



Personality disorders in general are pervasive, enduring patterns of thinking, perceiving, reacting, and relating that cause significant distress or functional impairment. Personality disorders vary significantly in their manifestations, but all are believed to be caused by a combination of genetic and environmental factors. Many gradually become less severe with age, but certain traits may persist to some degree after the acute symptoms that prompted the diagnosis of a disorder abate. Diagnosis is based on clinical criteria. Treatment is with psychosocial therapies and sometimes with medications.
Personality traits represent patterns of thinking, perceiving, reacting, and relating that are relatively stable over time.
Personality disorders exist when these traits become so pronounced, rigid, and maladaptive that they impair work and/or interpersonal functioning. These social maladaptations can cause significant distress in people with personality disorders and in those around them. For people with personality disorders (unlike many others who seek counseling), the distress caused by the consequences of their socially maladaptive behaviors is usually the reason they seek treatment, rather than any discomfort with their own thoughts and feelings. Thus, clinicians must initially help patients see that their personality traits are the root of the problem.
Personality disorders usually start to become evident during late adolescence or early adulthood, although sometimes signs are apparent earlier (during childhood). Traits and symptoms vary considerably in how long they persist; many resolve with time.
The Diagnostic and Statistical Manual of Mental Disorders, 5th ed, Text Revision (DSM-5-TR) lists 10 types of personality disorders, although most patients who meet criteria for one type also meet criteria for one or more others. Some types (eg, antisocial, borderline) tend to lessen or resolve as people age; others (eg, obsessive-compulsive, schizotypal) are less likely to do so.
About 9% of the general population (1) and up to half of psychiatric patients in hospital units and clinics have a personality disorder (2). Overall, there are no clear distinctions in terms of sex, socioeconomic class, and race. However, for antisocial personality disorder, males outnumber females 3:1 (3). In borderline personality disorder, females outnumber males 3:1 (but only in clinical settings, not in the general population) (4).
For most personality disorders, levels of heritability are about 50%, which is similar to or higher than that of many other major psychiatric disorders. This degree of heritability argues against the common assumption that personality disorders are character flaws primarily shaped by an adverse environment.
The direct health care costs and indirect costs of lost productivity associated with personality disorders, particularly borderline and obsessive-compulsive personality disorder, are significantly greater than similar costs associated with major depressive disorder or generalized anxiety disorder.
Types of Personality Disorders
DSM-5-TR groups the 10 types of personality disorders into 3 clusters (A, B, and C), based on similar characteristics. However, the clinical usefulness of these clusters has not been established.
Cluster A is characterized by appearing odd or eccentric. It includes the following personality disorders with their distinguishing features:
Paranoid: Mistrust and suspicion
Schizoid: Disinterest in others
Schizotypal: Eccentric ideas and behavior

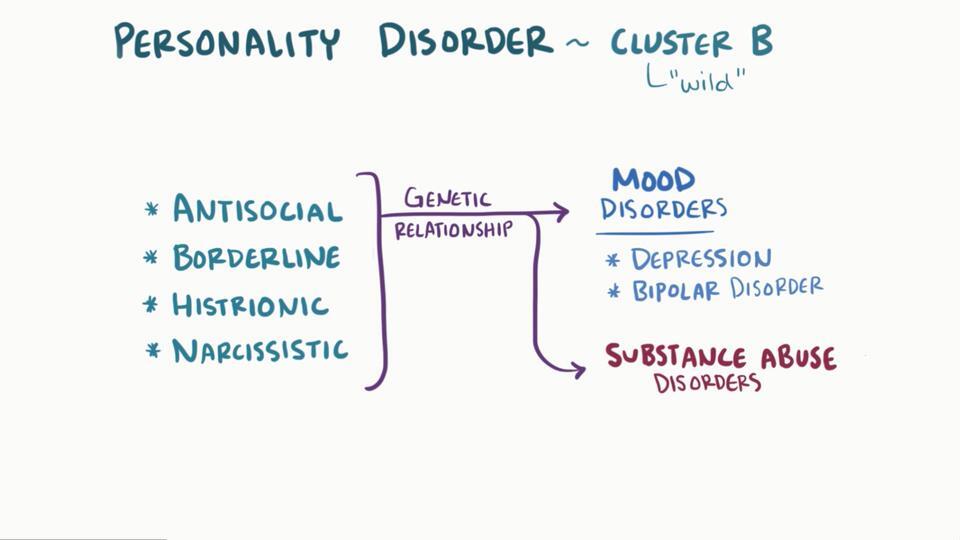
Cluster B is characterized by appearing dramatic, emotional, or erratic. It includes the following personality disorders with their distinguishing features:
Antisocial: Social irresponsibility, disregard for others, deceitfulness, and manipulation of others for personal gain
Borderline: Inner emptiness, unstable relationships, and emotional dysregulation
Histrionic: Attention seeking and excessive emotionality
Narcissistic: Self-grandiosity, need for admiration, and lack of empathy
Cluster C is characterized by appearing anxious or fearful. It includes the following personality disorders with their distinguishing features:
Avoidant: Avoidance of interpersonal contact due to rejection sensitivity
Dependent: Submissiveness and a need to be taken care of
