

Trigeminal neuralgia is severe facial pain due to malfunction of the fifth cranial nerve (trigeminal nerve). This nerve carries sensory information from the face to the brain and controls the muscles involved in chewing.
The cause is usually an abnormally positioned artery that compresses the trigeminal nerve.
People have repeated short, lightning-like bursts of excruciating stabbing pain in the lower part of the face.
Doctors base the diagnosis on the characteristic pain.
Certain antiseizure medications, certain antidepressants, or baclofen, may relieve the pain, but surgery is sometimes needed.Certain antiseizure medications, certain antidepressants, or baclofen, may relieve the pain, but surgery is sometimes needed.
Trigeminal neuralgia usually affects mainly adults, especially older adults. It is more common among women.
A common cause of trigeminal neuralgia is
An abnormally positioned artery that compresses the trigeminal nerve near where it exits the brain
Occasionally in younger people, trigeminal neuralgia results from nerve damage due to multiple sclerosis. Rarely, trigeminal neuralgia results from damage due to compression by a tumor, an abnormal connection between arteries and veins (arteriovenous malformation), or a bulge (aneurysm) in an artery supplying the brain.
Symptoms of Trigeminal Neuralgia
Pain due to trigeminal neuralgia can occur spontaneously but is often triggered by touching a particular spot (called a trigger point) on the face, lips, or tongue or by an action such as brushing the teeth or chewing. Repeated short, lightning-like bursts of excruciating stabbing pain can be felt in any part of the lower portion of the face but are most often felt in the cheek next to the nose or in the jaw.
Usually, only one side of the face is affected. The pain usually lasts seconds but may last up to 2 minutes. Recurring as often as 100 times a day, the pain can be incapacitating. Because the pain is intense, people tend to wince, and thus the disorder is sometimes called a tic. The disorder commonly resolves on its own, but bouts of the disorder often recur after a long pain-free interval.
Diagnosis of Trigeminal Neuralgia
A doctor's evaluation
Magnetic resonance imaging
Although no specific test exists for identifying trigeminal neuralgia, its characteristic pain usually makes it easy for doctors to diagnose. MRI of the brain is done to determine whether an artery is crossing the nerve. This information may guide future therapy. Brain MRI can also determine whether a tumor is compressing the nerve. However, doctors must distinguish trigeminal neuralgia from other possible causes of facial pain, such as disorders of the jaw, teeth, or sinuses.
Treatment of Trigeminal Neuralgia
Antiseizure or other medications
Sometimes surgery
Because the bouts of pain are brief and recurrent, typical analgesics are not usually helpful, but other medications, especially certain antiseizure medications, taken by mouth, may help. (Antiseizure medications stabilize nerve cell membranes.) The antiseizure medication carbamazepine is usually tried first. Oxcarbazepine, lamotrigine, gabapentin, or phenytoin, which are also antiseizure medications, may be prescribed if carbamazepine is ineffective or has intolerable side effects. , taken by mouth, may help. (Antiseizure medications stabilize nerve cell membranes.) The antiseizure medication carbamazepine is usually tried first. Oxcarbazepine, lamotrigine, gabapentin, or phenytoin, which are also antiseizure medications, may be prescribed if carbamazepine is ineffective or has intolerable side effects.
Baclofen (a medication used to reduce muscle spasms) or amitriptyline (a Baclofen (a medication used to reduce muscle spasms) or amitriptyline (atricyclic antidepressant) may be used instead. If amitriptyline has intolerable side effects, another tricyclic antidepressant may be tried.) may be used instead. If amitriptyline has intolerable side effects, another tricyclic antidepressant may be tried.
Injecting botulinum toxin (used to paralyze muscles or to treat wrinkles) near the area where pain is experienced may help some people. This treatment is used as an alternative to surgery in people whose pain does not respond well to medication.
If bouts of pain are frequent and severe, doctors may use a nerve block to temporarily relieve the pain until the medication given by mouth takes effect. An anesthetic is injected into the nerve to temporarily block its function.
If the pain continues to be severe despite medication, surgery may be done. If the cause is an abnormally positioned artery, a surgeon separates the artery from the nerve and places a small sponge between them. This procedure (called vascular decompression) usually relieves the pain for many years. If the cause is a tumor, the tumor can be surgically removed.
