


The need for treatment of arrhythmias depends on the symptoms and the seriousness of the arrhythmia. Treatment is directed at causes. If necessary, direct antiarrhythmic therapy, including antiarrhythmic drugs, cardioversion-defibrillation, implantable cardioverter-defibrillators (ICDs), pacemakers (and a special form of pacing, cardiac resynchronization therapy), catheter ablation, surgery, or a combination, is used.
ICDs cardiovert or defibrillate the heart in response to ventricular tachycardia (VT) or ventricular fibrillation (VF). Tiered-therapy ICDs also provide antibradycardia pacing and antitachycardia pacing (to terminate responsive atrial or ventricular tachycardias) and store intracardiac electrograms.
ICDs are implanted subcutaneously or subpectorally, with electrodes inserted transvenously into the right ventricle and sometimes also the right atrium. A biventricular ICD also has a left ventricular epicardial lead placed via the coronary sinus venous system or via thoracotomy to allow cardiac resynchronization therapy pacing (CRT-D). ICD platforms also include an ICD that is completely implanted subcutaneously (S-ICD) with no intravascular components, and a wearable vest-like defibrillator for short-term use.

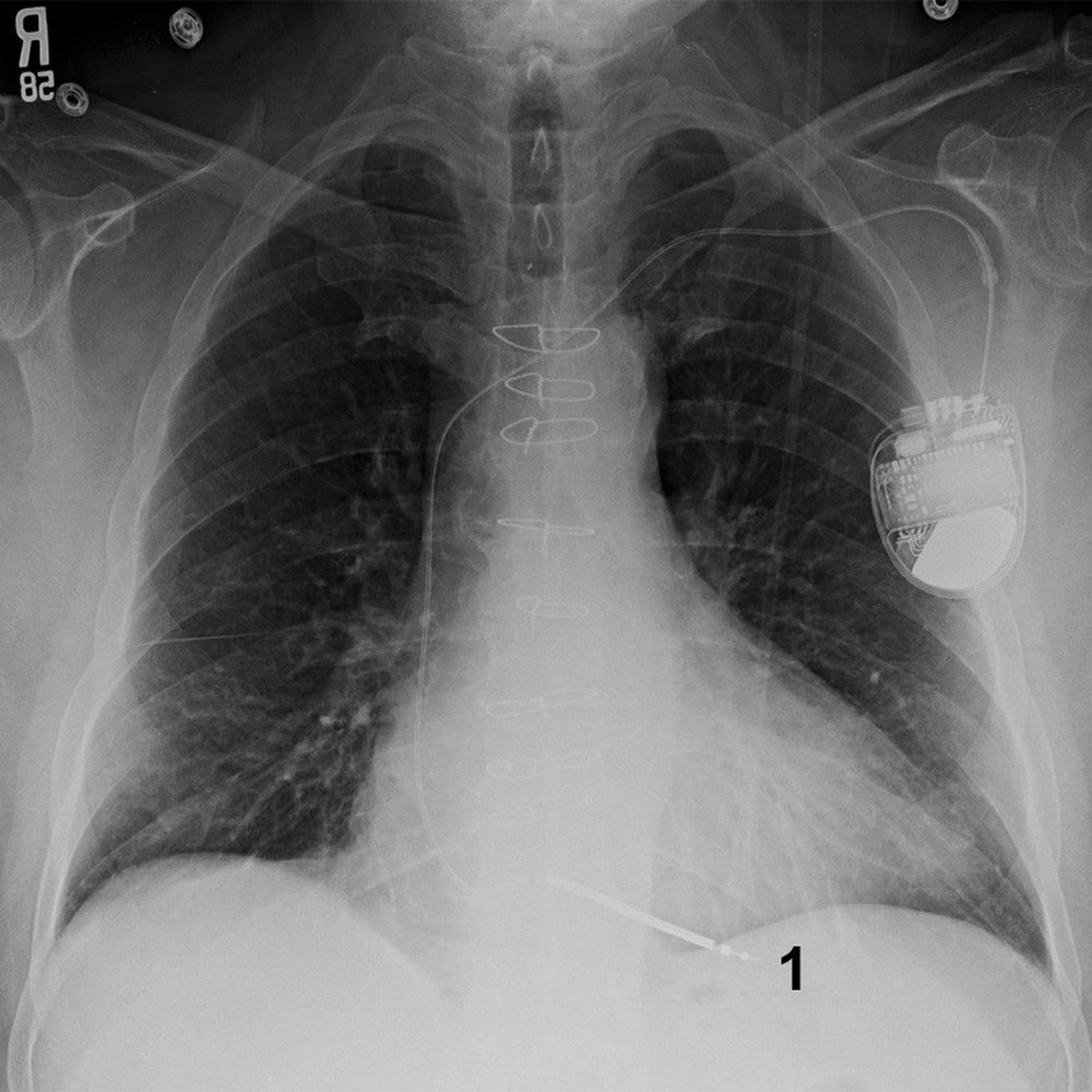
© 2017 Elliot K. Fishman, MD.
