



Cytomegalovirus infection may be acquired prenatally or perinatally and is the most common congenital viral infection. Infection in neonates is associated with preterm delivery, low birthweight, microcephaly, jaundice, petechiae, hepatosplenomegaly, periventricular calcifications, chorioretinitis, pneumonitis, hepatitis, and sensorineural hearing loss. Infection acquired later in infancy is associated with pneumonia, hepatosplenomegaly, hepatitis, thrombocytopenia, sepsis-like syndrome, and atypical lymphocytosis. Diagnosis of neonatal infection is by nucleic acid amplification testing. Neonates with symptomatic cytomegalovirus are treated with oral valganciclovir to prevent hearing deterioration and improve neurodevelopmental outcomes; parenteral ganciclovir can be used if gastrointestinal absorption is unreliable.
Cytomegalovirus (CMV) is frequently isolated from neonates. Although most infants shedding this virus are asymptomatic, others have life-threatening illness and devastating long-term sequelae.
It is not known when a person with primary CMV can conceive and pose no risk to the fetus. For this reason, people who develop primary CMV before or during pregnancy should be counseled about risks to the fetus, but few experts recommend routine serologic testing for CMV before or during pregnancy (1).
(See also Cytomegalovirus Infection in adults.)
General reference
1. Practice bulletin no. 151: Cytomegalovirus, parvovirus B19, varicella zoster, and toxoplasmosis in pregnancy [published correction appears in Obstet Gynecol. 2016 Feb;127(2):405] [published correction appears in Obstet Gynecol. 2016 Feb;127(2):405. doi: 10.1097/01.AOG.0000480402.22371.a4.]. Obstet Gynecol. 2015;125(6):1510-1525. doi:10.1097/01.AOG.0000466430.19823.53
Etiology of Congenital and Perinatal CMV Infection
Congenital CMV infection, which occurs in approximately 5 in 1000 live births worldwide, may result from transplacental acquisition of either a primary or recurrent maternal infection (1). Clinically apparent disease in the neonate is much more likely to occur after a primary maternal infection, particularly in the first half of pregnancy. In the United States, approximately 40% of women age 20 to 49 lack antibody to CMV, making them susceptible to primary infection (2).
Perinatal CMV infection is acquired by exposure to infected cervical fluid, human milk, or blood products. Maternal antibody is thought to be protective, and most exposed term infants are asymptomatic or not infected. In contrast, preterm infants (who have received less maternal antibody to CMV) can develop serious infection or can die, particularly when transfused with CMV-positive blood. Efforts should be made to transfuse these infants with only CMV-negative blood or components or to use blood that has been filtered to remove leukocytes, which carry CMV. Such leukoreduced blood is considered by many experts to be CMV safe.
Etiology references
1. Pesch MH, Schleiss MR. Emerging Concepts in Congenital Cytomegalovirus. Pediatrics. 2022;150(2):e2021055896. doi:10.1542/peds.2021-055896
2. Bate SL, Dollard SC, Cannon MJ. Cytomegalovirus seroprevalence in the United States: the national health and nutrition examination surveys, 1988-2004. Clin Infect Dis. 2010;50(11):1439-1447. doi:10.1086/652438
Symptoms and Signs of Congenital and Perinatal CMV Infection
Many people who become infected with CMV during pregnancy are asymptomatic, but some develop a mononucleosis-like illness.
Approximately 13% of infants with congenital CMV infection have symptoms, signs, or complications at birth, including (1) the following:
Intrauterine growth restriction
Petechiae
Hepatosplenomegaly
Periventricular calcifications
Chorioretinitis
Hepatitis
Pneumonitis
Sensorineural hearing loss
Infants who acquire CMV during or after birth, especially if they are preterm, may develop a sepsis-like syndrome, pneumonia, hepatosplenomegaly, hepatitis (which can lead to liver failure), thrombocytopenia, and atypical lymphocytosis. However, if transmission is via human milk, the risk of severe symptomatic disease and long-term sequelae is low.
Symptoms and signs reference
1. Khalil A, Heath PT, Jones CE, Soe A, Ville YG; Royal College of Obstetricians and Gynaecologists. Congenital Cytomegalovirus Infection: Update on Screening, Diagnosis and Treatment: Scientific Impact Paper No. 56. BJOG. 2025;132(2):e42-e52. doi:10.1111/1471-0528.17966
Diagnosis of Congenital and Perinatal CMV Infection
Polymerase chain reaction (PCR) testing using urine, saliva, blood, or tissue
Viral culture using urine, saliva, or tissue
Symptomatic congenital CMV infection must be distinguished from other congenital infections, including toxoplasmosis, rubella, lymphocytic choriomeningitis, and syphilis.
