



Eschar is stiff, necrotic tissue caused by deep partial-thickness and full-thickness (formerly called 2nd- and 3rd-degree) burns. Circumferential eschar on a limb constricts distal circulation, and eschar on the thorax constricts respiration. Escharotomy is surgical incision through the eschar to release the constriction, thereby restoring distal circulation and allowing for adequate ventilation.
Escharotomy is usually done within the 2 to 6 hours after a burn injury (1, 2). Unlike fasciotomies, where incisions are made specifically to decompress tissue compartments, escharotomy incisions do not breach the deep fascial layer.
(See also Burns.)
Indications for Burn Escharotomy
Eschar compressing or potentially compressing tissue in or surrounding burn area
Compressed tissue is identified by any of the following:
Absent distal arterial flow as determined with a Doppler ultrasonic flow meter in the absence of systemic hypotension
An oxygen saturation below 95% in the distal end of the extremity as shown by pulse oximetry in the absence of systemic hypoxia
Measurement of compartment pressure > 30 mm Hg (see How to Measure Compartment Pressure in a Forearm and How to Measure Compartment Pressure in the Lower Leg)
Impending or established respiratory compromise due to circumferential torso or neck burns
Physicians should have a high index of suspicion and a low threshold for performing escharotomy.
Contraindications to Burn Escharotomy
None
Complications of Burn Escharotomy
Complications from the procedure include:
Bleeding
Infection
Damage to underlying neurovascular structures
Inadvertent fasciotomy
Equipment for Burn Escharotomy
Sterile drapes
Cleansing solution (eg, povidone-iodine or chlorhexidine)
25- and 21-gauge needles
10-mL syringes
Local anesthetic (eg, 1% lidocaine)
#11 scalpel and/or electrocautery device
Sterile gauze
Topical antimicrobial (eg, bacitracin or mupirocin)
Sterile gloves
Relevant Anatomy for Burn Escharotomy
Eschars occur in full-thickness burns or, less commonly, deep partial-thickness burns through at least the dermis.
A properly executed escharotomy releases the eschar to the depth of subcutaneous fat only. This release results in minimal bleeding, which can be controlled with local pressure or electrocautery.
Major neurovascular structures to avoid when incising at the following sites include:
Elbow: Ulnar nerve
Wrist: Radial nerve
Fibular head: Superficial peroneal nerve
Ankle: Posterior tibial artery
Neck: Jugular veins
Penis: Dorsal vein
Positioning for Burn Escharotomy
Position to provide excellent exposure of burn wound.
Step-by-Step Description of Burn Escharotomy
Cleanse the site with povidone-iodine or chlorhexidine solution.
Drape with sterile drapes.
If burns are particularly painful, give systemic opioid analgesia (eg, fentanyl 1 to 2 mcg/kg IV or morphine 0.1 to 0.2 mg/kg IV, then titrate as needed) (3, 4).
Unsedated patients should be given procedural sedation and/or local anesthesia injected into viable tissue at the proximal and distal edges of the wound.
Limbs
Using sterile technique, incise the lateral and medial aspects of the involved extremity with a scalpel or electrocautery device from 1 cm proximal to the burned area to 1 cm distal to the involved area of constricting burn.
Avoid vital structures such as major arteries and nerves (eg, ulnar nerve at the elbow, the radial nerve at the wrist, the superficial peroneal nerve near the fibular head, the posterior tibial artery at the ankle).
Carry the incision only through the full thickness of skin. Incisions should cross joints. This incision should result in immediate separation of the constricting eschar to expose subcutaneous fat.
In circumferential burns of the hands, extend the incisions to the thenar and hypothenar aspects of the hand.
In circumferential burns of the feet, extend the incision to the great toe medially and the little toe laterally.
Reassess perfusion: A properly done escharotomy results in near-immediate softening of the tissue, improved distal tissue perfusion, sensation, Doppler flow signal strength, and oximetry values. If perfusion fails to improve after the procedure, reassess the escharotomy depth and location and reincise any insufficiently deep incisions.
Chest
Using sterile technique, incise the chest wall from the clavicle to the costal margin in the anterior axillary line bilaterally; avoid breast tissue in females (see figure ). Consider joining this by transverse subcostal incisions to result in a chevron-shaped subcostal incision.
Assess response: Increased airway pressure or an inability to ventilate is evidence of the need to reincise the eschar.
