Clinicians should evaluate the cause, severity, and nature of the pain and its effect on activities, mood, cognition, and sleep. Evaluation of the cause of acute pain (eg, back pain, chest pain) differs from that of chronic pain.
(See also Overview of Pain.)
The history should include the following information about the pain:
Timing (onset, persistence [whether constant or intermittent], pattern and degree of fluctuation and frequency of remissions, duration)
Quality (eg, sharp, dull, crampy, burning, aching, shooting)
Severity
Location (localized, diffuse, deep, superficial)
Radiation pattern
Exacerbating and relieving factors
Information from the history and physical examination help guide the choice of laboratory and imaging tests to identify possible causes of pain.
If pain becomes chronic, the evaluation should be more comprehensive. The goal of the chronic pain evaluation is to establish a diagnosis and identify comorbid conditions that may be exacerbating the pain. The evaluation should also elucidate the patient's history and the meaning they ascribe to the pain, identify the functional limitations the pain is causing, and ascertain the patient's goals and beliefs regarding treatment.
The Stanford 5 provides a useful framework for the clinician to quickly understand the patient's concerns regarding their pain, which may also help ensure greater treatment success (1). Using this approach, health care professionals should specifically ask about the following:
Cause: What tissue abnormalities the patient believes to be the cause of the current problem
Meaning: The reason why the patient believes they have this pain
Goals: What the patient expects to achieve with further treatment
Treatment: What the patient believes needs to be done now and in the future to help resolve the problem
Impact: What impact the primary problem has on the patient's life, including interference in vocational, social, and recreational activities, as well as the general effect it has on the patient's quality of life
Further assessment of chronic pain should be performed using patient-reported outcome tools that can help assess sleep and psychological dysfunction (eg, depression, anxiety, and PTSD). There are various patient-reported outcome tools available and the choice of tool depends on the specific domains of interest and the clinical context. The National Institutes of Health has developed the Patient-Reported Outcomes Measurement Information (PROMIS) tool, which can be used to assess different aspects of the patient's pain experience. These computer-adaptive tests aim to minimize patient burden and provide clinicians and researchers with standardized to normative data to replace the confusing multitude of other tests that have been used in the past (2). The results of these assessments serve as the basis for discussing patient function, social support, lifestyle, and psychological challenges.
Clinicians should assess the patient’s level of function and the pain's effect on function, focusing on activities of daily living (eg, dressing, bathing), employment, avocations, and personal relationships (including sexual). It is important to assess these functional levels repeatedly and to use them as markers for improvement throughout the course of treatment.
Psychological evaluation is a key component of pain assessment. Depression and anxiety are the most common mental health conditions that co-occur in patients with chronic pain. The relationship between these conditions and pain is bidirectional. Pain increases risk of a mood or anxiety disorder, and mood and anxiety disorders increase the risk of chronic pain. Other key factors to consider include adverse childhood experiences, history of trauma, expectations of treatment, ongoing life stressors, and history of or current substance use disorders. Appreciating cultural norms and attitudes in different patient subpopulations is important in interpreting these data.
In some patients, secondary gain (eg, time off, disability payments) may contribute to pain or pain-related disability; thus, asking about potential legal issues associated with their pain may be helpful.
Patients and sometimes family members and caregivers should be asked about the use, efficacy, and adverse effects of prescription and over-the-counter medications and other treatments. If misuse of opioids or other substances is suspected, further evaluation is required.
A physical examination focusing on neurological and psychiatric components is done and should include observation of the patient, basic mental status examination, inspection and palpation of tender areas, and testing of joint range of motion, strength, reflexes and tone, sensory function, coordination, and gait.
Studies including imaging, EEG, EMG, and autonomic nervous system testing are done to validate and supplement the history and physical examination.
Of note, clinicians should be aware of various factors that could result in inadequate pain management in populations that have certain characteristics (3):
Racial and ethnic minorities: There are differences in pain treatment across racial and ethnic groups, influenced by communication barriers, access to care, and variations in pain expression. Standardized assessment tools and culturally informed care can help reduce disparities.
Older adults: Pain in older adults is often underrecognized, partly due to assumptions that it is a normal part of aging. Cognitive impairment and altered pain perception further complicate assessment, requiring careful evaluation and tailored treatment.
Sex and gender differences: Women report higher rates of chronic pain but are sometimes undertreated or misdiagnosed due to differences in pain perception and provider biases. Hormonal influences also play a role in pain modulation.