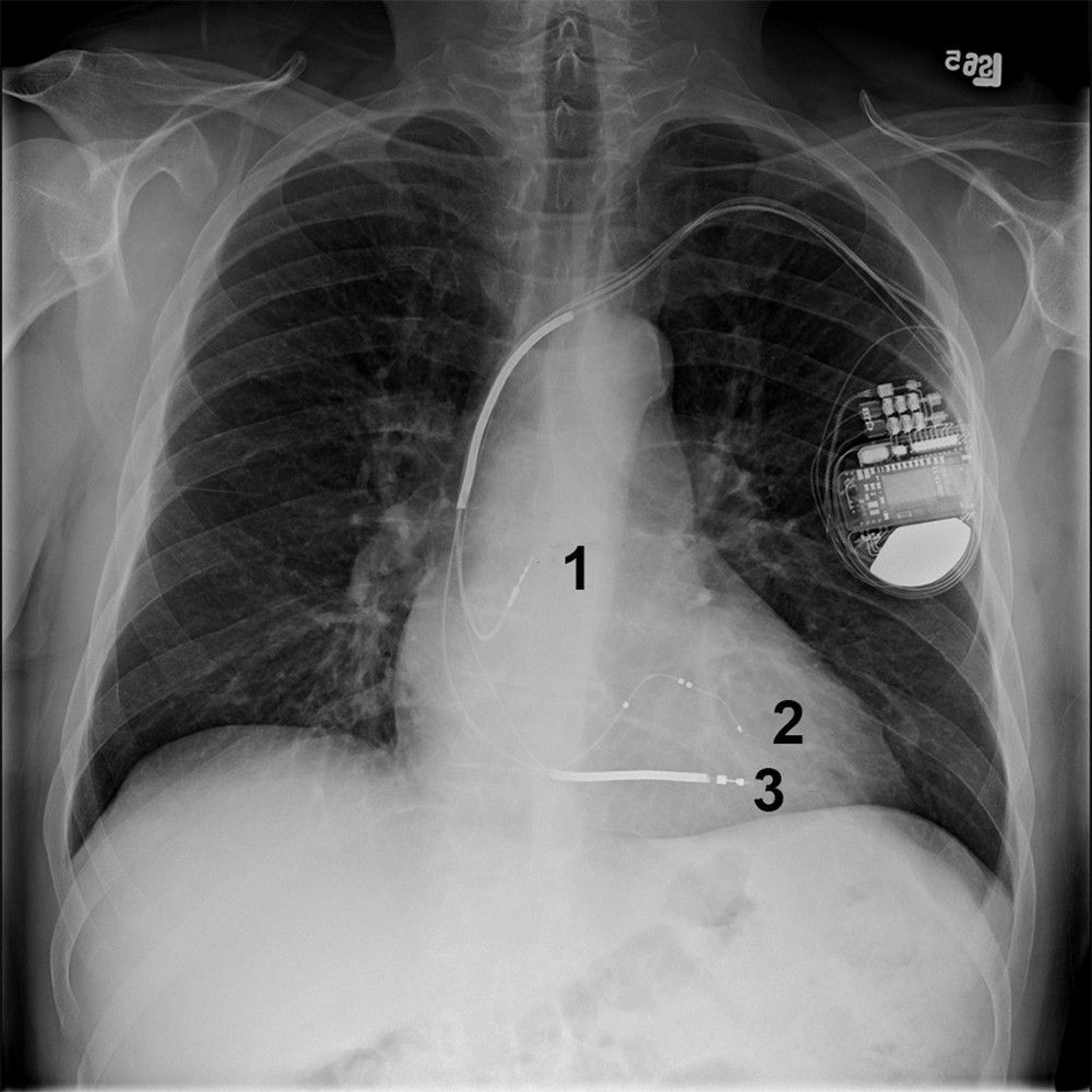
© 2017 Elliot K. Fishman, MD.