If people have pain unrelieved by medications and surgery seems too risky, a nerve block can be done to determine whether other procedures would help. If the injection of the anesthetic into the nerve relieves the pain, disrupting the nerve may relieve the pain, sometimes permanently. Disruptions may involve
Cutting the nerve surgically
Cutting the nerve with a radiofrequency probe (using heat) or a gamma knife
Compressing the nerve with a balloon
Destroying the nerve by injecting an agent such as glycerol into it
However, surgery that relieves pain often results in facial numbness. Also, pain often recurs. As a result, people may require many procedures. Having many procedures may increase the risk of developing severe pain that is difficult to treat.
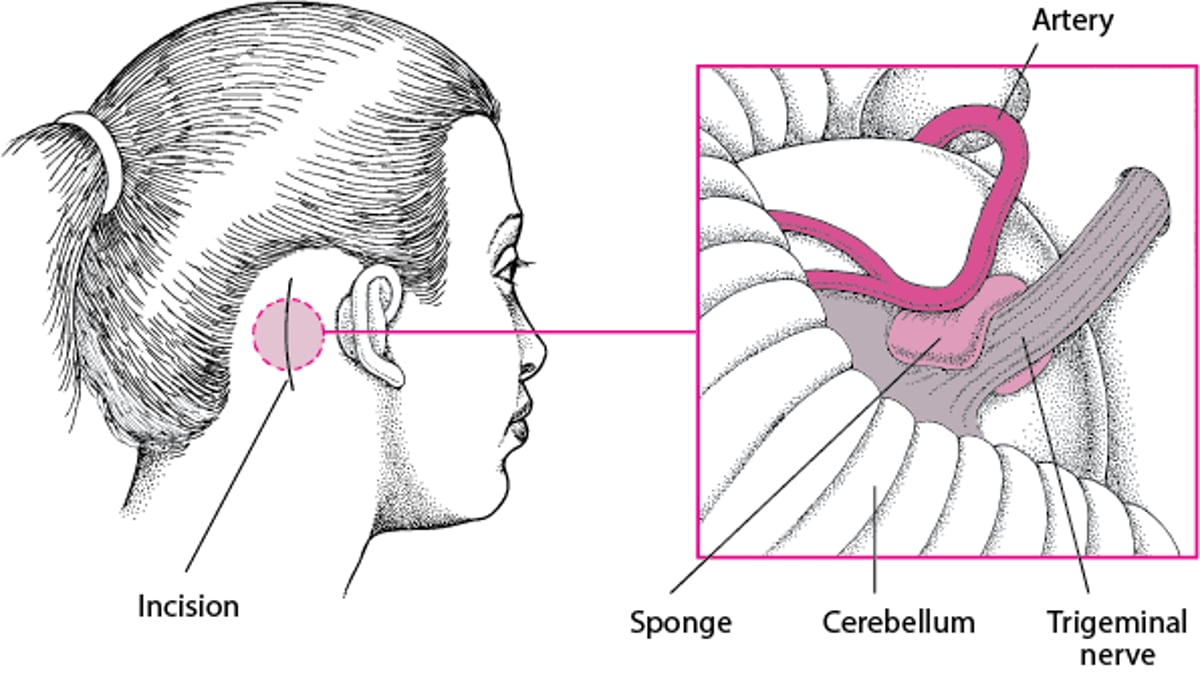
Taking the Pressure Off a Nerve
When pain results from an abnormally positioned artery pressing on a cranial nerve, the pain can be relieved by a surgical procedure called vascular decompression. This procedure may be done to treat trigeminal neuralgia, hemifacial spasms, or glossopharyngeal neuralgia. If the trigeminal nerve is compressed, an area on the back of the head is shaved, and an incision is made. The surgeon cuts a small hole in the skull and lifts the edge of the brain to expose the nerve. Then the surgeon separates the artery from the nerve and places a small sponge between them. A general anesthetic is required, but the risk of side effects from the procedure is small. Side effects include facial numbness, facial weakness, double vision, infection, bleeding, alterations in hearing and balance, and paralysis. Usually, this procedure relieves the pain, but in about 15% of people, pain recurs. |

Drug Information for the Topic





