



Brain herniation occurs when increased intracranial pressure causes the abnormal protrusion of brain tissue through openings in rigid intracranial barriers (eg, tentorial notch).
Because the skull is rigid after infancy, intracranial masses or swelling may increase intracranial pressure, sometimes causing protrusion (herniation) of brain tissue through one of the rigid intracranial barriers (tentorial notch, falx cerebri, foramen magnum). When intracranial pressure is increased sufficiently, regardless of the cause, Cushing reflex and other autonomic abnormalities can occur. Cushing reflex includes systolic hypertension with increased pulse pressure, irregular respirations, and bradycardia.
Brain herniation is life threatening.
Brain herniation is classified based on the structure through which tissue is herniated. Types include the following (see figure ):
Transtentorial (uncal)
Subfalcine
Central
Upward transtentorial
Tonsillar
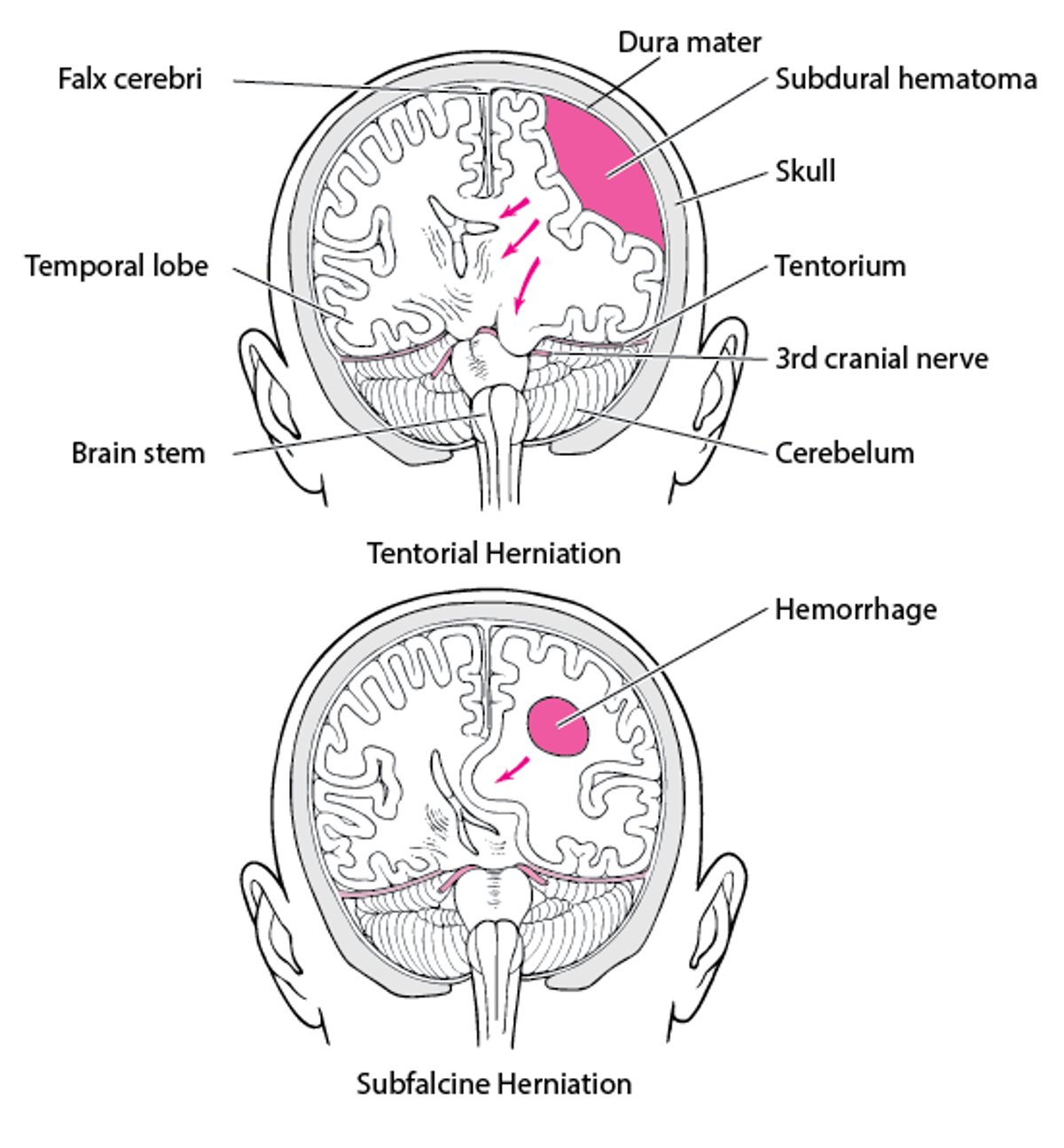
Brain Herniation
Increased intracranial pressure sometimes causes protrusion (herniation) of brain tissue through one of the rigid intracranial barriers (tentorial notch, falx cerebri, foramen magnum). Brain herniation is classified based on the structure through which tissue is herniated:
|

Transtentorial herniation
The medial temporal lobe is squeezed by a unilateral mass across and under the tentlike tentorium that supports the temporal lobe. The herniating lobe compresses the following structures:
Ipsilateral third cranial nerve (often first) and posterior cerebral artery
As herniation progresses, the ipsilateral cerebral peduncle
In about 5% of patients, the contralateral third cranial nerve and cerebral peduncle
Eventually, the upper brain stem and the area in or around the thalamus
Subfalcine herniation
The cingulate gyrus is pushed under the falx cerebri by an expanding mass high in a cerebral hemisphere. In this process, one or both anterior cerebral arteries become trapped, causing infarction of the paramedian cortex. As the infarcted area expands, patients are at risk of transtentorial herniation, central herniation, or both.
