

Part of pre-intubation and emergency rescue breathing procedures, the head tilt–chin lift maneuver and the jaw-thrust maneuver are 2 noninvasive, manual means to help restore upper airway patency when the tongue occludes the glottis, which commonly occurs in patients who are obtunded or unconscious.
(See also Respiratory Arrest and Airway Establishment and Control.)
These methods require active ongoing attendance by the operator and are an integral part of bag-valve-mask ventilation (BVM).
Positioning of the patient in a proper sniffing position, when possible, is important for these manual methods as well as for invasive methods of airway management (ie, supraglottic and tracheal artificial airways).
These methods should be supplemented with use of oropharyngeal or nasopharyngeal airways (1).
The addition of continuous positive airway pressure may achieve airway patency when these manual methods alone fail.
Indications
Treatment of suspected upper airway obstruction in obtunded or unresponsive patients
Part of initial emergency treatment for apnea or impending respiratory arrest
Improvement of airway patency (decreased sonorous respirations) during BVM ventilation and sometimes during spontaneous breathing
Contraindications
Absolute contraindications:
There is no medical contraindication to providing head tilt–chin lift and jaw-thrust maneuvers; however, performing these maneuvers as part of providing ventilatory support should not be initiated if there is a legal contraindication such as a do-not-resuscitate order or specific advance directive declining ventilatory support.
Relative contraindications:
Suspected or actual cervical spine injury
Tilting the head or otherwise moving the neck is contraindicated in a patient with a possible cervical spine injury, but maintaining an airway and ventilation is a greater priority. In the setting of a possible cervical spine injury, the jaw-thrust maneuver, in which the neck is held in a neutral position, should be performed instead of the head tilt–chin lift maneuver.
Complications
Complications are uncommon and include:
Spinal cord injury if the cervical spine has an unstable bony or ligamentous injury
Exacerbation of mandibular injury
Equipment
Gloves, mask, gown (ie, universal precautions)
Towels, sheets, or commercial devices (ramps) for elevating neck and head into optimal positioning
Suctioning apparatus and Yankauer catheter to suction oral secretion or any liquids in the oropharynx
Magill forceps (if needed to remove easily accessible foreign bodies in the oropharynx)
Additional Considerations
Suction should be used if necessary to clear the upper airway.
Relevant Anatomy
Aligning the external auditory canal with the sternal notch may help open the upper airway and establishes the best position to view the airway if endotracheal intubation becomes necessary.
The degree of head elevation that best aligns the ear and sternal notch varies (eg, no elevation in children with a large occiput, a large degree in patients with obesity).
Positioning
The sniffing position—only in the absence of cervical spine injury:
Position the patient supine on the stretcher.
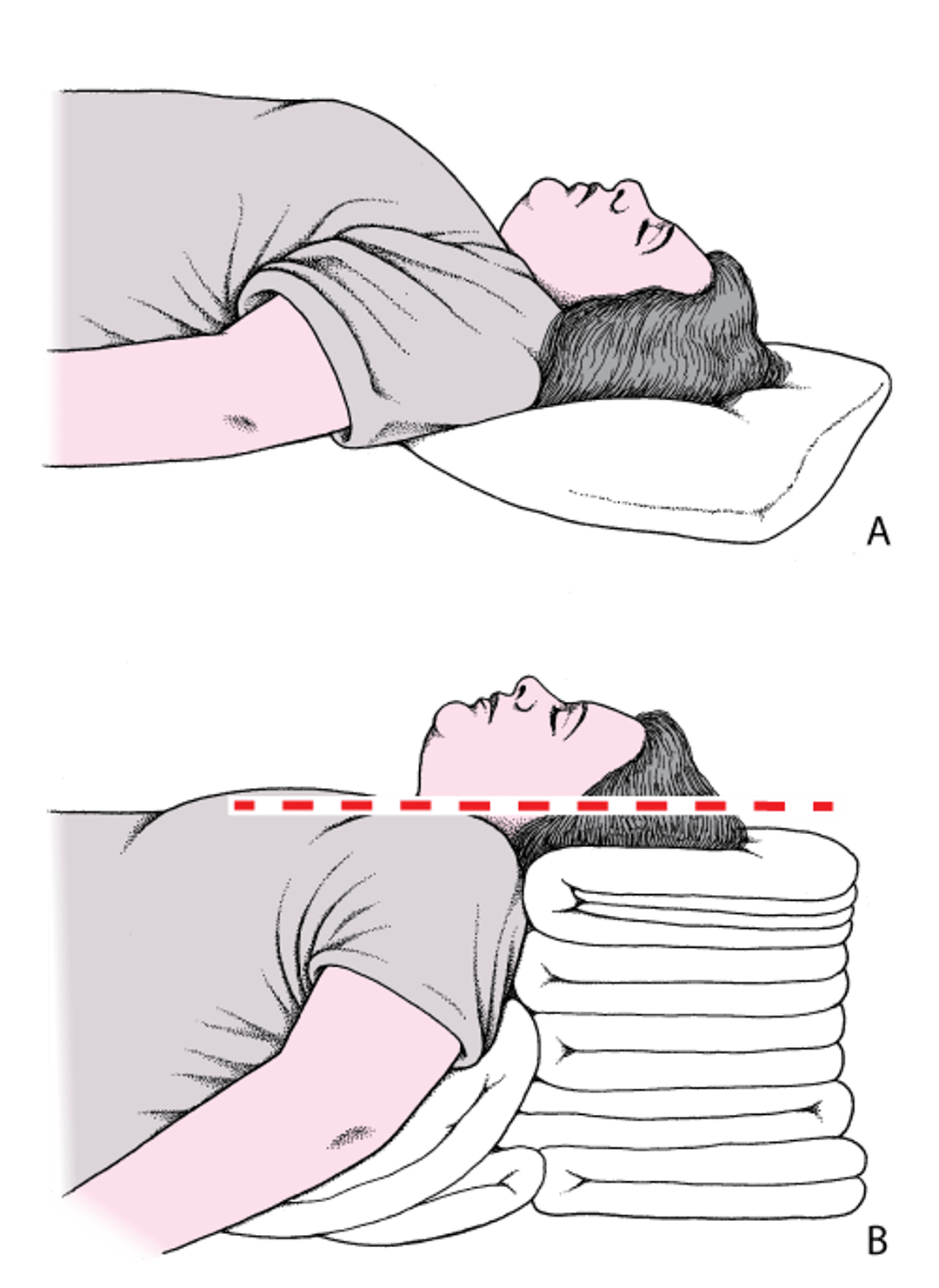
Align the upper airway for optimal air passage by placing the patient into a proper sniffing position. Proper sniffing position aligns the external auditory canal with the sternal notch. To achieve the sniffing position, folded towels or other materials may need to be placed under the head, neck, or shoulders, so that the neck is flexed on the body and the head is extended on the neck. In patients with obesity, many folded towels or a commercial ramp device may be needed to sufficiently elevate the shoulders and neck. In children, padding is usually needed behind the shoulders to accommodate the enlarged occiput.
Head and Neck Positioning to Open the Airway: Sniffing Position
A: The head is flat on the stretcher; the airway is constricted. B: The ear and sternal notch are aligned, with the face parallel to the ceiling (in the sniffing position), opening the airway. Adapted from Levitan RM, Kinkle WC: The Airway Cam Pocket Guide to Intubation, ed. 2. Wayne (PA), Airway Cam Technologies, 2007. |