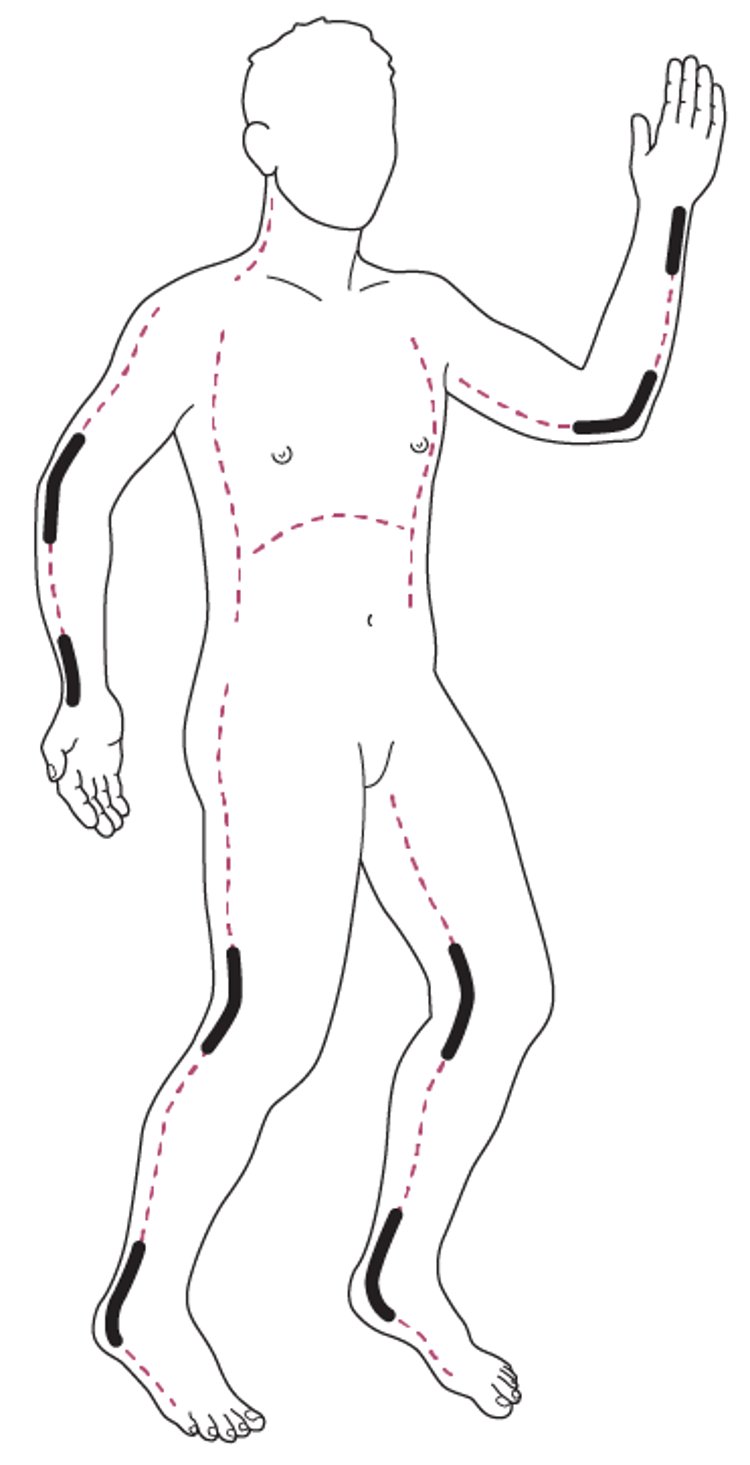
Escharotomy Incision Sites
The dashed lines are the preferred escharotomy incision sites. The bold lines are areas where vascular structures and nerves may be damaged by escharotomy incisions. |

Neck
Neck escharotomy should be done laterally and posteriorly to avoid the carotid and jugular vessels.
Penis
Penile escharotomy is done mid-laterally to avoid the dorsal vein.
Aftercare for Burn Escharotomy
Loosely pack incisions with sterile gauze impregnated with an appropriate topical antimicrobial such as bacitracin, silver sulfadiazine or mupirocin.
Transfer to a local or regional burn center for coordinated and definitive care, including pain control and tissue perfusion monitoring.
If a burn center is unavailable, admit to a local hospital.
Warnings and Common Errors for Burn Escharotomy
Because of edema and shock, skin temperature is a poor indicator of limb ischemia. Use objective measures (eg, absent distal Doppler flow, oxygen saturation below 95% in the distal end of the extremity as shown by pulse oximetry in the absence of systemic hypoxia, elevated compartment pressure) whenever possible.
Escharotomy incisions are at risk of infection. Treat incisions as part of the burn wound.
Do not confuse escharotomy with fasciotomy; escharotomy incisions remain above the fascial layer.
Tips and Tricks for Burn Escharotomy
Full-thickness burns are insensitive to pain and involve coagulation of superficial vessels, so no anesthesia is needed. However, patients with deep partial-thickness burns may still have pain sensation and require analgesia with IV opioids.
With proper escharotomy, the incision immediately bulges wide open as the pressure is relieved; failure to demonstrate this indicates the incision was too shallow (or that the eschar was nonconstricting).
References
1. Kagan RJ, Peck MD, Ahrenholz DH, et al. Surgical management of the burn wound and use of skin substitutes: An expert panel white paper. J Burn Care Res. 2013;34(2):e60–e79. doi: 10.1097/BCR.0b013e31827039a6
2. International Society for Burn Injury (ISBI) Practice Guidelines Committee, Steering Committee, Advisory Committee: ISBI practice guidelines for burn care. Burns. 2016;42(5):953–1021. doi: 10.1016/j.burns.2016.05.013
3. Romanowski KS, Carson J, Pape K, et al. American Burn Association Guidelines on the Management of Acute Pain in the Adult Burn Patient: A Review of the Literature, a Compilation of Expert Opinion, and Next Steps. J Burn Care Res. 2020 Nov 30;41(6):1129-1151. doi: 10.1093/jbcr/iraa119. PMID: 32885244; PMCID: PMC7703676.
4. Singer AJ, Beto L, Singer DD, et al. Association between burn characteristics and pain severity. Am J Emerg Med. 2015;33(9):1229-1231. doi:10.1016/j.ajem.2015.05.043
Drug Information for the Topic





