

Human immunodeficiency virus (HIV) infection (infection with either HIV-1 or HIV-2) destroys CD4+ lymphocytes and impairs cell-mediated immunity, increasing risk of certain infections and cancers. Initial infection may cause nonspecific febrile illness. Risk of subsequent manifestations—related to immunodeficiency—is proportional to the level of CD4+ lymphocyte depletion. HIV can directly damage the brain, gonads, kidneys, and heart, causing cognitive impairment, hypogonadism, renal insufficiency, or cardiomyopathy. Manifestations range from asymptomatic carriage of the virus to end-stage HIV (acquired immune deficiency syndrome [AIDS]), which is defined by the presence of an AIDS-defining illness (serious opportunistic infections or cancers) or a CD4 count < 200/mcL. HIV infection can be diagnosed by antibody, nucleic acid (HIV RNA), or antigen (p24) testing. Screening should be routinely offered to all adults and adolescents ages 13 to 64. In addition, pregnant women should be tested for HIV early in each pregnancy, even if they have been screened during previous pregnancies. Treatment aims to suppress HIV replication by using combinations of ≥ 2 medications that inhibit HIV enzymes; treatment can restore immune function in most patients if suppression of replication is sustained.
(See also Human Immunodeficiency Virus (HIV) Infection in Infants and Children.)
Human immunodeficiency virus (HIV) is a retrovirus. Retroviruses are enveloped RNA viruses defined by their mechanism of replication via reverse transcription to produce DNA copies that integrate into the host cell's genome.
There are 2 HIV types, HIV-1 and HIV-2. HIV-1 causes most HIV infections worldwide, but HIV-2 causes a substantial proportion of infections, particularly in parts of West Africa (1). In some areas of West Africa, both viruses are prevalent and may coinfect patients. HIV-2 appears to be less virulent than HIV-1.
HIV-1 originated in Central Africa in the first half of the 20th century, when a closely related chimpanzee virus first infected humans. Epidemic global spread began in the late 1970s, and AIDS was recognized in 1981.
General reference
1. Campbell-Yesufu OT, Gandhi RT: Update on human immunodeficiency virus (HIV)-2 infection. Clin Infect Dis 52(6):780-787, 2011. doi: 10.1093/cid/ciq248
Epidemiology of HIV Infection
The following global HIV statistics were estimated by the World Health Organization (WHO) in 2022 (see HIV Data and Statistics):
Global prevalence of HIV – 39 million
Children (0 to 14 years of age) with HIV – 1.5 million
People newly diagnosed with HIV infection – 1.3 million; since 2010, the number of people acquiring HIV has been reduced by 38%, from 2.1 million
Mortality from HIV-related causes – 630,000; since 2010, HIV-related deaths have been reduced by 51%, from 1.3 million
People with HIV receiving antiretroviral therapy – 29.8 million
People with HIV who know their status – 86% (76% of those who know their status are receiving treatment and 71% have suppressed viral loads)
HIV infection is most prevalent in Africa, particularly in sub-Saharan Africa. WHO estimated 2022 statistics in Africa include the following (see HIV Data and Statistics):
Prevalence – 25.6 million (90% knew their status, 82% were receiving treatment, and 76% had suppressed viral loads)
People newly diagnosed with HIV infection – 660,000 (a decrease to 0.57 per 1000 uninfected population from 1.75 per 1000 in 2010)
Mortality from HIV-related causes – 380,000 (a decrease of 56% from 2010)
The most recent estimates for HIV (in people ≥ 13 years old) in the United States from 2021 include the following (see U.S. Statistics: Fast Facts):
Prevalence – 1.2 million people (13% were not aware of their status)
People who acquired HIV – 32,100 (estimated new HIV infections declined 12% from 36,500 in 2017)
People who acquired HIV by subpopulation – Men who have sex with men (22,400 [70%]); people who reported heterosexual contact (7,100 [22%]); people who inject drugs (2,500 ([8%])
HIV has spread through epidemiologically distinct routes:
Heterosexual intercourse (affecting men and women about equally)
Men who have sex with men
Contact with infected blood (eg, through sharing of needles and via blood transfusions in the absence of effective donor-screening measures)
Mother-to-child transmission
Most HIV infections are transmitted through heterosexual contact, but risk factors vary according to region or national income level. For instance, in high-resource countries, transmission among men who have sex with men is usually the most common way infection occurs, whereas people who inject drugs are disproportionally affected in Central and Eastern Europe (1, 2).
