



Voluntary movement requires complex interaction of the corticospinal (pyramidal) tracts, basal ganglia, and cerebellum (the center for motor coordination) to ensure smooth, purposeful movement without extraneous muscular contractions.
The pyramidal tracts pass through the medullary pyramids to connect the cerebral cortex to lower motor centers of the brain stem and spinal cord.
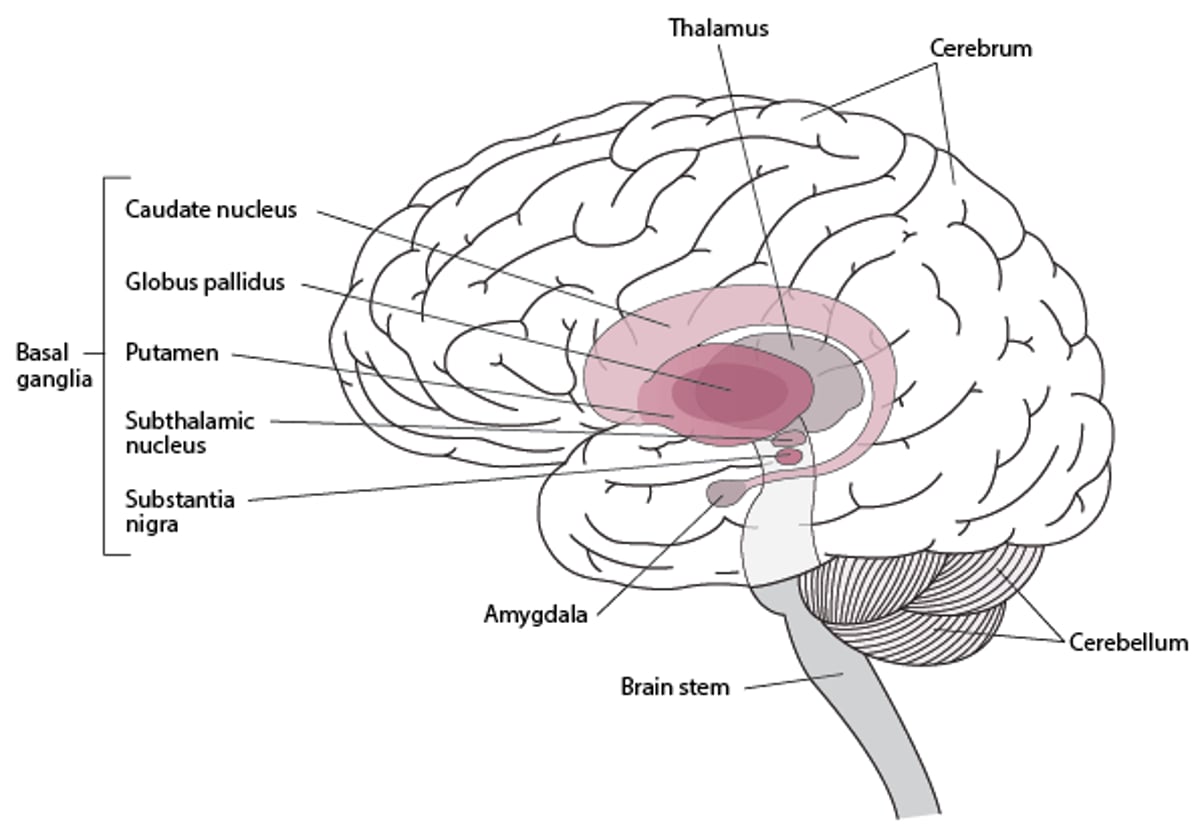
The basal ganglia (caudate nucleus, putamen, globus pallidus, subthalamic nucleus, and substantia nigra) form the extrapyramidal system. They are located deep in the forebrain and rostral midbrain. The basal ganglia direct their output mainly through the thalamus to the cerebral cortex (see figure ). Two main motor functions are integrated in the basal ganglia:
Operational learning (motor tasks)
Task selection (whether single, dual, or multiple as when walking and speaking)
Most neural lesions that cause movement disorders occur in the extrapyramidal system; thus, movement disorders are sometimes called extrapyramidal disorders.



