



Needle thoracostomy, also called needle decompression, is insertion of a needle into the pleural space to decompress a tension pneumothorax.
Needle thoracostomy is an emergency, potentially life-saving, procedure that can be done if tube thoracostomy cannot be done quickly enough.
Indications for Needle Thoracostomy
Tension pneumothorax that must be decompressed before tube thoracostomy can be done, usually in patients with hemodynamic instability due to compression of major blood vessels (1).
Contraindications to Needle Thoracostomy
None
There are no contraindications because this procedure is only done because of an immediate threat to life (usually hemodynamic compromise) which supersedes other considerations such as bleeding diatheses or anatomical chest-wall abnormalities.
Complications of Needle Thoracostomy
Pulmonary or diaphragmatic laceration
Intercostal neuralgia due to injury of the neurovascular bundle below a rib
Bleeding
Infection
Pneumothorax that is iatrogenic (if the procedure was done because of falsely suspected pneumothorax)
Rarely, perforation of other structures in the chest or abdomen
Equipment for Needle Thoracostomy
A 14- or 16-gauge needle (an over-the-needle catheter is best); 8-cm needles are more successful than 5-cm needles (2) but increase the risk of injury to underlying structures
Sterile gown, mask, gloves
Antiseptic solution for cleansing the area such as 2% chlorhexidine solution or povidone-iodine
Skin marking pen (optional)
Additional Considerations for Needle Thoracostomy
The urgency of the procedure is determined by the patient’s condition. Hypotension suggests a more advanced tension pneumothorax requiring more urgent treatment.
Relevant Anatomy for Needle Thoracostomy
Neurovascular bundles are located at the lower edge of each rib. Therefore, the needle must be placed over the upper edge of the rib to avoid damage to the neurovascular bundle.

