



Bunion is a prominence of the medial portion of the head of the first metatarsal bone. The cause is often a combination of a genetic predisposition and biomechanical factors related to the position of the first metatarsal bone or great toe leading to lateral angulation of the great toe (hallux valgus). Laxity at the first tarsometatarsal joint allows the metatarsal to rotate in the frontal plane, which causes the hallux to deform in the transverse plane and angulate laterally. Secondary osteoarthritis and spur formation are common. Symptoms may include pain and redness, bursitis medial to the joint, and mild synovitis. Diagnosis is usually clinical. Treatment is usually a shoe with a wide toe box, protective pads, and orthotics. For bursitis or synovitis, glucocorticoid injection may be helpful. Surgical intervention may be considered for refractory pain and difficulty with ambulation.
(See also Overview of Foot and Ankle Disorders.)
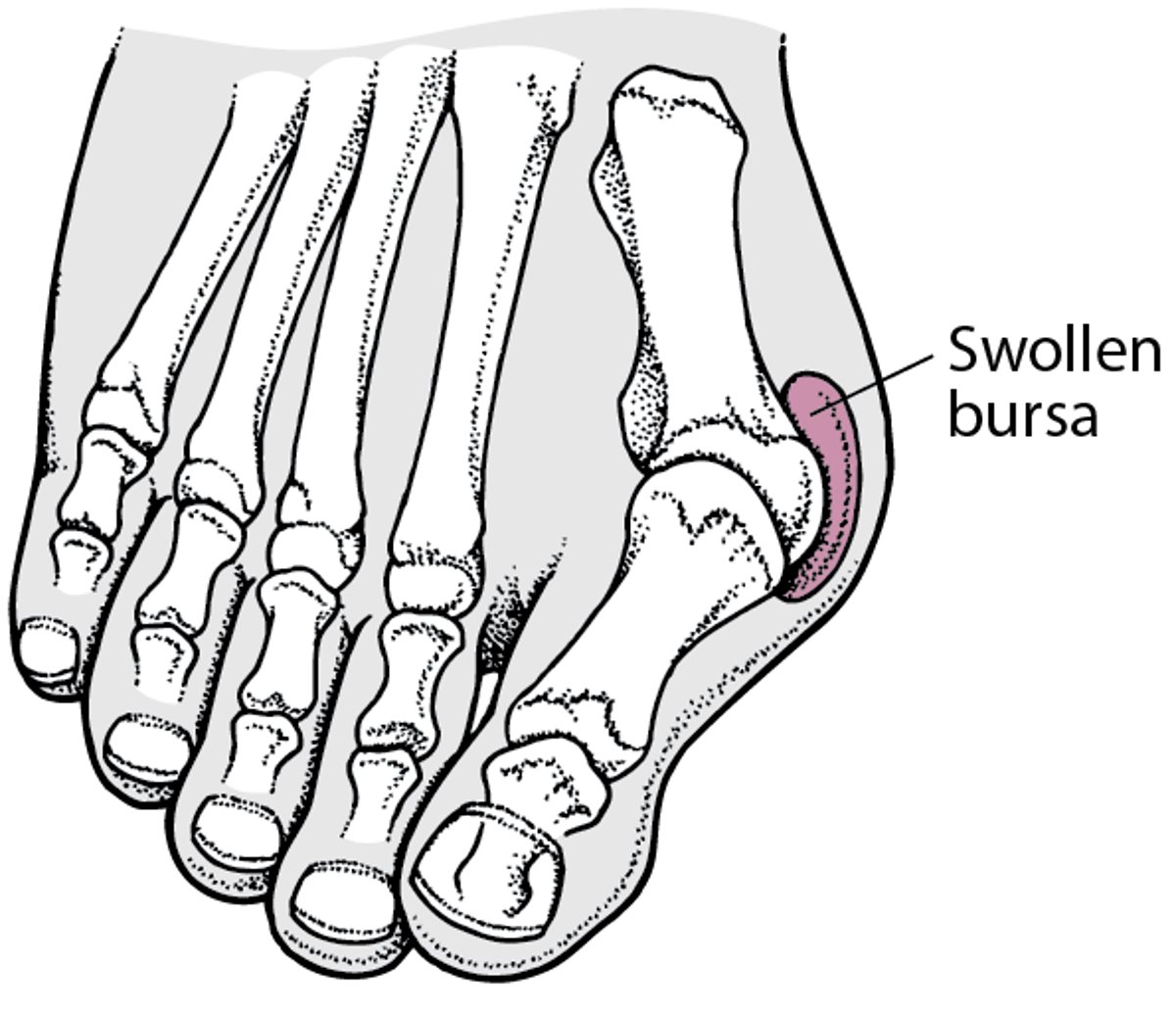
Contributing factors may include a genetic predisposition, excessive foot pronation, wearing tight and pointed-toe shoes, and trauma. Joint misalignment causes osteoarthritis with cartilage erosion and exostosis formation, resulting in joint motion being limited (hallux limitus) or eliminated (hallux rigidus). Mild synovitis may occur, causing joint swelling. Tight footwear can exacerbate symptoms, and an adventitious bursa can develop medial to the joint prominence, which can become painful, swollen, and inflamed (see figure ).