In areas where heterosexual transmission is dominant, HIV infection follows routes of trade, transportation, and economic migration to cities and spreads secondarily to rural areas. In Africa, particularly southern Africa, the HIV epidemic has killed tens of millions of adults, creating millions of orphans. Factors associated with increased rates of spread include
Poverty and sexual violence
Limited sexual education and awareness about HIV
Health care systems that do not provide access to HIV testing and antiretroviral medications
Stigmatization, criminalization, and discrimination against people with HIV
Many opportunistic infections that complicate HIV are reactivations of latent infections. Thus, epidemiologic factors that determine the prevalence of latent infections also influence the risk of specific opportunistic infections. In many countries with high rates of HIV infection, prevalence of latent tuberculosis and toxoplasmosis in the general population is higher than in other countries. Dramatic increases in reactivated tuberculosis and toxoplasmic encephalitis have followed the epidemic of HIV-induced immunosuppression in these countries. Similarly, in the United States, the incidence of coccidioidomycosis, common in the Southwest, and histoplasmosis, common in the Midwest, has increased because of HIV infection.
Human herpesvirus 8 infection, which causes Kaposi sarcoma, is common among men who have sex with men but uncommon among other patients with HIV in the United States and Europe. Thus, in the United States, > 90% of people with HIV who have developed Kaposi sarcoma are men who have sex with men (3).
Epidemiology references
1. Vermund SH, Leigh-Brown AJ: The HIV epidemic: High-income countries. Cold Spring Harb Perspect Med 2(5):a007195, 2012. doi: 10.1101/cshperspect.a007195
2. Hamers FF, Downs AM: HIV in central and eastern Europe. Lancet 361(9362):1035-1044, 2003. doi: 10.1016/S0140-6736(03)12831-0
3. Bhutani M, Polizzotto MN, Uldrick TS, et al: Kaposi sarcoma-associated herpesvirus-associated malignancies: Epidemiology, pathogenesis, and advances in treatment. Semin Oncol 42(2):223–246, 2015. doi: 10.1053/j.seminoncol.2014.12.027
Transmission of HIV Infection
Transmission of HIV requires contact with body fluids—specifically blood, semen, vaginal secretions, breast milk, or exudates from wounds or skin and mucosal lesions—that contain free HIV virions or infected cells. Transmission is more likely with the high levels of virions that are typical during primary infection, even when such infections are asymptomatic. Transmission by saliva or droplets produced by coughing or sneezing, although conceivable, is extremely unlikely.
HIV is not transmitted by contact that does not involve exchange of body fluids.
Transmission is usually
Sexual: Direct transmission through sexual activity
Needle- or instrument-related: Sharing of blood-contaminated needles or exposure to contaminated medical instruments
Transfusion- or transplant-related
Vertical: Transmission from an infected mother to child during pregnancy, childbirth, or through breast milk
Sexual transmission of HIV
The sexual practices with the highest risks are those that cause mucosal trauma (see table . A systematic review reported the following risk of transmission per sex act (1):
Receptive anal intercourse: 1 per 72 sex acts
Insertive anal intercourse: 1 per 909
Receptive penile–vaginal intercourse: 1 per 1250
Insertive penile–vaginal intercourse: 1 per 2500
Receptive or insertive oral sex: 0 to 4 per 10,000 exposures
Risk of transmission during oral sex does not increase significantly if semen or vaginal secretions are swallowed. However, open sores in the mouth, bleeding gums, or oral contact with menstrual blood may increase the risk (Oral Sex and HIV Risk ). Other practices that cause mucosal trauma include fisting (inserting most or all of the hand into the rectum or vagina) and using sexual toys. When used during intercourse with a partner with HIV infection, these practices increase the risk of HIV transmission.
