

The tongue may undergo changes in color and surface. Changes may be focal or involve most of the tongue. Some changes are asymptomatic; others cause tongue discomfort.
(See also table in topic Systemic Disorders and the Mouth.)
Tongue color changes
The papillary surface (dorsum) of the tongue may become discolored by smoking or chewing tobacco, by consuming certain foods or vitamins, or by surface growth of pigmented bacteria.
Black discoloration on the dorsum may be due to oral bismuth preparations. Brushing the tongue with a toothbrush or scraping it with a tongue scraper may remove such discoloration.
Blue-black discoloration, focal, small, and unchanging, on the ventral surface may be an amalgam tattoo.
A pale, smooth tongue can be caused by atrophic glossitis, which can occur with iron deficiency or vitamin B12 deficiency (1).
Magenta tongue suggests vitamin B12 deficiency.
A strawberry-red tongue may be the first sign of scarlet fever or, in a young child, be among the signs of Kawasaki disease or in multisystem inflammatory syndrome in children (MIS-C), an uncommon complication of COVID-19.


This tongue is erythematous. Characteristics of strawberry tongue are sloughing of the filiform papillae (caused by the systemic inflammatory process) and persistence of the fungiform papillae, which appear as the seeds of the strawberry. Strawberry tongue is not specific to Kawasaki disease and multisystem inflammatory syndrome in children (MIS-C); it may also be present in streptococcal and staphylococcal toxin-mediated disease.
SCIENCE PHOTO LIBRARY
A smooth red tongue and painful mouth may indicate general inflammation of the tongue (glossitis) or be caused by niacin deficiency.
Tongue surface changes
The most common tongue surface changes, all 3 benign, are:
Geographic tongue (benign migratory glossitis, or erythema migrans)
Fissured tongue (often associated with geographic tongue)
Hairy tongue
In geographic tongue, areas of the tongue are red and smooth (due to atrophy of filiform papilla) and are often surrounded by a slightly elevated yellow-white border. Other areas may be white or yellow and rough, representing psoriaform changes or coexisting psoriasis itself. The areas of discoloration can migrate over a period of weeks to years. The condition is usually painless, and no treatment is needed. Geographic tongue is more common in women than in men, and the risk of having it is lower among people who smoke (2).
If patients have symptoms, applying low doses of a topical glucocorticoid sometimes helps.

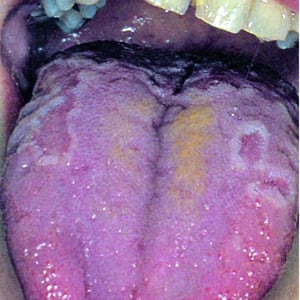
This photo shows some elevated white borders surrounding smooth, red areas of atrophy and loss of papillae. Other areas have a rough white or yellow surface (psoriaform changes). The lesions occur in multiple locations on the tongue and may coalesce to form a maplike appearance.
This photo shows some elevated white borders surrounding smooth, red areas of atrophy and loss of papillae. Other areas
© Springer Science+Business Media


Benign migratory glossitis (geographic tongue) in which the normal projections (papillae) on the tongue surface are lost and surrounded by raised white-yellow areas. The tongue also shows fissuring (deep grooves on the top and sides of the tongue), which often coexists with geographic tongue.
© Springer Science+Business Media
Benign migratory glossitis (geographic tongue) in which the normal projections (papillae) on the tongue surface are los


The tongue is brownish and has a hairy appearance due to accumulation of keratin on the top of the tongue (papillae).
The tongue is brownish and has a hairy appearance due to accumulation of keratin on the top of the tongue (papillae).
Photo courtesy of Craig B. Fowler, DDS.

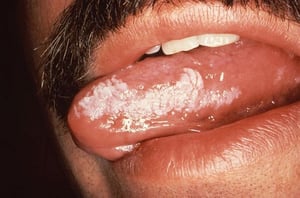
Oral hairy leukoplakia appears as verrucous white outgrowths on the lateral margins of the tongue.
Oral hairy leukoplakia appears as verrucous white outgrowths on the lateral margins of the tongue.
CDC/Sol Silverman, Jr., D.D.S.
This photo shows some elevated white borders surrounding smooth, red areas of atrophy and loss of papillae. Other areas have a rough white or yellow surface (psoriaform changes). The lesions occur in multiple locations on the tongue and may coalesce to form a maplike appearance.
This photo shows some elevated white borders surrounding smooth, red areas of atrophy and loss of papillae. Other areas
© Springer Science+Business Media
Benign migratory glossitis (geographic tongue) in which the normal projections (papillae) on the tongue surface are lost and surrounded by raised white-yellow areas. The tongue also shows fissuring (deep grooves on the top and sides of the tongue), which often coexists with geographic tongue.
© Springer Science+Business Media
Benign migratory glossitis (geographic tongue) in which the normal projections (papillae) on the tongue surface are los
The tongue is brownish and has a hairy appearance due to accumulation of keratin on the top of the tongue (papillae).
The tongue is brownish and has a hairy appearance due to accumulation of keratin on the top of the tongue (papillae).
Photo courtesy of Craig B. Fowler, DDS.
Oral hairy leukoplakia appears as verrucous white outgrowths on the lateral margins of the tongue.
Oral hairy leukoplakia appears as verrucous white outgrowths on the lateral margins of the tongue.
CDC/Sol Silverman, Jr., D.D.S.
Fissured tongue is an idiopathic condition occurring with varying prevalence rate ranging from approximately 3% up to 30% (3, 4). Deep grooves are located either along the midline or are distributed over the dorsum. Fissured tongue may occur with geographic tongue, Down syndrome, or Melkersson-Rosenthal syndrome, a rare syndrome that also features facial palsy and granulomatous cheilitis (5).
Hairy tongue is due to accumulation of keratin on normal filiform papillae that gives the tongue a hairy appearance. Hairy tongue is caused by lack of mechanical stimulation to the tongue (eg, due to poor oral hygiene) with trapping of residual food debris among the papillae (6). Hairy tongue may also appear after a fever, antibiotic treatment, or with excessive use of peroxide mouthwash. It is common in people who smoke heavily. Hairy tongue should not be confused with hairy leukoplakia, which usually is associated with immunodeficiency (especially HIV infection) and caused by the Epstein-Barr virus (7). It appears as white, hairy-appearing patches on the side of the tongue.
Other tongue surface changes include tongue ulcers, whitish patches, and red patches.
Tongue ulcers may be herpetiform aphthous ulcers (ventral tongue surface) or be due to trauma from accidental biting or from rubbing against a fractured tooth or restoration.
Whitish patches on the tongue, similar to those sometimes found inside the cheeks (buccal mucosa), may be due to:
Fever
Dehydration
Mouth breathing
Oral candidiasis (thrush)