In neonates, viral detection using culture or PCR of urine, saliva, blood, or a tissue sample is the primary diagnostic tool; maternal diagnosis can also be made by serologic testing or PCR (see Diagnosis of CMV). Congenital CMV infection is diagnosed if the virus (or viral nucleic acid) is identified in urine, saliva, or other body fluids obtained within the first 3 weeks of life; urine and saliva have the highest sensitivity. After 3 weeks, viral detection may indicate postnatal infection. Infants may shed CMV for several years after either type of infection.
Fetal CMV infection can be confirmed by PCR testing for CMV in the amniotic fluid.

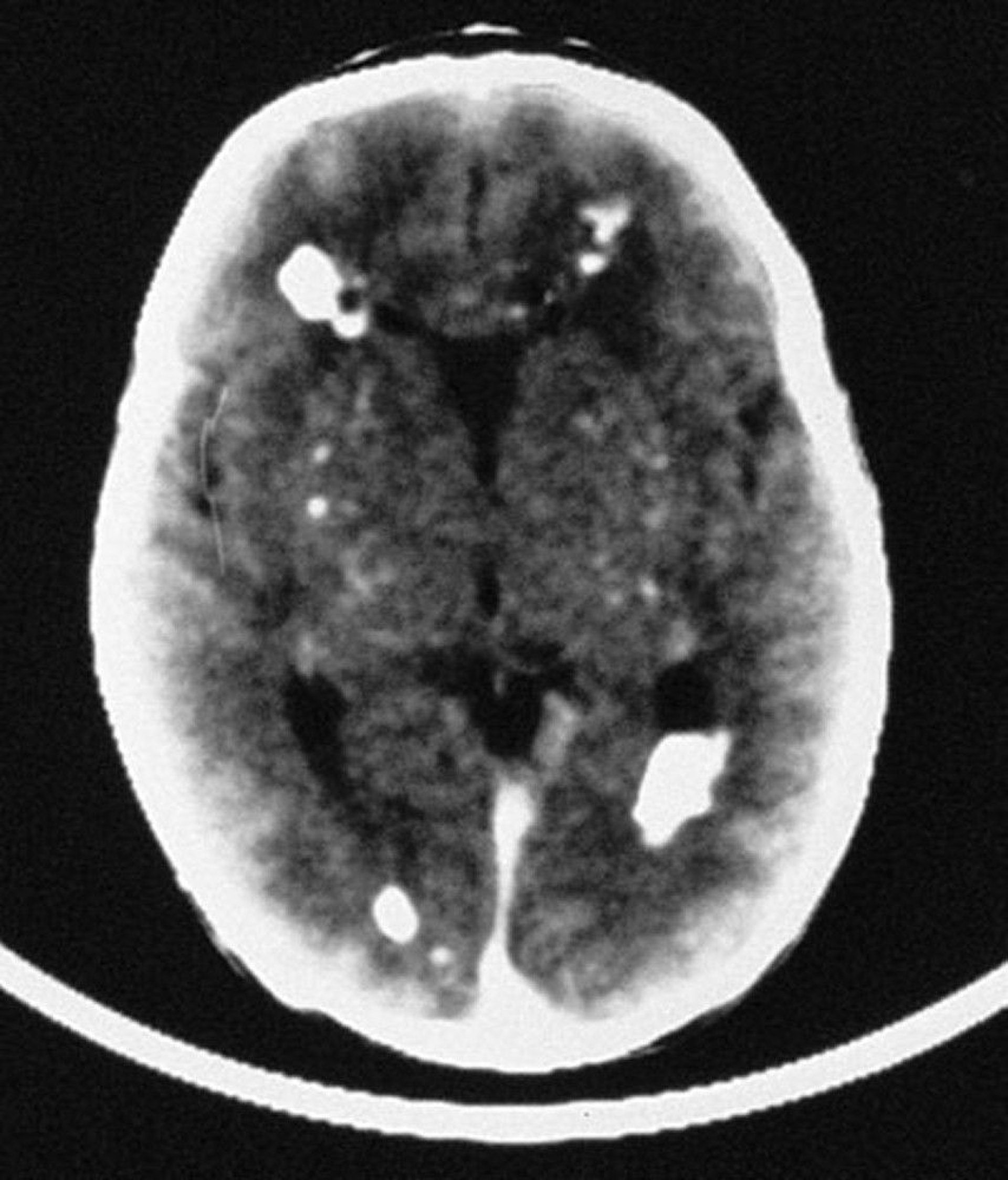
In this image, the CT scan reveals multiple intracranial calcifications, mostly periventricular in distribution, but also involving vascular structures of the brain.
