

Corneal transplantation (keratoplasty) is a common and highly successful type of transplantation. A scarred, severely painful, perforated, misshapen, or cloudy cornea (the clear layer in front of the iris and pupil) can be replaced with a clear, healthy one.
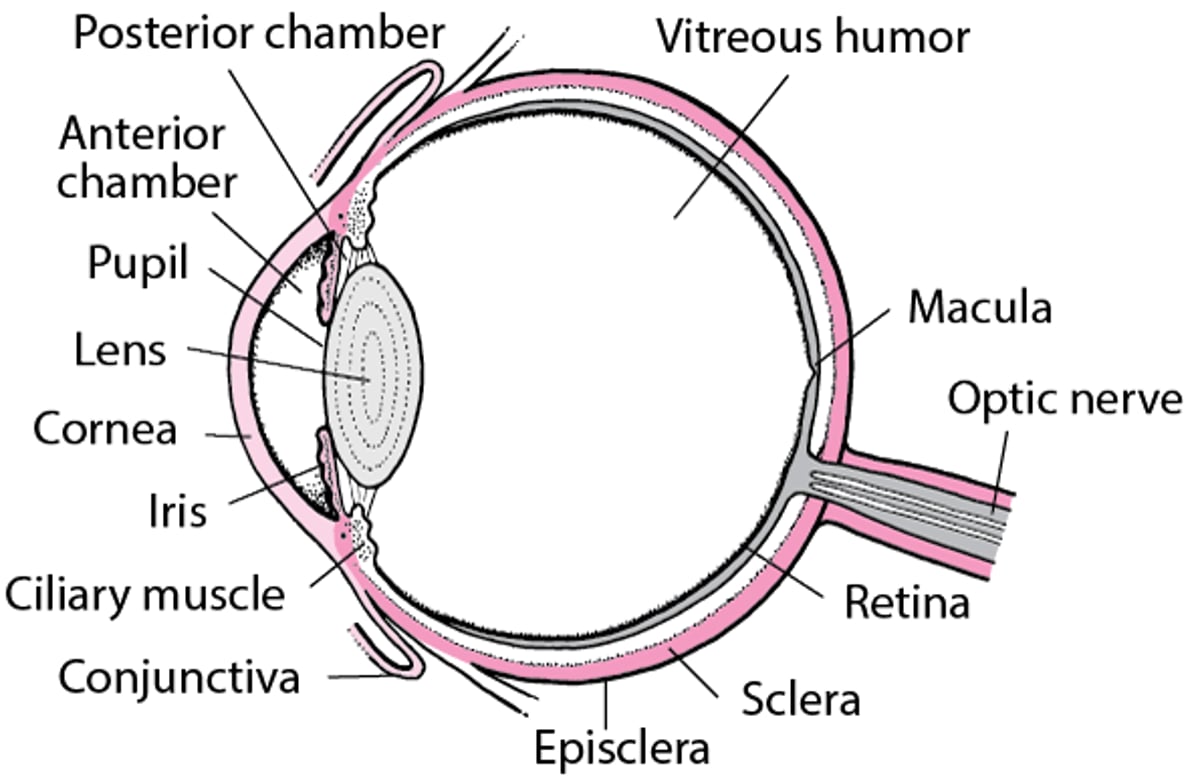
An Inside Look at the Eye

Donated corneas come from people who have recently died. Tissue matching is not routinely done because rejection is relatively rare and rejection reactions usually respond to treatment.
Transplants tend to be most successful when done for disorders such as bullous keratopathy, keratoconus, and certain corneal scars. They tend to be least successful when done because the cornea was damaged by a chemical or radiation.

Corneal Transplantation Procedures
There are 2 types of procedures:
Penetrating keratoplasty
Descemet stripping endothelial keratoplasty or Descemet membrane endothelial keratoplasty
For either procedure, doctors use a surgical microscope to do the procedure in about 1 to 2 hours. A general anesthetic (which puts a person to sleep) or a local anesthetic (which numbs the eye) and a medication given by vein that makes a person become very sleepy (called sedation) is used.
In penetrating keratoplasty, the donated cornea is cut to the right size, the whole damaged cornea is removed, and the whole donated cornea is sewn in place.
Some diseases of the cornea affect only the inner layers. For these diseases, doctors do a partial transplant in a procedure called Descemet stripping endothelial keratoplasty (DSEK) or Descemet membrane endothelial keratoplasty (DMEK). They remove and replace only the inner layers of the cornea instead of the whole cornea. The incision is smaller, fewer sutures are needed, healing is faster, and vision improves faster than when the whole cornea is replaced. However, the surgical technique is more difficult than in penetrating keratoplasty and may require a laser treatment before surgery and additional office surgery to get the best results.
Some diseases of the cornea affect only the outer and middle layers. For these, doctors can sometimes do a procedure called deep anterior lamellar keratoplasty (DALK), which replaces the middle and the outer layers of the cornea. This procedure takes more time than other corneal transplants and is more technically difficult. For people who have a particular form of inherited bullous keratopathy, a procedure called Descemet stripping only (DSO) can be done. In DSO, no tissue from another person is required.
In all types of corneal transplantation, the recipient usually goes home the same day. After transplantation, people must take antibiotic eye drops for several weeks and corticosteroid eye drops for several months. An eye shield, glasses, or sunglasses must be worn. Vision is not fully improved for about 18 months after penetrating keratoplasty and for 2 to 6 months after partial transplant.
Complications of Corneal Transplantation
Some corneal transplantation complications are
Rejection of the transplant
Infection
Incision problems
Failure of the transplant
Episodes of mild rejection are common and are easily and successfully treated with corticosteroid eye drops in most people. Severe, irreversible rejection (called graft failure) is rare. DMEK has the lowest rejection rates, and penetrating keratoplasty has the highest rejection rates of the different types of corneal transplantation. Rejection is not a risk with DSO because there is no foreign tissue to reject.
A transplanted cornea is usually not irreversibly rejected because a cornea does not have or need a blood supply. It receives oxygen and other nutrients from nearby tissues and fluid. The components of the immune system that initiate rejection in response to a foreign substance—certain white blood cells and antibodies—are carried in the bloodstream. Thus, these cells and antibodies do not reach the transplanted cornea, do not encounter the foreign tissue there, and do not initiate severe rejection. However, in rare cases where abnormal blood vessels have grown deeply and extensively into the person’s cornea, the transplanted cornea is severely rejected and fails at a higher rate.
Sometimes the transplant may fail and not work well (that is, it may become cloudy and not remain clear). Corneal transplants can be repeated multiple times.
People who have had several unsuccessful transplants may be given an artificial cornea (keratoprosthesis).
Corneal Limbal Stem Cell Transplantation
The eye, like other living tissues, depends on continual production of new cells to replace old ones. One place that this production occurs is where the cornea attaches to the conjunctiva (called the limbus). Certain kinds of injuries (for example, severe chemical burns or very severe and prolonged overwearing of contact lenses) damage these limbal stem cells so much that they can no longer produce enough new cells to keep the cornea covered. Infection and scarring can then affect the cornea. A corneal transplant does not replace the limbal stem cells and thus is of no benefit.
Stem cells can be transplanted from the limbus of a person's other eye, if it is healthy, or from a person who recently died, sometimes curing or relieving the problem. After stem cells from a deceased donor are transplanted, people are given medications that suppress the immune system so that their body does not reject the transplant.





