

Esophageal spasm is a disorder of the rhythmic waves of muscular contractions (peristalsis) of the esophagus.
The cause of this disorder is not known.
Symptoms include chest pain and difficulty swallowing.
The diagnosis is based on the results of barium swallow x-rays and manometry.
Treatments include calcium channel blockers or other medications, injections of botulinum toxin, and sometimes surgery or endoscopy.
The esophagus is the hollow tube that leads from the throat (pharynx) to the stomach. (See also Overview of the Esophagus.)
In esophageal spasm, the normal propulsive contractions that move food through the esophagus are replaced periodically by nonpropulsive contractions or excessive muscular contractions that do not move food through the esophagus.
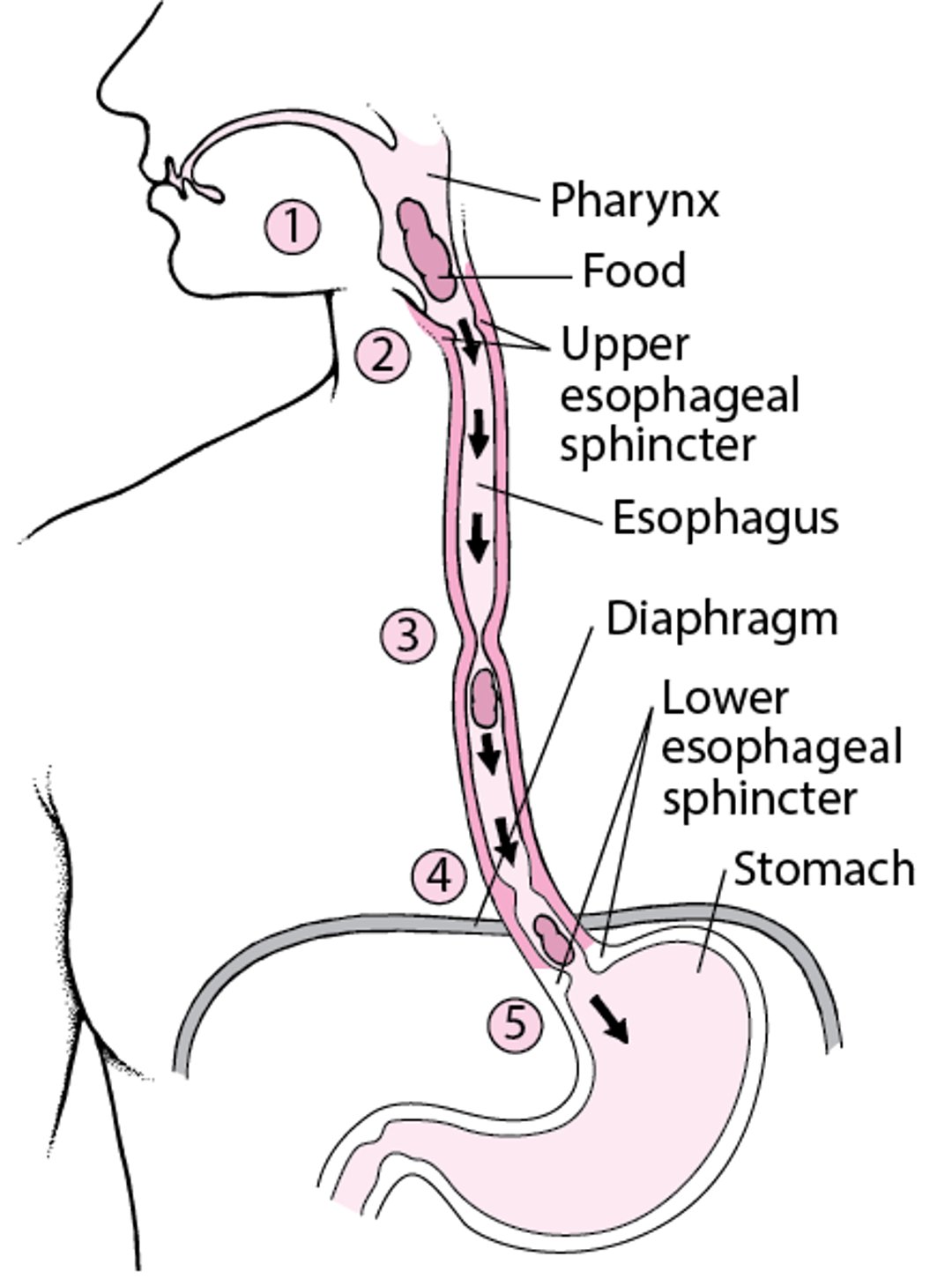
How the Esophagus Works
As a person swallows, food moves from the mouth to the throat, also called the pharynx (1). The upper esophageal sphincter opens (2) so that food can enter the esophagus, where waves of muscular contractions, called peristalsis, propel the food downward (3). The food then passes through the diaphragm (4) and lower esophageal sphincter (5) and moves into the stomach. |

The exact cause of esophageal spasm is not known but is suspected to be a nerve defect. People who take opioids are at increased risk of esophageal spasm.
Symptoms of Esophageal Spasm
Sometimes, esophageal spasm does not cause any symptoms.
When it does cause symptoms, muscle spasms throughout the esophagus typically are felt as chest pain under the breastbone coinciding with difficulty swallowing (dysphagia) liquids (especially those that are very hot or cold) and solids.
Esophageal spasm also may cause severe pain without swallowing difficulty. This pain, often described as a squeezing pain under the breastbone, may accompany exercise or exertion, making it difficult for a doctor to distinguish it from angina (chest pain stemming from heart disease).
Diagnosis of Esophageal Spasm
Tests to rule out heart disease
Barium swallow x-rays
Manometry