Language barriers: Patients with limited English proficiency face challenges in expressing pain, leading to potential undertreatment. The use of professional interpreters and multilingual pain assessment tools is essential for equitable care.
Pain severity
Pain severity should be assessed before and after potentially painful interventions. In verbal patients, self-report is the gold standard, and external signs of pain or distress (eg, crying, wincing, rocking) are secondary. For patients who have difficulty communicating and for young children, nonverbal indicators (behavioral and sometimes physiologic) may need to be the primary source of information.
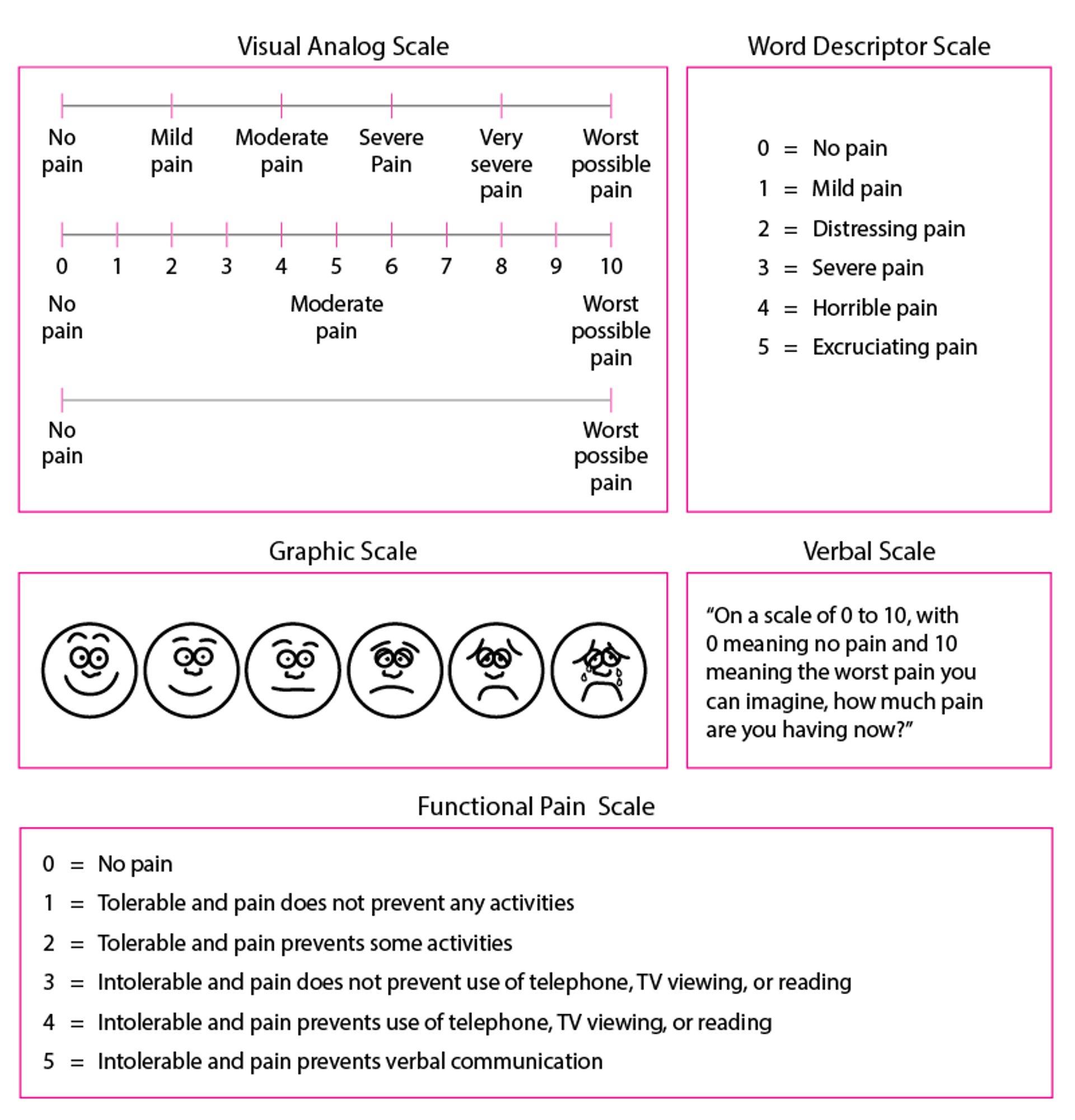
Formal measures (see figure ) include
Verbal category scales (eg, mild, moderate, severe)
Numeric scales
The Visual Analog Scale (VAS)
For a numeric scale, patients are asked to rate their pain from 0 to 10 (0 = no pain; 10 = “the worst pain ever”). For the VAS, patients make a hash mark representing their degree of pain on an unmarked 10-cm line with the left side labeled “no pain” and the right side labeled “unbearable pain.” The pain score is distance in mm from the left end of the line. Children and patients with limited literacy or known developmental problems may select from images of faces ranging from smiling to contorted with pain or from fruits of varying sizes to convey their perception of pain severity. When measuring pain, the examiner should specify a time period (eg, “on average during the past week”).
