


Breast cancer rarely causes symptoms in its early stages, and early treatment is more likely to be successful; thus, screening is important. Screening is the hunt for a disorder before any symptoms occur. Breast cancer screening is recommended for all women in the United States, but major medical organization vary regarding the starting age and frequency of screening.
Screening for Breast Cancer
Screening for breast cancer may include
Yearly breast examination by a health care professional
Mammography
If women have an increased risk of breast cancer, magnetic resonance imaging (MRI)
Concerns about screening for breast cancer
It can be challenging to keep up with the latest recommendations for breast cancer screening, such as when to start mammograms. Also, medical organizations may change their recommendations over time, or different organizations may have different recommendations.
Some people think that more testing is better, but testing may also have disadvantages. For example, screening tests for breast cancer sometimes indicate a cancer is present when no cancer is present (called a false-positive result). When results of a breast screening test are positive, a breast biopsy is usually done. Having a false-positive result means having a biopsy that is not needed and being exposed to unnecessary anxiety, pain, and expense. Because of these potential issues, organizations recommend that some people do not need to have a screening test. These people include those who are younger or older than a certain age (see sidebar Breast Cancer: When to Start Screening Mammography?). Women should discuss current recommendations and their own risk and priorities with a health care professional and decide which type of screening, if any, is appropriate for them.
Mammography
Mammography is one of the most effective ways to detect breast cancer early. Mammography is designed to be sensitive enough to detect the possibility of cancer at an early stage, sometimes years before it can be felt. Because mammography is so sensitive, it may indicate cancer when none is present (a false-positive result). About 85 to 90% of abnormalities detected during screening (that is, in women with no symptoms or lumps) are not cancer. Typically, when the result is positive, more specific diagnostic procedures, usually a breast biopsy, are scheduled. Mammography may miss up to 15% of breast cancers. It is less accurate in women with dense breast tissue. Thus, these women may require additional tests, such as breast ultrasonography, 3-dimensional mammography (tomosynthesis), or magnetic resonance imaging (MRI).
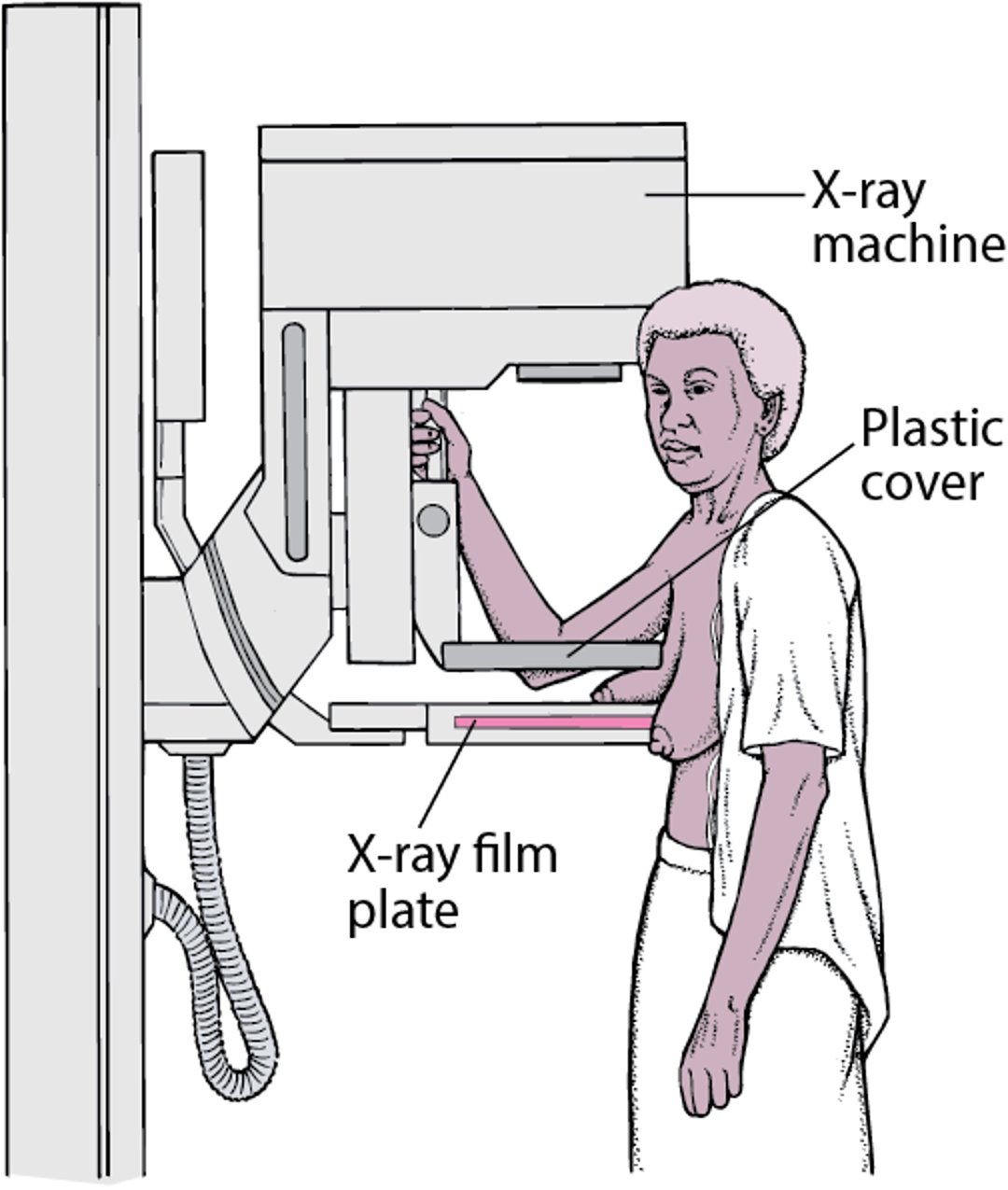