By permission of the publisher. From Demmler G: Congenital and perinatal infections. In Atlas of Infectious Diseases: Pediatric Infectious Diseases. Edited by CM Wilfert. Philadelphia, Current Medicine, 1998.
A complete blood count (CBC) with differential and liver tests may be helpful but are not specific. Cranial ultrasound or CT and an ophthalmologic evaluation should also be performed. Periventricular calcifications are commonly found on CT.
Hearing tests should be routinely performed at birth in all infected neonates, and continued close monitoring is required because hearing loss may develop after the neonatal period and be progressive.
Treatment of Congenital and Perinatal CMV Infection
Ganciclovir or valganciclovir for symptomatic neonates
Symptomatic neonates are given antiviral medications. Oral valganciclovir for 6 months decreases viral shedding in neonates with congenital CMV and modestly prevents hearing deterioration and improves neurodevelopmental outcomes at 12 and 24 months of age (1); parenteral ganciclovir can be used if gastrointestinal absorption is unreliable.
In utero treatment of affected fetuses with acyclovir or valacyclovir may also improve neonatal outcomes, but large studies with long-term follow up are lacking.
The main toxicity of these medications is neutropenia.
Treatment reference
1. Kimberlin DW, Jester PM, Sánchez PJ, et al: Valganciclovir for symptomatic congenital cytomegalovirus disease. N Engl J Med 372(10):933–943, 2015. doi: 10.1056/NEJMoa1404599
Prognosis for Congenital and Perinatal CMV Infection
Symptomatic neonates have a mortality rate of up to 5 to 10% (1). Approximately 30 to 65% of survivors of symptomatic congenital CMV develop sensorineural hearing loss (2).
Among asymptomatic neonates, 5 to 15% eventually develop neurologic sequelae; hearing loss is the most common (3).
Prognosis references
1. Grosse SD, Fleming P, Pesch MH, Rawlinson WD. Estimates of congenital cytomegalovirus-attributable infant mortality in high-income countries: A review. Rev Med Virol. 2024;34(1):e2502. doi:10.1002/rmv.2502
2. Foulon I, De Brucker Y, Buyl R, et al. Hearing Loss With Congenital Cytomegalovirus Infection. Pediatrics. 2019;144(2):e20183095. doi:10.1542/peds.2018-3095
3. Smyrli A, Raveendran V, Walter S, et al. What are the neurodevelopmental outcomes of children with asymptomatic congenital cytomegalovirus infection at birth? A systematic literature review. Rev Med Virol. 2024;34(4):e2555. doi:10.1002/rmv.2555
Prevention of Congenital and Perinatal CMV Infection
Nonimmune pregnant patients should attempt to limit exposure to the virus. For instance, because CMV infection is common among children attending day care centers, pregnant patients should always wash their hands thoroughly after exposure to urine and oral or respiratory secretions from children.
Pasteurization of donated human milk can decrease CMV transmission to severely immunocompromised neonates, who are at increased risk of severe postnatal CMV infection.
Transfusion-associated perinatal CMV disease can be avoided by giving preterm neonates blood products from CMV-seronegative donors or leukoreduced products.
Vaccines to prevent congenital CMV infection are in development. Maternal antiviral therapy with acyclovir or valacyclovir to prevent fetal transmission is being investigated (1).
CMV hyperimmune globulin given to pregnant patients with primary CMV infection did not show a reduction in congenital infection in a randomized, controlled trial (2).
Prevention references
1. Hughes BL, Clifton RG, Rouse DJ, et al: A trial of hyperimmune globulin to prevent congenital cytomegalovirus infection. N Engl J Med 385(5):436–444, 2021. doi: 10.1056/NEJMoa1913569
2. Revello MG, Lazzarotto T, Guerra B, et al: A randomized trial of hyperimmune globulin to prevent congenital cytomegalovirus. N Engl J Med 370(14):1316–1326, 2014. doi: 10.1056/NEJMoa1310214
Key Points
Cytomegalovirus (CMV) is the most common congenital viral infection and may be asymptomatic or symptomatic.
Multiple organs can be affected, and risk of preterm birth increases.
Distinguish symptomatic congenital CMV infection from other congenital infections (eg, toxoplasmosis, rubella, lymphocytic choriomeningitis, syphilis) using polymerase chain reaction (PCR) testing or viral culture.
Parenteral ganciclovir or oral valganciclovir may prevent hearing deterioration and improve neurodevelopmental outcomes in infants with symptomatic infection.
Drug Information for the Topic





