

An intracranial epidural abscess is a pocket of pus that develops between the skull and the top layer of tissues covering the brain (dura mater). A subdural empyema is a pocket of pus that develops between the dura mater and the middle layer of the tissues covering the brain (arachnoid mater).
(See also Overview of Brain Infections.)
Intracranial epidural abscesses and subdural empyemas may result from a sinus or an ear infection or from conditions that allow bacteria to enter the skull, such as a head injury or head surgery.
Fever, headache, sleepiness, vomiting, seizures, a stiff neck, and other signs of brain dysfunction may develop over several days.
Without treatment, symptoms progress rapidly, leading to coma and death.
To diagnose these disorders, doctors do magnetic resonance imaging or computed tomography with a contrast agent.
Treatment includes surgical drainage, antibiotics, and sometimes drugs to prevent seizures or to reduce pressure within the skull.
Intracranial epidural abscesses and subdural empyemas develop outside the brain itself but within the skull:
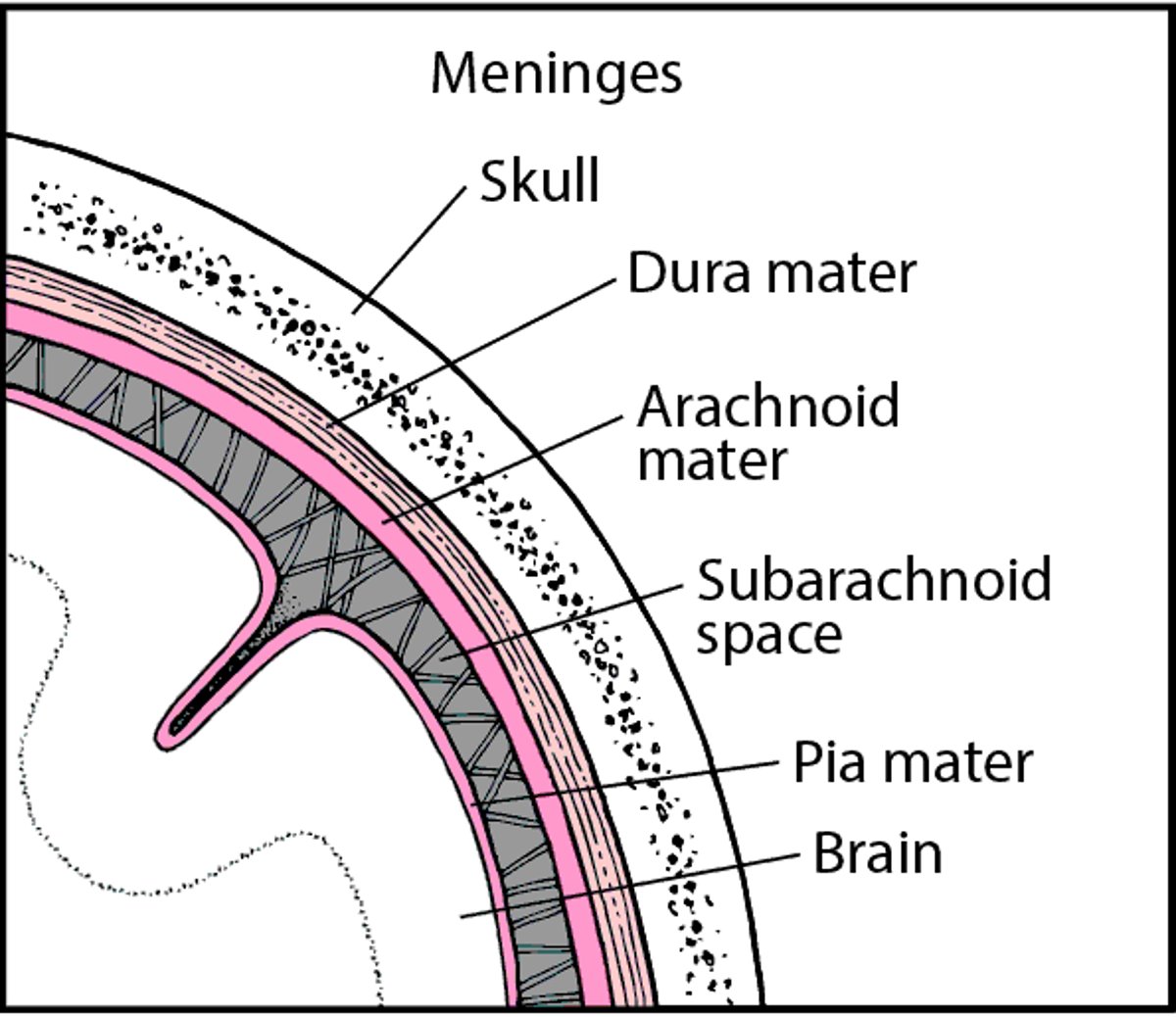
Intracranial epidural abscess: Between the dura mater (the outer layer of tissue covering the brain) and the skull
Subdural empyema: Between the arachnoid mater (the middle layer of tissue covering the brain) and the dura mater
Tissues Covering the Brain
Within the skull, the brain is covered by 3 layers of tissue called the meninges. |

Causes
Epidural abscesses and subdural empyemas may result from
A severe ear infection (such as chronic otitis media)
A head injury that allows bacteria to enter the skull
Surgery on the head that allows bacteria to enter the skull
Rarely, a blood infection
The same kinds of bacteria that cause brain abscesses (such as Staphylococcus aureus and Bacteroides fragilis) can cause epidural abscesses and subdural empyemas.
In children younger than 5 years, the cause is usually bacterial meningitis. Because meningitis is now uncommon in children, epidural abscesses and subdural empyemas are also uncommon in children.
Symptoms
Like a brain abscess, an epidural abscess or a subdural empyema can cause fever, headache, sleepiness, vomiting, seizures, a stiff neck, and other signs of brain dysfunction.