For mammography, x-rays are used to check for abnormal areas in the breast. A technician positions the woman’s breast on top of an x-ray plate. An adjustable plastic cover is lowered on top of the breast, firmly compressing the breast. Thus, the breast is flattened so that the maximum amount of tissue can be imaged and examined. X-rays are aimed downward through the breast, producing an image on the x-ray plate. Two x-rays are taken of each breast in this position. Then plates may be placed vertically on either side of the breast, and x-rays are aimed from the side. This position produces a side view of the breast.
Mammography: Screening for Breast Cancer

Breast tomosynthesis (3-dimensional mammography) may be used with mammography to produce a clear, highly focused 3-dimensional picture of the breast. This technique makes it somewhat easier to detect cancer, especially in women with dense breast tissue. However, this type of mammography exposes women to more radiation than traditional mammography.
Recommendations for routine screening with mammography vary. Experts disagree about
When it should start
How often it should be done
When (or if) it should be stopped
Experts have different recommendations about when to start routine mammography. Most medical organizations recommend screening mammography for some women starting at between ages 40 to 49 and for all women starting at age 50.
Recommendations to start at age 50 are because screening mammography is more accurate in women 50 or older. The reason is that as women age, fatty tissue replaces fibroglandular tissue in the breast. Abnormalities next to fatty tissue are easier to detect with a mammogram.
The benefit of screening is not as clear in women aged 40 to 49. Experts are concerned about anxiety, false positives, and also about starting screening too soon or screening too often because exposure to radiation would be increased.
Women with risk factors for breast cancer are more likely to benefit from starting mammography before age 50. They should discuss the risks and benefits of screening mammograms with their doctor.
Whenever it is started, mammography is then repeated every 1 or 2 years.
Routine mammography may be stopped at age 75, depending on the woman's life expectancy and her wish for continued screening.
Did You Know...
|
The dose of radiation used in mammography is very low and is considered safe.
Mammography may cause some discomfort, but the discomfort lasts only a few seconds. Mammography should be scheduled at a time during the menstrual period when the breasts are less likely to be tender.
Deodorants and powders should not be used on the day of the procedure because they can interfere with the image obtained. The entire procedure takes about 15 minutes.
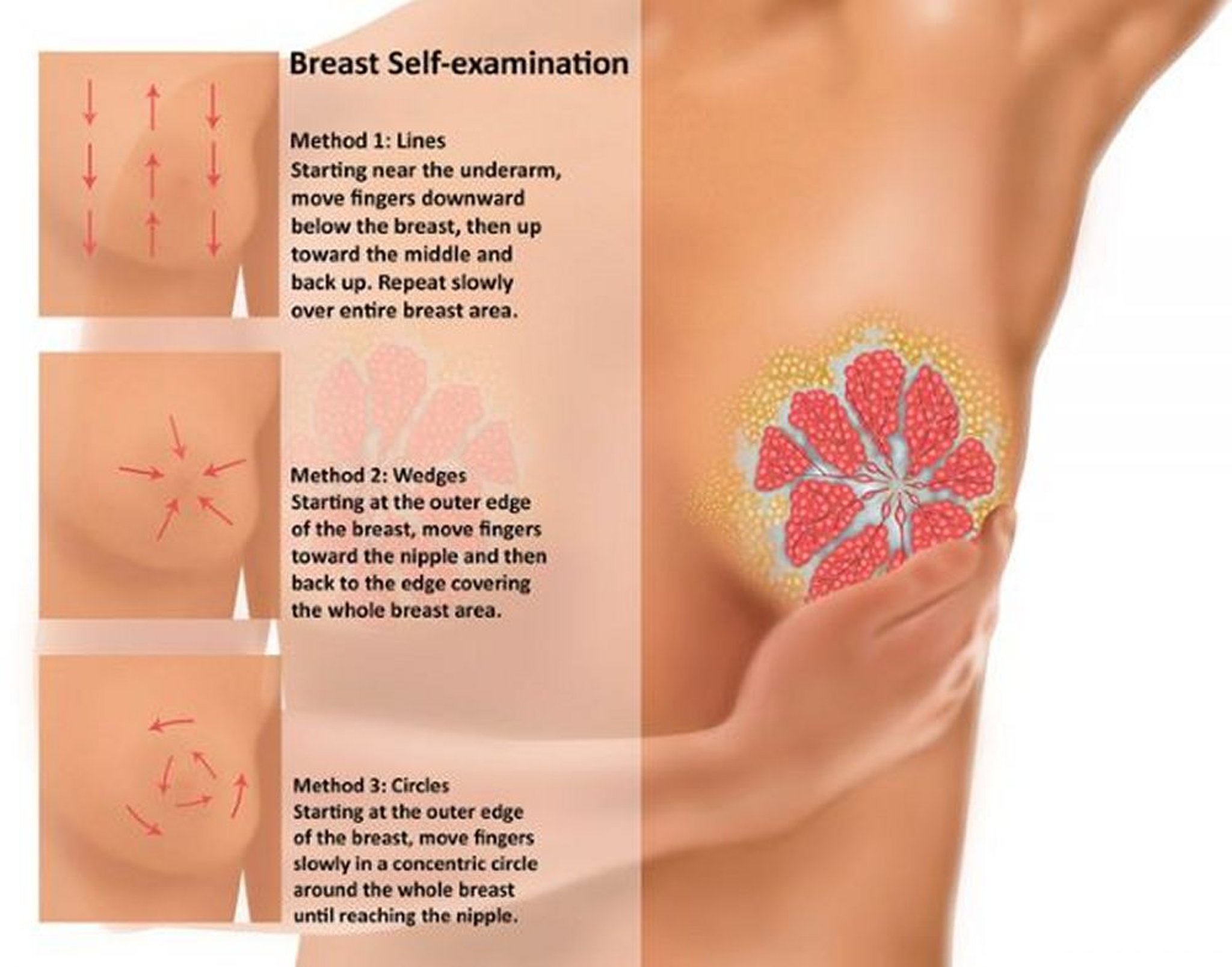
Breast self-awareness