Obsessive-compulsive: Perfectionism, rigidity, and obstinacy
General references
1. Lenzenweger MF, Lane MC, Loranger AW, et al: DSM-IV personality disorders in the National Comorbidity Survey Replication. Biol Psychiatry 62(6):553-564, 2007. doi: 10.1016/j.biopsych.2006.09.019
2. Zimmerman M, Chelminski I, Young D: The frequency of personality disorders in psychiatric patients. Psychiatr Clin North Am 31(3):405-220, 2008 vi. doi: 10.1016/j.psc.2008.03.015
3. Alegria AA, Blanco C, Petry NM, et al: Sex differences in antisocial personality disorder: Results from the National Epidemiological Survey on Alcohol and Related Conditions. Personal Disord 4(3):214-222, 2013. doi: 10.1037/a0031681
4. Sansone RA, Sansone LA: Gender patterns in borderline personality disorder. Innov Clin Neurosci 8(5):16-20, 2011. PMID: 21686143
Symptoms and Signs of Personality Disorders
According to DSM-5-TR, personality disorders are primarily problems with
Self-identity
Interpersonal functioning
Self-identity problems may manifest as an unstable self-image (eg, people fluctuate between seeing themselves as kind or cruel) or as inconsistencies in values, goals, and appearance (eg, people are deeply religious while in church but profane and disrespectful elsewhere).
Interpersonal functioning problems typically manifest as failing to develop or sustain close relationships and/or being insensitive to others (eg, unable to empathize).
People with personality disorders often seem inconsistent, confusing, and frustrating to people around them (including clinicians). These people may have difficulty knowing the boundaries between themselves and others. Their self-esteem may be inappropriately high or low. They may have inconsistent, detached, overemotional, abusive, or irresponsible styles of parenting, which can lead to physical and mental problems in their spouse and/or children.
People with personality disorders often lack insight regarding the impact of their behavior on interpersonal relationships.
Diagnosis of Personality Disorders
Diagnostic and Statistical Manual of Mental Disorders, 5th ed, Text Revision (DSM-5-TR) criteria
Personality disorders are underdiagnosed. When people with personality disorders seek treatment, their chief complaints are often of depression or anxiety rather than of the manifestations of their personality disorder. Once clinicians suspect a personality disorder, they evaluate cognitive, affective, interpersonal, and behavioral tendencies using specific diagnostic criteria. More sophisticated and empirically rigorous diagnostic tools are available for more specialized and academic clinicians.
Diagnosis of a personality disorder requires a persistent, inflexible, pervasive pattern of maladaptive traits involving ≥ 2 of the following (1) :
Cognition (ie, ways of perceiving and interpreting self, others, and events)
Affectivity (ie, range, intensity, lability, and appropriateness of emotional response)
Interpersonal functioning
Impulse control
The persistent pattern of maladaptive traits must cause significant distress or impaired functioning in social, occupational, and other important areas
The pattern is stable and has an early onset (traced back to at least adolescence or early adulthood)
Also, other possible causes of the symptoms (eg, other mental health disorders, substance use, head trauma) must be excluded.
For a personality disorder to be diagnosed in patients < 18 years, the pattern must have been present for ≥ 1 year, except for antisocial personality disorder, which cannot be diagnosed in patients < 18 years.
Because many patients with a personality disorder lack insight into their condition, clinicians may need to obtain history from other clinicians who have treated these patients previously, family members, friends, or others who have contact with them.
Diagnosis reference
1. American Psychiatric Association: Diagnostic and Statistical Manual of Mental Disorders, 5th ed, Text Revision (DSM-5-TR). Washington, DC, American Psychiatric Association, 2022, pp. 733-737.
Treatment of Personality Disorders
Psychotherapy
Sometimes medications for specific symptoms or coexisting psychiatric disorders
The gold standard of treatment for personality disorders is psychotherapy. Both individual and group psychotherapy are effective for many of these disorders if the patient is seeking treatment and is motivated to change.