Mucous membrane inflammation facilitates HIV transmission. Sores on the mouth, vagina, penis, or rectum increase risk of transmission. Sexually transmitted infections, such as gonorrhea, chlamydia, trichomoniasis, and especially those that cause ulceration (eg, chancroid, herpes, syphilis), increase the risk several-fold.
Risk of transmission is increased in the early and advanced stages of HIV infection when HIV concentrations in plasma and genital fluids are higher. Evidence shows that people with HIV infection treated with antiretroviral therapy who have an undetectable viral load (virally suppressed) do not sexually transmit the virus to their partners (2, 3).
Circumcision seems to reduce the risk of males acquiring HIV infection by about 50%, by removing the penile mucosa (underside of foreskin), which is more susceptible to HIV infection than the keratinized, stratified squamous epithelium that covers the rest of the penis.
HIV Transmission Risk for Several Sexual Activities
Risk* | Activity |
|---|---|
None (unless sores are present) | Dry kissing Body-to-body rubbing and massage Using unshared inserted sexual devices (eg, sex toys) Genital stimulation by a partner but no contact with semen or vaginal fluids Bathing or showering together Contact with feces or urine if skin is intact |
Theoretical (extremely low risk unless sores are present) | Wet kissing Receptive oral-penile sex without ejaculation or if a condom is used Oral-vaginal sex if a barrier is used Oral-anal contact Digital penetration of the vagina or anus, with or without a glove Use of sexual devices/toys that are disinfected before being shared with a partner |
Low | Receptive oral-penile sex without a condom and with ejaculation Oral sex done to a woman if no barrier is used Vaginal or anal intercourse if a condom is used correctly Use of shared but not disinfected inserted sexual devices/toys |
High | Vaginal or anal intercourse with or without ejaculation if a condom is not used or is not used correctly |
* All risks are for sexual encounters with a person who has a detectable HIV viral load. | |
Needle- and instrument-related transmission
The risk of HIV transmission after skin penetration with a medical instrument contaminated with infected blood is approximately 1/400 without postexposure antiretroviral prophylaxis (1). Postexposure antiretroviral prophylaxis as soon as possible after exposure is recommended ( U.S. Guidelines for Management of Occupational Exposures to HIV). Risk appears to be higher if the wound is deep or if blood is inoculated (eg, with a contaminated hollow-bore needle). Risk is also increased with hollow-bore needles and with punctures of arteries or veins compared with solid needles or other penetrating objects coated with blood because larger volumes of blood may be transferred. Thus, sharing needles that have entered the veins of other people is a very high risk activity.
Risk of transmission from clinicians with HIV infection who take appropriate precautions is unclear but appears minimal (Surveillance of Occupationally Acquired HIV/AIDS ). However, extensive investigations of patients cared for by other physicians with HIV infection, including surgeons, have uncovered few other cases.
Vertical (mother-to-child) transmission
HIV can be transmitted from a mother to her fetus or newborn:
During pregnancy, transplacentally
During childbirth
Via breast milk
The overall cumulative risk of vertical transmission without antiretroviral medications is 35 to 45% (4).
Transmission rates can be reduced significantly by treating pregnant women with HIV infection with antiretroviral drugs during pregnancy, labor, and breastfeeding.
Cesarean delivery reduces the risk and is preferred for pregnant women with HIV infection whose viral loads are > 1,000 copies/mL at or near delivery, independent of antepartum antiretroviral therapy, or whose levels are unknown (5).
Testing and prophylactic treatment of the infant also reduce the risk.
HIV is excreted in breast milk. The overall risk of transmission through breastfeeding is approximately 14%, reflecting varying durations of breastfeeding and plasma viral RNA concentrations (eg, risk is high in women who become infected during pregnancy or during the period of breastfeeding) (6).
