infection with the intestinal fluke Fasciolopsis buski, which is acquired by eating aquatic plants or ingesting contaminated water.
Flukes are parasitic flatworms that infect various parts of the body (blood vessels, gastrointestinal tract, lungs, liver) depending on the species.
F. buski is present in the intestine of pigs in many parts of Asia and the Indian subcontinent. The prevalence of infection is highest among children in endemic areas. F. buski is also called the giant intestinal fluke because it is largest fluke that infects humans.
Human infection is typically acquired by ingesting contaminated water or eating aquatic (freshwater) plants, particularly bamboo shoots, watercress, or water chestnuts, that bear infectious metacercariae. F. buski requires a snail intermediate host for completion of its life cycle. The snails used by F. buski are small planorbid snails in the genera Hippeutis and Segmentina (1, 2). Adult worms attach to and ulcerate the mucosa of the proximal small bowel. They grow to about 20 to 75 mm by 8 to 20 mm. Adult worms have a life span of about 1 year.

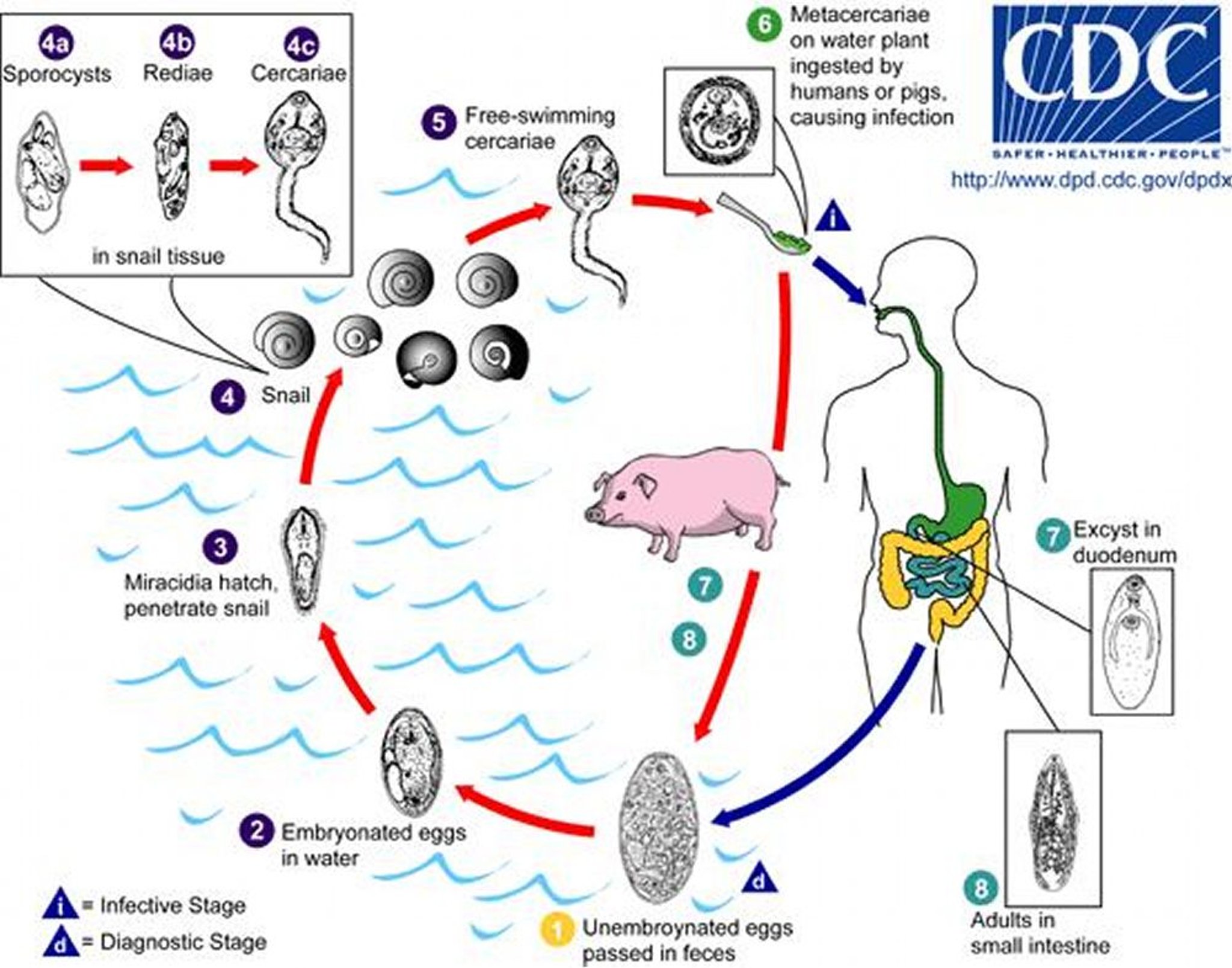
1. In the human host, unembryonated eggs are discharged into the intestine and pass out of the body with the feces.
2. Eggs become embryonated in water.
3. The eggs release miracidia, which penetrate a snail (intermediate host).
4. In the snail, the miracidia develop into sporocysts, then rediae, and then cercariae.
5. The cercariae are released from the snail.
6. They encyst (form cystic structures) as metacercariae on aquatic plants and may be ingested by a mammalian host (human or pig).
7. After ingestion, the metacercariae excyst (rupture out of existing cysts) in the duodenum and attach to the intestinal wall.
8. There, they develop into adult flukes in about 3 months.
Image from the Centers for Disease Control and Prevention Image Library.
Fasciolopsiasis is generally asymptomatic. In heavy infections, symptoms typically begin 30 to 60 days after exposure and can include anorexia, vomiting, diarrhea, abdominal pain, and signs of malabsorption. Peripheral eosinophilia may be present.
In severe cases, malabsorption can result in edema and ascites due to protein loss. Vitamin B12 deficiency and anemia can also occur.
Diagnosis of fasciolopsiasis is based on detecting eggs or, less commonly, adult worms in the feces or other gastrointestinal fluids (vomitus, bile, or gastroduodenal samples obtained via biopsy). F. buski eggs are broadly ellipsoidal, operculated and measure 130 to 150 micrometers long by 60 to 90 micrometers wide. The eggs are difficult to distinguish microscopically from those of Fasciola hepatica.


F. buski eggs are broadly ellipsoidal and operculated (protective covering or lid-like structure) and measure 130 to 150 micrometers long by 60 to 90 micrometers wide. F. buski eggs can be difficult to distinguish from Fasciola hepatica eggs, but the abopercular (opposite to the opercular end) ends of F. hepatica eggs often have a roughened or irregular area.
The eggs are unembryonated when passed in feces.
CDC/DPDx
Treatment of fasciolopsiasis is with praziquantel orally 3 times a day for 1 day.
Prevention involves not drinking contaminated water or eating freshwater plants in areas where Fasciolopsis buski is endemic (2).
References
1. Centers for Disease Control and Prevention: DPDx–Laboratory Identification of Parasites of Public Health Concern: Fasciolopsiasis. June 5, 2024. Accessed July 2, 2025.
2. Centers for Disease Control and Prevention: Fasciolopsiasis: About Fasciolopsiasis. April 25, 2024. Accessed July 11, 2025.
Drug Information for the Topic