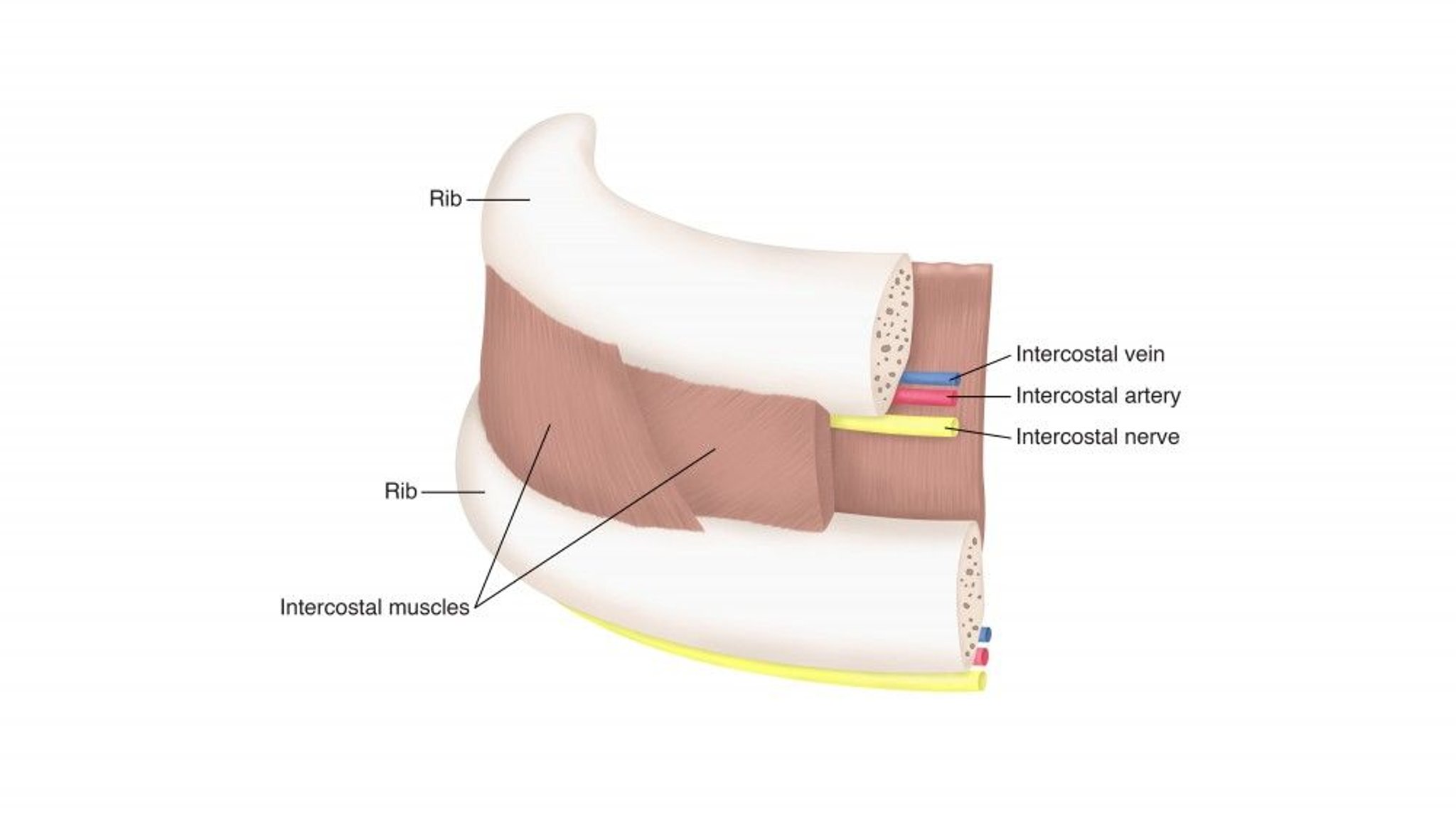
The neurovascular bundle located at the lower edge of the rib includes the intercostal vein, artery, and nerve.
Positioning for Needle Thoracostomy
Patient should be supine (lying on the back).
Step-by-Step Description of Needle Thoracostomy
Select the insertion site: The preferred insertion site historically has been the second intercostal space in the mid-clavicular line in the affected hemithorax due to ease of access. However, this site has a high failure rate with thicker chest walls. Specific alternative sites such as the fourth or fifth intercostal space along the anterior axillary line have been suggested due to lower failure rates (3).
If time permits, prepare the area at and around the insertion site using an antiseptic solution such as chlorhexidine or povidone-iodine.
There is rarely time to provide local anesthesia, but if there is, inject 1% lidocaine into the skin, subcutaneous tissue, rib periosteum (of the rib below the insertion site), and the parietal pleura. Inject a large amount of local anesthetic around the highly pain-sensitive periosteum and parietal pleura. Aspirate with the syringe before injecting lidocaine to assess for blood; this step is needed to avoid injection into a blood vessel. Proper location is confirmed by return of air in the anesthetic syringe when entering the pleural space.
Insert the thoracostomy needle, piercing the skin over the rib below the target interspace, then directing the needle toward the head over the rib until the pleura is punctured (usually indicated by a pop and/or sudden decrease in resistance).
After doing a needle thoracostomy, make preparations for a tube thoracostomy as soon as possible.


Aftercare for Needle Thoracostomy
Chest radiograph should be done to confirm expansion of the lung and proper placement of the chest tube.
Warnings and Common Errors for Needle Thoracostomy
Depending on the thickness of the chest wall, a longer needle or alternate site may be needed.
Tips and Tricks for Needle Thoracostomy
References
1. Lyng JW, Ward C, Angelidis M, et al: Prehospital Trauma Compendium: Traumatic Pneumothorax Care: Position Statement and Resource Document of NAEMSP. Prehosp Emerg Care Published online December 4, 2024. doi:10.1080/10903127.2024.2416978
2. Aho JM, Thiels CA, El Khatib MM, et al: Needle thoracostomy: Clinical effectiveness is improved using a longer angiocatheter. J Trauma Acute Care Surg 80(2):272–277, 2016. doi: 10.1097/TA.0000000000000889
3. Laan DV, Vu TD, Thiels CA, et al: Chest wall thickness and decompression failure: A systematic review and meta-analysis comparing anatomic locations in needle thoracostomy. Injury 47(4):797–804, 2016. doi:10.1016/j.injury.2015.11.045
4. Clemency BM, Tanski CT, Rosenberg M, et al: Sufficient catheter length for pneumothorax needle decompression: A meta-analysis. Prehosp Disaster Med 30(3):249–253, 2015. doi: 10.1017/S1049023X15004653
5. Beckett A, Savage E, Pannell D, et al: Needle decompression for tension pneumothorax in Tactical Combat Casualty Care: Do catheters placed in the midaxillary line kink more often than those in the midclavicular line? J Trauma 2011 71(5 Suppl 1):S408–S412, 2011. doi: 10.1097/TA.0b013e318232e558
Drug Information for the Topic