Impulse generators for ICDs typically last about 5 to 7 years.
Indications for ICDs
ICDs are the preferred treatment for patients who have had
An episode of VF or hemodynamically significant VT not due to reversible or transient conditions (eg, electrolyte disturbance, antiarrhythmic drug proarrhythmia, acute myocardial infarction)
ICDs may also be indicated for patients with VT or VF inducible during an electrophysiologic study and for patients with idiopathic or ischemic cardiomyopathy, a left ventricular ejection fraction of < 35%, and a high risk of VT or VF. Other indications (see table Indications for Implantable Cardioverter-Defibrillators) are less clear .
Because ICDs treat rather than prevent VT or VF, patients prone to these arrhythmias may require both an ICD and antiarrhythmic drugs to reduce the number of episodes and need for uncomfortable shocks; this approach also prolongs the life of the ICD.
Indications for Implantable Cardioverter-Defibrillators in Ventricular Tachycardia and Ventricular Fibrillation
Level of Evidence | Specific Indications |
|---|---|
Indicated (established by evidence) | Hemodynamically unstable VT or VF when there is no transient or reversible cause Hemodynamically stable sustained VT in patients with a structural heart disorder Syncope of undetermined origin with sustained monomorphic VT induced during an electrophysiologic study Ischemic cardiomyopathy, NYHA class II or III heart failure symptoms during optimal medical therapy, and LV ejection fraction ≤ 0.35 measured at least 40 days post-MI and at least 90 days post-revascularization Ischemic cardiomyopathy, NYHA class I heart failure symptoms during optimal medical therapy, and LV ejection fraction ≤ 30% measured at least 40 days post-MI and at least 90 days post-revascularization Nonischemic dilated cardiomyopathy, NYHA class II or III heart failure symptoms during optimal medical therapy, and LV ejection fraction ≤ 0.35 Ischemic cardiomyopathy, nonsustained VT, LV ejection fraction ≤ 40% measured at least 40 days post-MI, and inducible VF or sustained VT detected during an electrophysiologic study Arrhythmogenic right ventricular cardiomyopathy (ARVC) with sustained VT, resuscitated cardiac arrest, or severe right or left ventricular systolic dysfunction Long QT syndrome with documented VT or symptoms suggestive thereof while receiving beta-blocker drug therapy Short QT interval with sustained VT, or cardiac arrest Brugada syndrome with type 1 ECG pattern and syncope presumed to be due to VT Catecholaminergic polymorphic ventricular tachycardia (CPVT) with sustained VT or syncope on beta blocker drug therapy Early repolarization with sustained VT or cardiac arrest |
Possibly indicated and supported by bulk of evidence | Idiopathic dilated cardiomyopathy, significant LV dysfunction during optimal medical therapy, and unexplained syncope Cardiomyopathy due to a Lamin A/C mutation with unexplained syncope, or an independent indication for a permanent pacemaker, or ≥ 2 high-risk factors (nonsustained VT, intermediate LVEF 35% to 44%, non-missense mutation, male sex) Hypertrophic cardiomyopathy (HCM) with ≥ 1 high risk factors other than sustained VT/VF (family history of premature sudden death, unexplained recent syncope, LV thickness ≥ 30 mm) or with either abnormal exercise BP response or nonsustained VT plus ≥ 1 other sudden death risk modifiers (age < 30 years, late gadolinium enhancement on cardiac MRI, LV outflow tract obstruction, LV aneurysm, remote syncope) ARVC without sustained VT/VF or severe right or left ventricular systolic dysfunction but with prior syncope or with multiple other risk factors for ventricular tachyarrhythmias (Towbin JA et al) NYHA class IV heart failure in nonhospitalized patients awaiting cardiac transplantation Cardiac sarcoidosis with LV ejection fraction > 35% who have ≥ 1 of the following: unexplained syncope, significant myocardial scar visible on cardiac MRI or PET scan, inducible sustained VT or VF, or an independent indication for a permanent pacemaker Giant cell myocarditis with VF or unstable VT during optimal medical therapy |