Basal Ganglia

Classification of Movement and Cerebellar Disorders
Movement disorders are commonly classified as those with
Decreased or slow movement (hypokinetic disorders)
Increased movement (hyperkinetic disorders)
The classic and most common hypokinetic disorder is
Hyperkinetic disorders include
Chorea (including hemiballismus [rapid chorea] and athetosis [slow chorea])
Stereotypies
Akathisia
However, this classification does not account for overlap between categories (eg, tremors that occur in Parkinson disease).
Cerebellar disorders are sometimes considered hyperkinetic disorders often accompanied by axial, gait, and appendicular ataxia with or without central nystagmus, ocular saccadic dysmetria, and ocular pursuit dysfunction.
Hyperkinetic disorders
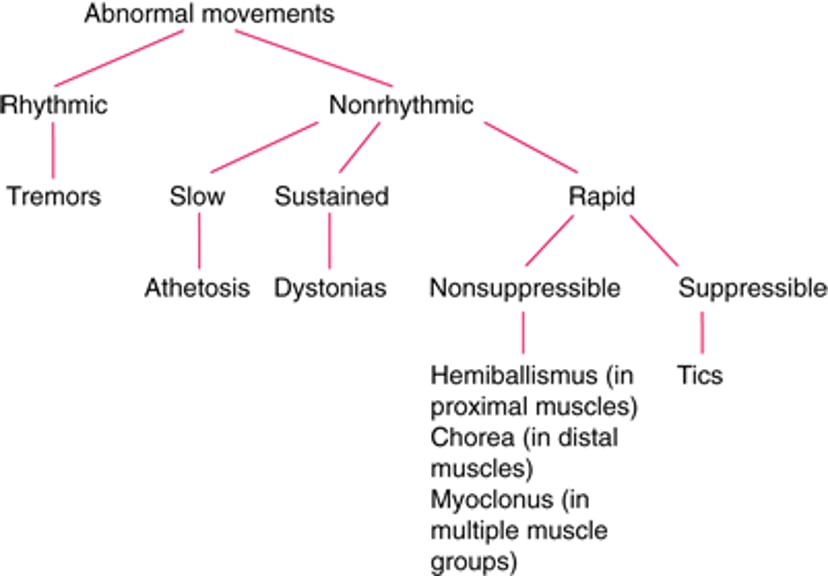
Hyperkinetic disorders (see figure and table ) can be
Rhythmic
Nonrhythmic
Rhythmic disorders are primarily tremors—regular alternating or oscillatory movements, which can occur mainly at rest, or while maintaining a position, and/or during attempted movement. However, in some cases, a tremor, though rhythmic, is irregular, as occurs when tremor is associated with dystonic disorders.
Nonrhythmic hyperkinetic disorders can be
Slow (eg, athetosis)
Sustained (eg, dystonias)
Rapid (eg, myoclonus, chorea, tics, hemiballismus)
Rapid nonrhythmic hyperkinetic disorders may be
Suppressible (eg, tics)
Nonsuppressible (eg, hemiballismus, chorea, myoclonus)
Athetosis and chorea may occur together as choreoathetosis. Chorea is the most characteristic movement disorder in Huntington disease.
Multiple motor and phonatory tics are the defining feature of Tourette syndrome.