Central herniation
Both temporal lobes herniate through the tentorial notch because of bilateral mass effects or diffuse brain edema. Ultimately, brain death occurs.
Upward transtentorial herniation
Upward transtentorial herniation can occur when an infratentorial mass (eg, tumor in the posterior fossa, cerebellar hemorrhage) compresses the brain stem, kinking it and causing patchy brain stem ischemia. The posterior third ventricle becomes compressed. Upward herniation also distorts the mesencephalon vasculature, compresses the veins of Galen and Rosenthal, and causes superior cerebellar infarction due to occlusion of the superior cerebellar arteries.
Tonsillar herniation
Usually, tonsillar herniation is caused by an expanding infratentorial mass (eg, cerebellar hemorrhage). The cerebellar tonsils, forced through the foramen magnum, compress the brain stem and obstruct cerebrospinal fluid (CSF) flow.
Etiology of Brain Herniation
Brain herniation is a complication of a disorder that causes increased intracranial pressure (ICP). Increased intracranial pressure may be caused by
Space-occupying lesions (eg, brain tumor, edema, or abscess; contusions; hematomas)
Generalized swelling or edema of the brain (eg, due to acute liver failure or hypertensive encephalopathy)
Increased venous pressure (eg, due to heart failure, obstruction of superior mediastinal or jugular veins, or venous sinus thrombosis)
Obstruction of the CSF flow (eg, due to hydrocephalus or extensive meningeal disease)
Symptoms and Signs of Brain Herniation
Symptoms and signs of brain herniation are listed in the table below. Usually, patients also have signs of the disorder causing herniation; these signs can be nonspecific (eg, impaired consciousness, lethargy).
Effects of Brain Herniation
Type of Herniation | Mechanism* | Findings |
|---|---|---|
Transtentorial | Compression of ipsilateral third cranial nerve | Unilateral dilated, fixed pupil Oculomotor paresis |
Compression of the posterior cerebral artery | Contralateral homonymous hemianopia Absence of blinking in response to visual threat from the hemianopic side in obtunded patients | |
Compression of the contralateral third cranial nerve and cerebral peduncle (indented by the tentorium to form Kernohan notch) | Contralateral dilated pupil and oculomotor paresis Ipsilateral hemiparesis | |
Compression of the ipsilateral cerebral peduncle | Contralateral hemiparesis | |
Eventually, compression of the upper brain stem and the area in and around the thalamus | Impaired consciousness Abnormal breathing patterns Fixed, unequal pupils | |
Further compromise of the brain stem | Loss of oculocephalic reflex Loss of oculovestibular reflex Loss of corneal reflexes Decerebrate posturing | |
Subfalcine (cingulate) | Trapping of one or both anterior cerebral arteries, causing infarction of the paramedian cortex | Contralateral leg paralysis |
Expansion of infarcted area | Increased intracranial pressure Increased risk of transtentorial herniation, central herniation, or both | |
Central | Bilateral, more or less symmetric damage to the midbrain | Pupils fixed in midposition Decerebrate posturing Many of the same symptoms as transtentorial herniation |
Further compromise of the brain stem | Loss of all brain stem reflexes Disappearance of decerebrate posturing Cessation of respirations Brain death | |
Upward transtentorial | Compression of the posterior third ventricle | Hydrocephalus, which increases intracranial pressure |
Distortion of the mesencephalon vasculature Compression of the veins of Galen and Rosenthal Superior cerebellar infarction due to occlusion of the superior cerebellar arteries | Early: Nausea, vomiting, occipital headache, ataxia Later: Somnolence, breathing abnormalities, patchy and progressive loss of brain stem reflexes | |
Posterior fossa mass (eg, cerebellar hemorrhage) | Ataxia, dysarthria | |
Progressive brain stem compression | Increasing somnolence Respiratory irregularities Patchy but progressive loss of brain stem reflexes | |
Tonsillar | Compression of the brain stem Obstruction of cerebrospinal fluid (CSF) flow | Acute hydrocephalus (with impaired consciousness, headache, vomiting, and meningismus) Dysconjugate eye movements, nystagmus Later, abrupt respiratory and cardiac arrest |
* Not all mechanisms occur in every patient. | ||
CNS = central nervous system. | ||
Diagnosis of Brain Herniation
CT or MRI
After the patient is stabilized, brain imaging with CT or MRI is required to check for mass lesions and help identify displacement of brain tissue and the type of herniation.