Typically, personality disorders are not very responsive to medications, although some medications can effectively target specific symptoms (eg, depression, anxiety).
Disorders that often coexist with personality disorders (eg, depressive disorders, anxiety, substance-related disorders, somatic symptom disorders, and eating disorders) can make treatment challenging, lengthening time to remission, increasing risk of relapse, and decreasing response to otherwise effective treatment. For treatments typically used for each disorder, see table .
Treatment of Personality Disorders
Diagnosis | Psychotherapy | Medications |
|---|---|---|
Contingency management | Antidepressants (SSRIs) Mood stabilizers (lithium, valproate) | |
Psychodynamic psychotherapy Cognitive-behavioral therapy | Antidepressants (MAOIs, SSRIs) | |
General psychiatric management and other structured clinical management approaches Supportive psychotherapy Dialectical behavioral therapy Transference-focused psychotherapy Systems training for emotional predictability and problem solving | Mood stabilizers (lamotrigine, topiramate) for mood symptoms, impulsivity, and anxiety Atypical (2nd-generation) antipsychotics for transient psychotic symptoms, mood regulation, and anger problems Antidepressants (not harmful but limited efficacy) Avoidance of benzodiazepines and stimulants | |
Psychodynamic psychotherapy Cognitive-behavioral therapy | Antidepressants (MAOIs, SSRIs) | |
Psychodynamic psychotherapy | — | |
Psychodynamic psychotherapy | — | |
Psychodynamic psychotherapy | Antidepressants (SSRIs) | |
Cognitive-behavioral therapy | Antidepressants | |
Supportive psychotherapy Social skills training | — | |
Supportive psychotherapy Social skills training Cognitive-behavioral therapy for anxiety management | Atypical antipsychotics | |
* There is controversy about whether antisocial personality disorder is treatable. | ||
MAOIs = monoamine oxidase inhibitors; SSRIs = selective serotonin reuptake inhibitors. | ||
General principles for treatment
In general, treatment of personality disorders aims to
Reduce subjective distress
Enable patients to understand that their problems are internal to themselves
Decrease significantly maladaptive and socially undesirable behaviors
Modify problematic personality traits
Reducing subjective distress (eg, anxiety, depression) is the first goal. These symptoms often respond to increased psychosocial support, which often includes moving the patient out of highly stressful situations or relationships. Pharmacotherapy may also help relieve stress. Reduced stress makes treating the underlying personality disorder easier.
An effort to enable patients to recognize that their problems are internal should be made early. Patients need to understand that their problems with work or relationships are caused by their maladaptive ways of relating to the world (eg, to tasks, to authority, or in intimate relationships). Achieving such understanding requires a substantial amount of time, patience, and commitment on the part of a clinician. Clinicians also need a basic understanding of the patient’s areas of emotional sensitivity and usual ways of coping. Family members and friends can help identify problems of which patients and clinicians would otherwise be unaware.
Maladaptive and undesirable behaviors (eg, recklessness, social isolation, lack of assertiveness, temper outbursts) should be dealt with quickly to minimize ongoing damage to jobs and relationships. Behavioral change is most important for patients with the following personality disorders:
Behavior can typically be improved within months by group therapy and behavior modification; limits on behavior must often be established and enforced. Sometimes patients are treated in a day hospital or residential setting. Self-help groups or family therapy can also help change socially undesirable behaviors. Because family members and friends can act in ways that either reinforce or diminish the patient’s maladaptive behavior or thoughts, their involvement is helpful; with coaching, they can be allies in treatment.
Modifying maladaptive personality traits (eg, dependency, distrust, arrogance, manipulativeness) typically takes > 1 year. The cornerstone for effecting such change is individual psychotherapy.
During therapy, clinicians try to identify interpersonal problems as they occur in the patient's life. Clinicians then help patients understand how these problems are related to their personality traits and provide skills training to develop new, better ways of interacting. Typically, clinicians must repeatedly point out the undesirable behaviors and their consequences before patients become aware of them. This strategy can help patients change their maladaptive behaviors and mistaken beliefs. Although clinicians should act with sensitivity, they should be aware that kindness and sensible advice by themselves do not change personality disorders.
Key Points
Personality disorders involve rigid, maladaptive personality traits that are marked enough to cause significant distress or to impair work and/or interpersonal functioning.
Treatments become effective only after patients see that their problems are within themselves, not just externally caused.
Psychosocial therapy is the mainstay of treatment.
Medications help control specific symptoms only in selected cases—eg, to control significant anxiety, angry outbursts, and depression.
Personality disorders are slow to change, and may gradually become less severe over time.





