

Familial adenomatous polyposis is an inherited disorder in which many (often 100 or more) precancerous polyps develop throughout the large intestine and rectum during childhood or adolescence.
A polyp is a growth of tissue that projects from the wall of a hollow space, such as the intestines (see also Polyps of the Colon and Rectum).
Familial adenomatous polyposis occurs in 1 in 8,000 to 14,000 people. The polyps are present in 50% of people by age 15 and in 95% of people by age 35. In nearly all untreated people, the polyps develop into cancer of the large intestine or rectum (colorectal cancer) before age 40.
Did You Know...
|
People with familial adenomatous polyposis also have an increased risk of developing cancer in the duodenum, pancreas, thyroid, brain, and liver. People with familial adenomatous polyposis can develop other complications (previously termed Gardner syndrome), particularly various types of noncancerous tumors. These noncancerous tumors develop elsewhere in the body (for example, on the skin, skull, or jaw).
Symptoms of Familial Adenomatous Polyposis
Symptoms of familial adenomatous polyposis are the same as with other colonic polyps (see symptoms of polyps of the colon and rectum).
Most people have no symptoms, but a few have rectal bleeding. Usually the bleeding is only in microscopic amounts.
Diagnosis of Familial Adenomatous Polyposis
Colonoscopy
Genetic testing
Testing for hepatoblastoma in children
Colonoscopy is done to make the diagnosis of familial adenomatous polyposis.
For people with familial adenomatous polyposis, doctors also recommend genetic testing. First-degree relatives (parents, siblings, or children) should also have genetic testing. If genetic testing is unavailable, relatives should be screened once a year with sigmoidoscopy (examination of the lower portion of the large intestine with a viewing tube) beginning at age 12. These screenings are done less frequently over time.

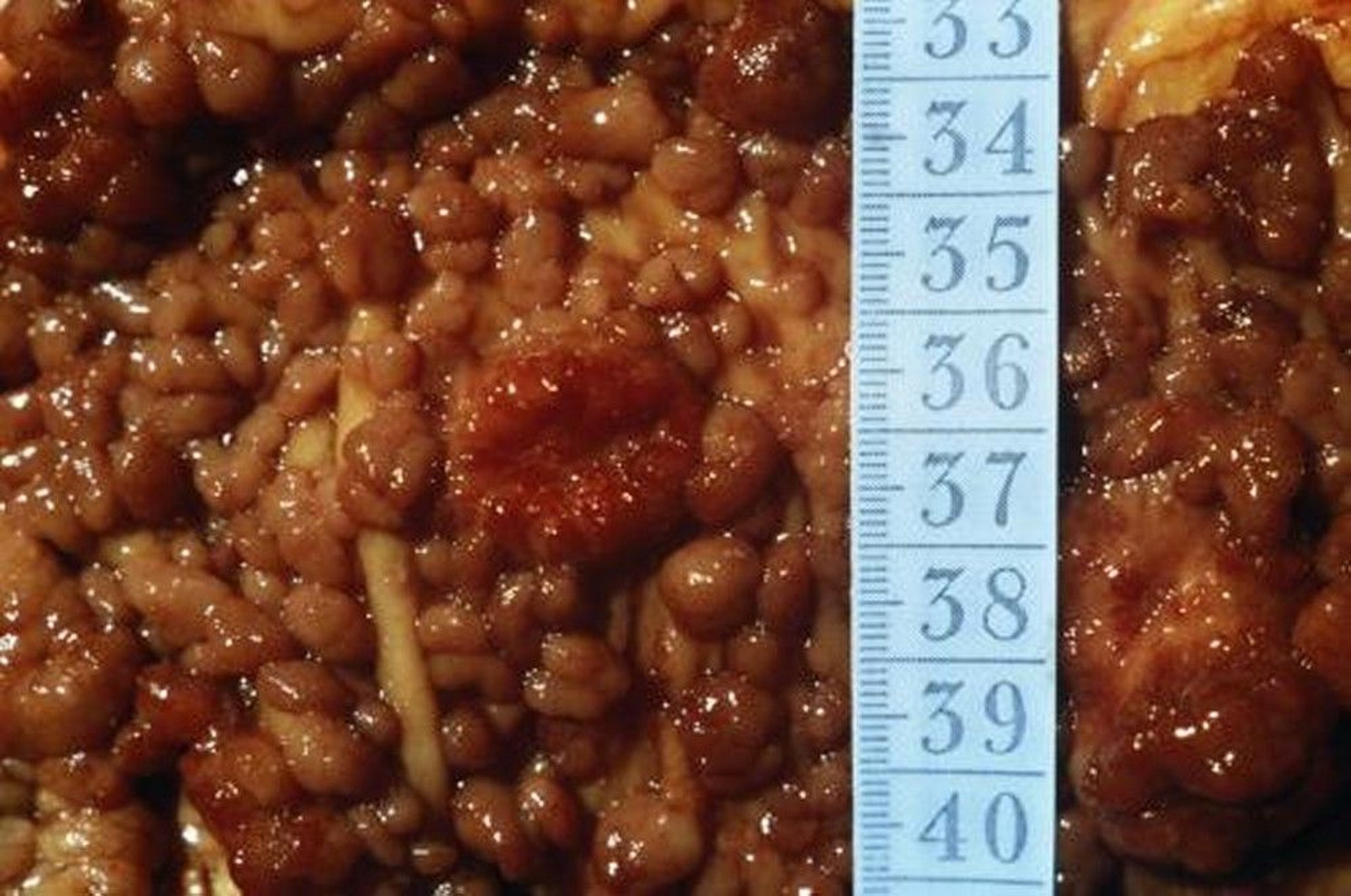
This photo shows numerous polyps in the colon.
CNRI/SCIENCE PHOTO LIBRARY
Children of people with familial adenomatous polyposis may be given blood and sometimes imaging tests to screen for a type of liver cancer (hepatoblastoma) from birth until 5 years of age.
Treatment of Familial Adenomatous Polyposis
Surgical removal of the colon and sometimes the rectum
Possibly nonsteroidal anti-inflammatory drugs (NSAIDs)
Because nearly all people with familial adenomatous polyposis develop cancer, doctors typically recommend surgery be done soon after the diagnosis is made. There are several procedures. Complete removal of the large intestine and rectum (called total colectomy or proctocolectomy) eliminates the risk of cancer. Because the person then has no rectum, the cut-off end of the small intestine is permanently attached to a surgical opening in the abdominal wall (ileostomy). Bodily wastes (stool) are eliminated through the ileostomy into a disposable bag.
As an alternative to ileostomy, sometimes doctors can remove the large intestine and only the lining of the rectum (polyps grow from the lining). Then, they can form the end of the small intestine into a pouch that is connected to the anus. The pouch functions somewhat like a rectum, eliminating the need for an ileostomy.
As another alternative to ileostomy, only the large intestine is removed and the rectum is joined to the small intestine. This procedure does not eliminate the possibility of rectal polyps developing, which could then turn into cancer. Thus the remaining part of the rectum must be inspected by sigmoidoscopy frequently, so that new polyps can be removed. If new polyps appear too rapidly, however, the rectum must also be removed and a pouch or ileostomy is needed.
After people have their entire rectum and large intestine removed, they should have an endoscopy of the stomach and upper section of the small intestine (duodenum) at regular intervals to look for cancer. Doctors may also recommend people have their thyroid screened every year.
Some NSAIDs are being studied for their ability to reverse the growth of polyps in people with familial adenomatous polyposis and in people with polyps or cancer of the large intestine. Their effects are temporary, however, and once these drugs are stopped, the polyps begin to grow again.