Classification of Common Hyperkinetic Disorders

Hyperkinetic Disorders
Abnormal Movement | Causes | Description |
|---|---|---|
Akathisia (motor restlessness) | Parkinson disease, traumatic brain injury, encephalitis Antipsychotic medications, some antiemetics, antidepressants, calcium channel blockers | Patients with akathisia cannot remain still; they have an urge to move continuously (eg, forward rocking, lateral swaying). |
Huntington disease, encephalitis, hepatic encephalopathy Medications and substances (eg, cocaine, amphetamines, antipsychotics) | Movements are nonrhythmic, slow, writhing, and sinuous (snakelike), primarily in distal muscles; alternating postures of the proximal limbs often blend continuously to produce a flowing stream of movement. | |
Huntington disease, hyperthyroidism, hypoparathyroidism, hyperglycemia and, less commonly, hypoglycemia, paraneoplastic syndromes, systemic lupus erythematosus (SLE) affecting the CNS, other autoimmune disorders, rheumatic fever, tumors or infarcts of the caudate nucleus or putamen Pregnancy, often in women who had rheumatic fever Medications and substances that can cause chorea (eg, levodopa, phenytoin, cocaine, oral contraceptives) Medications that can cause tardive dyskinesia (eg, antipsychotics) | Movements are random, flowing, and nonsuppressible, going from one place to another, primarily in distal muscles or the face. Sometimes abnormal movements are incorporated into semipurposeful acts that mask the involuntary movements (parakinesia). Chorea often occurs with athetosis as choreoathetosis. | |
Dystonias | Primary (idiopathic) Degenerative or metabolic disorders (eg, Wilson disease, neurodegeneration with brain iron accumulation [NBIA] such as PKAN due to a PANK2 mutation [previously, Hallervorden-Spatz disease], various lipidoses, multiple sclerosis, cerebral palsy, stroke, brain hypoxia) Medications that block dopamine receptors, most often antipsychotics (eg, phenothiazines, thioxanthenes, butyrophenones) or antiemetics Brain damage in the basal ganglia and their circuits due to any condition (eg, vascular, posttraumatic, postinfectious, or inflammatory causes; tumors) | Sustained or intermittent muscle contractions often distort body posture or cause twisting, repetitive movements. |
Lesions (most often due to stroke) in the contralateral subthalamic nucleus or in connecting afferent or efferent pathways | Movements are nonrhythmic, rapid, nonsuppressible, violent, and flinging. | |
Various causes (eg, degeneration of the basal ganglia, dementias, epileptic syndromes, metabolic disturbances, physical and hypoxic encephalopathies, toxic encephalopathies, viral encephalopathies, certain medications such as levodopa, lithium, and MAO inhibitors) | Very rapid and jerky, nonsuppressible, shocklike twitches occur; they may be focal, segmental, or generalized. | |
Primary (idiopathic or familial) Secondary: Parkinson disease, uremia, iron deficiency, peripheral neuropathies | Legs feel uncomfortable, and patients have an irresistible urge to move the legs. Discomfort lessens significantly when the legs are moved; discomfort is worse at night (diurnal variability). Many patients also have periodic limb movement disorder (involuntary jerking of the legs and arms) during sleep. | |
Stereotypies (stereotypic movements) | Autism spectrum disorders, intellectual disability, limbic autoimmune or paraneoplastic encephalitis; can also occur in normal children | Repetitive rhythmic movements occur; they are usually bilateral (eg, hand flapping, waving) or behaviors (eg, sniffing, vocalizing, posturing) Preschool stereotypies occur in 3–4% of patients; they are benign and are typically stopped by distraction (eg, calling the child's name). |
Tardive dyskinesia | Antipsychotics, some antiemetics | Movements are stereotypic and cannot be voluntarily suppressed; consciousness is preserved. |
Tics | Primary: Tourette syndrome Secondary: Huntington disease, neuroacanthocytosis, PKAN, infections, stroke, medications and substances (eg, methylphenidate, cocaine, amphetamines, dopamine antagonists [which can cause tardive dyskinesias]) | Movements are nonrhythmic, stereotypic, rapid, and repetitive; characteristically, patients have an urge to do them and feel brief relief after doing them. Tics can be suppressed only for brief periods and with conscious effort. Tics may be motor or phonatory; they may be simple (eg, eye blinking, growling, clearing the throat) or complex (eg, shoulder shrugging, arm swinging, shouting words or sentences, including obscenities). |
Essential tremor Wilson disease Certain medications (eg, lithium, valproate, olanzapine, other typical and atypical antipsychotics—see table Some Causes of Secondary and Atypical Parkinsonism) Withdrawal syndromes (eg, from alcohol, opioids, or sedatives) Endocrine, metabolic, and toxic disorders (eg, anoxic encephalopathy, hepatic encephalopathy, hypoglycemia, hyperparathyroidism, hyperglycemia, hyperthyroidism, hypocalcemia, uremia, heavy metal toxicity) Physiologic | Movements are regular, mostly rhythmic, and oscillatory. | |
CNS = central nervous system; MAO = monoamine oxidase; PKAN = pantothenate kinase‒associated neurodegeneration; PANK2 = pantothenate kinase 2. | ||