Because the chest pain of esophageal spasm is similar to that of angina (chest pain caused by heart disease), doctors do tests to rule out heart disease. Tests may include computed tomography (CT) scans of the coronary arteries, electrocardiography (ECG), exercise stress testing, or other tests.
To look for esophageal spasm itself, doctors may do a barium swallow. In this test, people are given barium in a liquid before x-rays are taken. The barium outlines the esophagus, making abnormalities easier to see. This test may show that the barium does not move normally down the esophagus and that some of the contractions of the esophageal wall are uncoordinated and do not move the barium.
Pressure measurements by manometry (a test in which a tube placed in the esophagus measures the pressure of contractions) provide the most sensitive and detailed analysis of the spasms.
Treatment of Esophageal Spasm
Calcium channel blockers
Stopping opioid use
Injections of botulinum toxin
Sometimes surgical or endoscopic myotomy
Esophageal spasm is often difficult to treat. Calcium channel blockers such as nifedipine may relieve the symptoms by relaxing the muscles of the esophagus. Tricyclic antidepressants are also used to relax muscles and may also be given. Esophageal spasm is often difficult to treat. Calcium channel blockers such as nifedipine may relieve the symptoms by relaxing the muscles of the esophagus. Tricyclic antidepressants are also used to relax muscles and may also be given.
Other medications such as nitroglycerin, long-acting nitrates, tricyclic antidepressants, and medications with Other medications such as nitroglycerin, long-acting nitrates, tricyclic antidepressants, and medications withanticholinergic effects (such as dicyclomine) are less successful. (such as dicyclomine) are less successful.
People who are taking opioids should stop taking them.
Rarely, a trial of botulinum toxin injections into the esophagus, lower esophageal sphincter, or both may be tried.
Some people have symptoms that are severe and difficult to treat with medications. If medications do not help, sometimes a surgeon may cut the muscle layer along the full length of the esophagus (myotomy). Alternatively, a gastroenterologist may cut this muscle layer during endoscopy.
Drug Information for the Topic