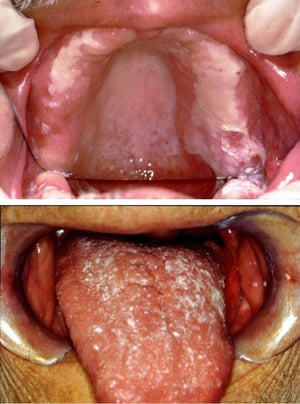
Oral candidiasis takes many forms, including angular cheilitis and pseudomembranous plaques on the oral mucosae, which can be associated with dentures, as in this image (top), or develop on the tongue (bottom) or pharynx.
Oral candidiasis takes many forms, including angular cheilitis and pseudomembranous plaques on the oral mucosae, which
Images courtesy of Jonathan Ship, MD.


This photo shows a thick plaque of leukoplakia extending widely over the dorsum of the tongue.
This photo shows a thick plaque of leukoplakia extending widely over the dorsum of the tongue.
© Springer Science+Business Media


Erythroplakia is a general term that can describe red, flat, or eroded velvety lesions that develop in the mouth. In this image, an exophytic squamous cell carcinoma on the tongue is surrounded by a margin of erythroplakia.
Erythroplakia is a general term that can describe red, flat, or eroded velvety lesions that develop in the mouth. In th
Image provided by Jonathan A. Ship, DMD.
Oral candidiasis takes many forms, including angular cheilitis and pseudomembranous plaques on the oral mucosae, which can be associated with dentures, as in this image (top), or develop on the tongue (bottom) or pharynx.
Oral candidiasis takes many forms, including angular cheilitis and pseudomembranous plaques on the oral mucosae, which
Images courtesy of Jonathan Ship, MD.
This photo shows a thick plaque of leukoplakia extending widely over the dorsum of the tongue.
This photo shows a thick plaque of leukoplakia extending widely over the dorsum of the tongue.
© Springer Science+Business Media
Erythroplakia is a general term that can describe red, flat, or eroded velvety lesions that develop in the mouth. In this image, an exophytic squamous cell carcinoma on the tongue is surrounded by a margin of erythroplakia.
Erythroplakia is a general term that can describe red, flat, or eroded velvety lesions that develop in the mouth. In th
Image provided by Jonathan A. Ship, DMD.
Red patches on the tongue may indicate:
Atrophic glossitis related to pernicious anemia
Median rhomboid glossitis (a form of erythematous candidiasis)
Traumatic ulcer from accidental biting or rubbing against a sharp tooth or restoration.
Leukoplakia and erythroplakia may be manifestations of oral squamous cell carcinoma; biopsy is indicated for both.
General references
1. Lopez A, Cacoub P, Macdougall IC, et al. Iron deficiency anaemia. Lancet. 2016;387(10021):907-916. doi:10.1016/S0140-6736(15)60865-0
2. Shulman JD, Carpenter WM. Prevalence and risk factors associated with geographic tongue among US adults. Oral Dis. 2006;12(4):381-386. doi: 10.1111/j.1601-0825.2005.01208.x
3. Feng J, Zhou Z, Shen X, et al. Prevalence and distribution of oral mucosal lesions: a cross-sectional study in Shanghai, China. J Oral Pathol Med. 2015;44(7):490-494. doi:10.1111/jop.12264
4. Yarom N, Cantony U, Gorsky M. Prevalence of fissured tongue, geographic tongue and median rhomboid glossitis among Israeli adults of different ethnic origins. Dermatology. 2004;209(2):88-94. doi:10.1159/000079590
5. Rose AE, Leger M, Chu J, et al. Cheilitis granulomatosa. Dermatol Online J. 2011;17(10):15. Published 2011 Oct 15.
6. Randall DA, Wilson Westmark NL, Neville BW. Common Oral Lesions. Am Fam Physician. 2022;105(4):369-376.
7. Farisyi MA, Sufiawati I. Detection of Epstein-Barr virus DNA in saliva of HIV-1-infected individuals with oral hairy leukoplakia. Oral Dis. 2020;26 Suppl 1:158-160. doi:10.1111/odi.13400
Drug Information for the Topic