Subfalcine herniation is the most common type of cerebral herniation. In this image, the left brain has herniated under the free edge of the falx cerebri (arrow) because hemorrhage from an infarct in the middle cerebral artery has increased intracerebral pressure.
© 2017 Elliot K. Fishman, MD.
Treatment of Brain Herniation
Immediate stabilization (airway, breathing, circulation, or ABCs)
Admission to an intensive care unit (ICU)
Supportive measures, including control of ICP
Treatment of underlying disorder
Treatment of brain herniation is similar to treatment of coma. The cause of brain herniation is treated when possible.
Hypotension must be corrected. Patients are admitted to the ICU so that respiratory and neurologic status can be monitored.
Patients must be stabilized. Airway, breathing, and circulation must be ensured immediately.
If increased ICP is suspected, intubation should be considered. Intubation is indicated if herniation is confirmed or airway protection is necessary (1).
If indicated, intubation uses a rapid-sequence oral intubation (using a paralytic medication) protocol rather than nasotracheal intubation; nasotracheal intubation in a patient who is breathing spontaneously causes more coughing and gagging, thus increasing ICP, which is already increased because of intracranial abnormalities.
If ICP is increased, intracranial and cerebral perfusion pressure should be monitored (see Intracranial Pressure Monitoring) (1), and pressures should be controlled. The goal is to maintain ICP at ≤ 20 mm Hg and cerebral perfusion pressure at 50 to 70 mm Hg. Cerebral venous drainage can be enhanced (thus lowering ICP) by elevating the head of the bed to 30° and by keeping the patient’s head in a midline position.
Measures to control ICP include (2)
Sedation: Sedatives may be necessary to control agitation, excessive muscular activity (eg, due to delirium), or pain, which can increase ICP.
Hyperventilation: Hyperventilation causes hypocapnia, which causes vasoconstriction, thus decreasing cerebral blood flow globally.
Hydration: Isotonic fluids are used. Providing free water through IV fluids (eg, 5% dextrose, 0.45% saline) can aggravate cerebral edema and should be avoided. Fluids may be restricted to some degree, but patients should be kept euvolemic. If patients have no signs of dehydration or fluid overload, IV fluids with normal saline can be started at 50 to 75 mL/h. The rate can be increased or decreased based on serum sodium, osmolality, urine output, and signs of fluid retention (eg, edema).
Diuretics: Serum osmolality should be kept at 295 to 320 mOsm/kg. Osmotic diuretics (eg, mannitol) may be given IV to lower ICP and maintain serum osmolality. Osmotic diuretics do not cross the blood-brain barrier. They pull water from brain tissue across an osmotic gradient into plasma, eventually leading to equilibrium. Fluid and electrolyte balance should be monitored closely while osmotic diuretics are used. A 3% saline solution is another potential osmotic agent to control ICP.
Blood pressure (BP) control: Systemic antihypertensives (eg, calcium channel blockers) are needed only when hypertension is severe (> 180/95 mm Hg). How much BP is reduced depends on the clinical context. Systemic BP needs to be high enough to maintain cerebral perfusion pressure even when ICP increases.