This anteroposterior view of the foot shows radiographic findings consistent with hallux valgus, with medial deviation of the first metatarsal. There is also lateral subluxation of the base of the first proximal phalanx with respect to the head of the first metatarsal.
Image courtesy of James C. Connors, DPM.
Bunion
A bunion (hallux valgus) is a lateral deviation of the hallux (first toe) on the first metatarsal. |

Symptoms and Signs of Bunion
The initial symptom of bunion may be pain at the joint prominence when wearing certain shoes. The joint capsule may be tender at any stage. Later symptoms may include a painful, warm, erythematous, cystic, movable, fluctuant swelling located medially (adventitial bursitis) and swellings and mild inflammation affecting the entire joint, which is more circumferential. With hallux limitus or rigidus, there is restriction of passive joint motion, tenderness at the dorsolateral aspect of the joint, and increased dorsiflexion of the distal phalanx.
Diagnosis of Bunion
Primarily history and physical examination

The diagnosis of a bunion is clinical; it is easily recognized on physical examination.
The presence of acute circumferential intense pain, warmth, swelling, and erythema suggests alternative or superimposed diagnoses such as gouty arthritis or infectious arthritis, which may mandate examination of synovial fluid. If multiple joints are affected, the presence of gout or another systemic rheumatic disease should also be considered.
Radiographs are generally not needed for diagnostic purposes, but weight-bearing views may be helpful in determining the extent and severity of damage to the first metatarsophalangeal joint. Suggestive findings include joint space narrowing and bony spurs extending from the metatarsal head or sometimes from the base of the proximal phalanx. On the anteroposterior (AP) radiographic view, the first metatarsal will be deviated medially, which causes the metatarsal head to be prominent in the medial soft tissue. The hallux is angulated laterally and causes excessive wear on the articular surface of the lateral aspect of the metatarsal head. The lateral sesamoid will appear in the intermetatarsal space. The hallux may abut the second digit and, in cases of severe deformity, the hallux may overlap or underlap the second toe.
Treatment of Bunion
Wide toe box, bunion pads, orthotics, or a combination
Sometimes, surgical treatment of complications
Mild discomfort may lessen by wearing a shoe with a wide toe box or with stretchable material. If not, bunion pads can shield the painful area. Toe spacers can also be tried. Orthotics can also be prescribed to redistribute and relieve pressure from the affected articulation.
If conservative therapy fails, surgery aimed at correcting abnormal bony alignments and restoring joint mobility should be considered. If the patient is unwilling to wear large, wider shoes to accommodate the bunion, surgery can be considered; however, patients should be told that orthotic devices should be worn after surgery to reduce the risk of recurrence.
For an associated bursitis, bursal aspiration and injection of a glucocorticoid may relieve pain (see Considerations for Using Glucocorticoid Injections).
For joint pain, oral nonsteroidal anti-inflammatory drugs (NSAIDs) or an intra-articular injection of a glucocorticoid combined with an anesthetic solution may help with analgesia.
For hallux limitus or hallux rigidus, treatment usually consists of orthotics or shoes that reduce motion or stress at the first metatarsophalangeal joint. Some patients may experience pain relief from a glucocorticoid injection. Sometimes surgical interventions (eg, osteotomy, arthrodesis) may be appropriate for patients with pain refractory to conservative measures.
Key Points
Excessive turning in (supination) of the ankles, wearing tight and pointed-toe shoes, and occasionally trauma increase the risk of prominences at the medial first metatarsophalangeal joints (bunions).
Symptoms can include pain, synovial or cystic swelling, and limitation of passive joint motion.
Use clinical findings to confirm the diagnosis.
Weight-bearing foot radiographs are useful to determine the severity of the deformity.
Treat initially with a wide or expansile toe box, toe spacers, bunion pads, orthotics, or a combination.
Reserve surgery for correction of abnormal bony alignment and restoration of joint mobility if conservative therapy is not effective.