Women should be familiar with how their breasts normally look and feel. Because breast cancer also affects men, men should be aware of changes in or around their nipples. If a woman notices a change, she may want to do a breast self-examination. Women should report any changes to a health care professional right away. In the past, most doctors recommended that women examine their breasts for lumps each month. Most medical organizations no longer recommend that people do monthly or weekly breast self-examinations as a routine way to check for cancer. Doing these examinations when there is no lump or other change does not help detect breast cancer early in women who get screening mammograms.

Gwen Shockey/SCIENCE PHOTO LIBRARY
Breast examination by a health care professional
A breast examination may be part of a routine physical examination. However, as with breast self-examination, a doctor's examination may miss a cancer. If women need or want screening, a more sensitive test, such as mammography, should be done, even if a doctor's examination did not detect any abnormalities. Many doctors and medical organizations no longer require an annual breast examination by a doctor.
During the examination, a doctor inspects the breasts for irregularities, dimpling, tightened skin, lumps, and a discharge. The doctor feels (palpates) each breast with a flat hand and checks for enlarged lymph nodes in the armpit—the area most breast cancers invade first—and above the collarbone. Normal lymph nodes cannot be felt through the skin, so those that can be felt are considered enlarged. However, noncancerous conditions can also cause lymph nodes to enlarge. Lymph nodes that can be felt are biopsied to see if they are abnormal.
Magnetic resonance imaging
MRI is usually used to screen women with a high risk of breast cancer, such as those with a BRCA mutation. For these women, screening should also include mammography and breast examination by a health care professional. MRI may be recommended for women with dense breast tissue as part of an overall assessment that includes evaluation of risk.
Prevention of Breast Cancer
Taking medications that decrease the risk of breast cancer (chemoprevention) may be recommended for the following women:
Those who are over age 35 and have had a previous lobular carcinoma in situ or abnormal tissue structure (atypical hyperplasia) in the milk ducts or milk-producing glands
Those who have a BRCA1 or BRCA2 or another high-risk gene mutation
Those who are between the ages of 35 and 59 and have a high risk of developing breast cancer based on their current age, age when menstruation began (menarche), age at the first birth of a child, number of first-degree relatives with breast cancer, and results of prior breast biopsies
Medications that block estrogen receptors in breast tissue may be used to prevent breast cancer. They include
Women should ask their doctor about possible side effects before taking these medications.
Risks of include
Cancer of the uterus (endometrial cancer)
Possibly stroke
These risks are higher for older women.
Both medications may also increase bone density and thus benefit women who have osteoporosis.