Glucocorticoids: Glucocorticoids are effective only when vasogenic edema (due to disruption of the blood-brain barrier, as may result from tumors or abscesses) is present. Glucocorticoids are ineffective for cytotoxic edema (due to cell death and breakdown) and can increase plasma glucose, exacerbating cerebral ischemia.
Removal of cerebrospinal fluid (CSF): When ICP is increased, CSF can be removed at periodic intervals; it is removed slowly, at a reduced rate of 1 to 2 mL/minutes to help lower ICP.
Position: Positioning the patient to maximize venous outflow from the head can help minimize increases in ICP. The head of the bed can be elevated to 30° (with the head above the heart) as long as cerebral perfusion pressure remains at the desired range. The patient’s head should be kept in a midline position, and neck rotation and flexion should be minimized. Tracheal suctioning, which can increase ICP, should be limited.
If ICP continues to increase despite other measures to control it, the following may be used:
Titrated hypothermia: When ICP is increased after head trauma or cardiac arrest, hypothermia in the range of 32 to 35° C has been used to reduce ICP to < 20 mm Hg. While several studies conflict about the benefit of hypothermia, a meta-analysis of over 50 trials suggests likely benefit for therapeutic hypothermia in adults but does not recommend its use in children (3).
Pentobarbital coma: Pentobarbital can reduce cerebral blood flow and metabolic demands. However, its use is controversial because treatment with pentobarbital can lead to complications (eg, hypotension) and clinical outcomes of pentobarbital coma are inconsistent; lack of early response to pentobarbital predicts poor outcomes (4). In some patients with refractory intracranial hypertension that does not respond to standard hyperventilation and hyperosmolar therapy, pentobarbital can improve functional outcome.
Decompressive craniotomy: Craniotomy with duraplasty can be done to provide room for brain swelling. This procedure can prevent deaths, but overall functional outcome may not greatly improve, and it may lead to complications such as hydrocephalus (5). It may be most useful for large cerebral infarcts with impending herniation, particularly in patients < 50 years.
Brain herniation due to tumors is treated with mannitol, a glucocorticoid (eg, dexamethasone), and endotracheal intubation. Hyperventilation to a carbon dioxide partial pressure (PCO2) of 26 to 30 mm Hg can help decrease ICP temporarily in emergencies. Mass lesions should be surgically decompressed as soon as possible.
Treatment references
1. Le Roux P, Menon DK, Citerio G, et al. Monitoring in Neurocritical Care: A statement for healthcare professionals from the Neurocritical Care Society and the European Society of Intensive Care Medicine. Neurocrit Care. 21 Suppl 2 (Suppl 2):S1–26, 2014. doi: 10.1007/s12028-014-0041-5
2. Cook AM, Jones GM, Hawryluk GWJ, et al. Guidelines for the acute treatment of cerebral edema in neurocritical care patients. Neurocrit Care. 32 (3):647–666 2020. doi: 10.1007/s12028-02-00959-7
3. Crompton EM, Lubomirova I, Cotlarciuc I, Han TS, Sharma SD, Sharma P. Meta-Analysis of Therapeutic Hypothermia for Traumatic Brain Injury in Adult and Pediatric Patients. Crit Care Med. 2017;45(4):575-583. doi:10.1097/CCM.0000000000002205
4. Stansbury BM, Kelley CJ, Rudy RF, et al. Pentobarbital coma for management of intracranial hypertension following traumatic brain injury: Lack of early response to treatment portends poor outcomes. Am J Surg. 2023;226(6):864-867. doi:10.1016/j.amjsurg.2023.07.011
5. Su TM, Lan CM, Lee TH, Hsu SW, Tsai NW, Lu CH. Risk factors for the development of posttraumatic hydrocephalus after unilateral decompressive craniectomy in patients with traumatic brain injury. J Clin Neurosci. 2019;63:62-67. doi:10.1016/j.jocn.2019.02.006
Key Points
Brain herniation results from increased intracranial pressure (ICP), which may be caused by space-occupying lesions, generalized swelling or edema of the brain, increased venous pressure, or obstruction of cerebrospinal flow (CSF) flow.
Specific symptoms vary based on which structures are compressed; patients also have impaired consciousness and other neurologic deficits caused by the disorder causing herniation.
After stabilizing the patient, do brain imaging with CT or MRI.
Monitor and control ICP using sedatives, endotracheal intubation, hyperventilation, hydration, diuretics, measures to control blood pressure, and sometimes glucocorticoids.
Treat the cause when possible.
Drug Information for the Topic