Some Pain Scales for Quantifying Pain as It Is Occurring
For the Functional Pain Scale, examiners should clearly explain to the patient that functional limitations are relevant to the evaluation only if they are due to the pain being evaluated; treatment aims to relieve pain as much as possible, at least to a tolerable level (0–2). Adapted from the American Geriatrics Society (AGS) Panel on Chronic Pain in Older Persons: The management of chronic pain in older persons. Journal of the American Geriatrics Society 46:635–651, 1998; used with permission; from Gloth FM III, Scheve AA, Stober CV, et al: The functional pain scale (FPS): Reliability, validity, and responsiveness in a senior population. Journal of the American Medical Directors Association 2 (3):110–114, 2001; and from Gloth FM III: Assessment. In Handbook of Pain Relief in Older Adults: An Evidence-Based Approach, edited by FM Gloth III. Totowa (NJ), Humana Press, 2003, p. 17; used with permission; copyright © FM Gloth, III, 2000. |

Patients with dementia or aphasia
Assessing pain in patients with disorders affecting cognition, speech, or language (eg, dementia, aphasia) can be difficult. Pain is suggested by facial grimacing, frowning, or repetitive eye blinking. Sometimes caregivers can describe behaviors that suggest pain (eg, sudden social withdrawal, irritability, grimacing). Pain should be considered in patients who have difficulty communicating and who inexplicably change their behavior. Many patients who have difficulty communicating can communicate meaningfully when an appropriate pain scale is used. For example, the Functional Pain Scale has been validated and can be used in nursing home patients who have Mini-Mental State Examination scores of ≥ 17.
Patients receiving neuromuscular blockade
No validated instruments are available to assess pain when neuromuscular blockade is used to facilitate mechanical ventilation.
If the patient is given a sedative, the dose can be adjusted until there is no evidence of consciousness. In such cases, specific analgesics are not needed. If, however, the patient is sedated but continues to have evidence of consciousness (eg, blinking, some eye movement, response to command), pain treatment should be considered based on the degree of pain usually caused by the condition (eg, burns, trauma). If a potentially painful procedure (eg, turning a bedbound patient) is required, pretreatment with the selected analgesic or anesthetic should be given.
References
1. Thernstrom M. The Pain Chronicles: Cures, Myths, Mysteries, Prayers, Diaries, Brain Scans, Healing, and the Science of Suffering. Farrar, Strauss and Giroux, New York, 2010. pp 220–223.
2. Bevans M, Ross A, Cella D. Patient-Reported Outcomes Measurement Information System (PROMIS): efficient, standardized tools to measure self-reported health and quality of life. Nurs Outlook. 2014;62(5):339-345. doi:10.1016/j.outlook.2014.05.009
3. Nguyen LH, Dawson JE, Brooks M, Khan JS, Telusca N. Disparities in Pain Management. Anesthesiol Clin. 2023 Jun;41(2):471-488. doi: 10.1016/j.anclin.2023.03.008
Key Points
Chronic pain assessment requires a thorough understanding of the patient's history, functional limitations, comorbidities, and the personal significance of their pain.
The Stanford 5 framework helps clinicians understand patients' views on the cause, meaning, goals, treatment expectations, and impact on life of their pain.
Clinicians should use standardized patient-reported outcomes tools to help assess various aspects of the patient's experience of pain.
Psychological evaluation is also a key component of pain assessment; depression and anxiety are the most common mental health conditions that co-occur in patients with chronic pain.
Assess pain severity before and after potentially painful interventions.