Possibly indicated but less well supported by evidence | Idiopathic dilated cardiomyopathy, NYHA class I heart failure symptoms during optimal medical therapy, LV ejection fraction ≤ 0.35 Long QT syndrome with no symptoms but a QTc > 0.50 second during beta-blocker therapy Syncope and an advanced structural heart disorder if invasive and noninvasive investigations have not identified a cause HCM with nonsustained VT or an abnormal blood pressure response to exercise but no other sudden death risk modifiers ARVC without sustained VT/VF or severe right or left ventricular systolic dysfunction but with fewer other risk factors for ventricular tachyarrhythmias (Towbin et al) |
Not indicated | Syncope of unknown etiology in absence of inducible VT or VF and without a structural heart disorder Incessant VT or VF VT or VF with mechanisms amenable to catheter or surgical ablation VT or VF due to transient or reversible disorders when correction is feasible and likely to prevent recurrence Psychiatric disorders that may worsen with ICD implantation or that preclude follow-up Patients with no reasonable expectation of survival with an acceptable functional status for ≥ 1 year Patients with NYHA class IV drug-refractory heart failure symptoms who are not candidates for cardiac transplantation or a CRT ICD |
ARVC = arrhythmogenic right ventricular cardiomyopathy; BP = blood pressure; CPVT = catecholaminergic polymorphic ventricular tachycardia; CRT = cardiac resynchronization therapy; HCM = hypertrophic cardiomyopathy; ICD = implantable cardioverter defibrillator; LV = left ventricular; MI = myocardial infarction; NYHA = New York Heart Association; QTc = corrected QT interval; RV = right ventricular; VF = ventricular fibrillation; VT = ventricular tachycardia. | |
Data from Al-Khatib SM, Stevenson WG, Ackerman MJ, et al: 2017 AHA/ACC/HRS guideline for management of patients with ventricular arrhythmias and the prevention of sudden death: a report of the American College of Cardiology Foundation, American Heart Association Task Force on Clinical Practice Guidelines and the Heart Rhythm Society. J Am Coll Cardiol 72:e91–e220, 2018 doi: 10.1016/j.jacc.2017.10.054 and Towbin JA, McKenna WJ, Abrams DJ, et al: 2019 HRS expert consensus statement on evaluation, risk stratification, and management of arrhythmogenic cardiomyopathy. Heart Rhythm 16:e301–e372, 2019. | |
ICD malfunction
ICDs may malfunction by
Delivering inappropriate pacing or shocks
Not delivering pacing or shocks when needed
ICDs may deliver inappropriate pacing or shocks in response to sinus rhythm, supraventricular tachycardia, atrial fibrillation, atrial flutter, or nonphysiologically generated impulses (eg. due to lead fracture).
ICDs may not deliver appropriate pacing or shocks when needed because of factors such as lead or impulse generator migration, undersensing, an increase in pacing threshold due to fibrosis at the site of prior shocks, and battery depletion.
When an ICD discharges
In patients who report that the ICD has discharged but that no associated symptoms of syncope, dyspnea, chest pain, or persistent palpitations occurred, follow up with the ICD clinic and/or the electrophysiologist within the week is appropriate. The ICD can then be electronically interrogated to determine the reason for discharge. If such associated symptoms were present, or the patient received multiple shocks, emergency department referral is indicated to look for a treatable cause (eg, coronary ischemia, electrolyte abnormality) or device malfunction.