The symptoms can evolve over several days. Meningitis or a brain abscess may develop. Or a blood clot may form in the large veins (venous sinuses) that carry blood from the brain.
Without treatment, symptoms progress rapidly, leading to coma and death, particularly in people with a subdural empyema.
Diagnosis
Magnetic resonance imaging or computed tomography
To diagnose an epidural abscess or a subdural empyema, doctors use magnetic resonance imaging (MRI) done after gadolinium is injected intravenously. Gadolinium (an MRI contrast agent) makes abscesses and empyemas easier to see on MRI scans. If MRI is not available, computed tomography (CT) is done after a radiopaque contrast agent (which makes abscesses and empyemas easier to see on CT scans) is injected.
Samples of blood and tissue are sent to a laboratory so that any bacteria present can be grown (cultured) identified.
A spinal tap (lumbar puncture) is of little help and may be dangerous. If a large abscess, empyema, or other mass is present in the skull, removing spinal fluid during a spinal tap can cause the brain to shift down and be forced through a small natural opening in the tissue that divides the brain into compartments (called brain herniation). The resulting damage can be fatal.
Treatment
Drainage of the pus
Antibiotics and sometimes other medications
In infants, a needle can sometimes be inserted directly into the abscess or empyema through a fontanelle (a soft spot between the skull bones) to drain the pus, relieve pressure, and help doctors make the diagnosis.
Epidural abscesses and subdural empyemas must be drained surgically. If the infection occurred because of an abnormality in the sinuses or middle ear, the surgeon may need to repair the abnormality at the same time.
Antibiotics (such as cefotaxime or ceftriaxone, metronidazole, and vancomycin) are given intravenously.Antibiotics (such as cefotaxime or ceftriaxone, metronidazole, and vancomycin) are given intravenously.
Antiseizure medications to control seizures and measures to reduce pressure within the skull may be needed. These measures include the following:
Use of diuretics, which reduce the amount of fluid in the body
Corticosteroids, which reduce inflammation and swelling
Drug Information for the Topic