If cervical spine injury is a possibility:
Position the patient supine or at a slight incline on the stretcher.
Avoid moving the neck and perform the jaw-thrust maneuver. Do not perform the head tilt–chin lift.
Step-by-Step Description of Procedure
Head tilt–chin lift:
Tilt the patient’s head back by pushing down on the forehead.
Place the tips of your second and third fingers under the chin and pull up on the mandible (not on the soft tissues). This lifts the tongue away from the posterior pharynx and improves airway patency.
Be sure to pull up only on the bony parts of the mandible. Pressure to the soft tissues of the neck may obstruct the airway.
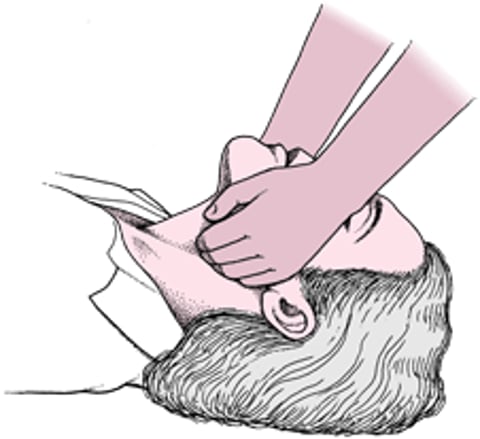
Jaw thrust:
Stand at the head of the stretcher and place your palms on the patient’s temples and your fingers under the mandibular rami.
In patients with possible cervical spine injury, avoid extending the neck.
Lift the mandible upward with your fingers, at least until the lower incisors are higher than the upper incisors. This maneuver lifts the tongue along with the mandible, thus relieving upper airway obstruction.
Be sure to pull or push up only on the bony parts of the mandible. Pressure to the soft tissues of the neck may obstruct the airway.
Successful performance of either of these maneuvers should result in no upper airway obstruction sounds (eg, no sonorous respirations) during spontaneous or BVM ventilations.
Jaw Thrust


Aftercare
Maintain these positions as long as necessary.
Reference
1. Panchal AR, Bartos JA, Cabañas JG, et al. Part 3: Adult Basic and Advanced Life Support: 2020 American Heart Association Guidelines for Cardiopulmonary Resuscitation and Emergency Cardiovascular Care. Circulation 2020;142(16_suppl_2):S366-S468. doi:10.1161/CIR.0000000000000916