In high-resource countries, women with HIV infection are advised not to breastfeed (see CDC: Breastfeeding and Special Circumstances). However, in resource-limited settings, breastfeeding is associated with reduced infant morbidity and mortality due to malnutrition and infectious diseases. For women with HIV in low-resource settings, the World Health Organization (WHO) recommends antiretroviral treatment and adherence support combined with breastfeeding for at least 12 months (see WHO: Guidelines on HIV and Infant Feeding).
Because many women with HIV infection and their infants are treated or take prophylactic antiretroviral medications during pregnancy, the incidence of HIV in children has decreased significantly in many countries (see Human Immunodeficiency Virus (HIV) Infection in Infants and Children).
Transfusion- and transplant-related transmission
Screening of blood donors with tests for both antibodies to HIV and HIV RNA has minimized the risk of transmission via blood transfusion. Current risk of transmitting HIV via blood transfusion is estimated to be < 1/2,000,000 per unit transfused in the United States (7). However, in many countries with a high prevalence of HIV, where blood and blood products are not screened for HIV, the risk of transfusion-transmitted HIV infection remains high.
Rarely, HIV has been transmitted via transplantation of organs from HIV-seropositive donors. Infection has developed in recipients of kidney, liver, heart, pancreas, bone, and skin—all of which contain blood—but screening for HIV greatly reduces the risk of transmission. HIV transmission is even more unlikely from transplantation of cornea, ethanol-treated and lyophilized bone, fresh-frozen bone without marrow, lyophilized tendon or fascia, or lyophilized and irradiated dura mater.Rarely, HIV has been transmitted via transplantation of organs from HIV-seropositive donors. Infection has developed in recipients of kidney, liver, heart, pancreas, bone, and skin—all of which contain blood—but screening for HIV greatly reduces the risk of transmission. HIV transmission is even more unlikely from transplantation of cornea, ethanol-treated and lyophilized bone, fresh-frozen bone without marrow, lyophilized tendon or fascia, or lyophilized and irradiated dura mater.
HIV transmission is possible via artificial insemination using sperm from HIV-positive donors. In the United States, sperm washing is considered an effective method of reducing the risk of partner insemination from a known HIV-positive sperm donor.
Transmission references
1. Patel P, Borkowf CB, Brooks JT, et al: Estimating per-act HIV transmission risk: A systematic review. AIDS 28(10):1509-1519, 2014. doi: 10.1097/QAD.0000000000000298
2. Rodger AJ, Cambiano V, Bruun T, et al: Risk of HIV transmission through condomless sex in serodifferent gay couples with the HIV-positive partner taking suppressive antiretroviral therapy (PARTNER): Final results of a multicentre, prospective, observational study. Lancet 393(10189):2428-2438, 2019. doi:10.1016/S0140-6736(19)30418-0
3. Rodger AJ, Cambiano V, Bruun T, et al: Sexual activity without condoms and risk of HIV transmission in serodifferent couples when the HIV-positive partner is using suppressive antiretroviral therapy [published correction appears in JAMA 316(2):171-181, 2016. doi: 10.1001/jama.2016.5148. Erratum in: JAMA316(6):667. Erratum in: JAMA 316(19):2048, 2016. PMID: 27404185
4. Newell ML, Coovadia H, Cortina-Borja M, et al: Mortality of infected and uninfected infants born to HIV-infected mothers in Africa: A pooled analysis. Lancet 364(9441):1236-1243, 2004. doi:10.1016/S0140-6736(04)17140-7
5. ACOG Committee Opinion No. 751 Summary: Labor and delivery management of women with human immunodeficiency virus infection. Obstet Gynecol 32(3):803-804, 2018. doi: 10.1097/AOG.0000000000002821.
6. Dunn DT, Newell ML, Ades AE, Peckham CS: Risk of human immunodeficiency virus type 1 transmission through breastfeeding. Lancet 340(8819):585-588, 1992. doi:10.1016/0140-6736(92)92115-v
7. Steele WR, Dodd RY, Notari EP, et al: HIV, HCV, and HBV incidence and residual risk in US blood donors before and after implementation of the 12-month deferral policy for men who have sex with men. Transfusion 61(3):839-850, 2021. doi: 10.1111/trf.16250
Pathophysiology of HIV Infection
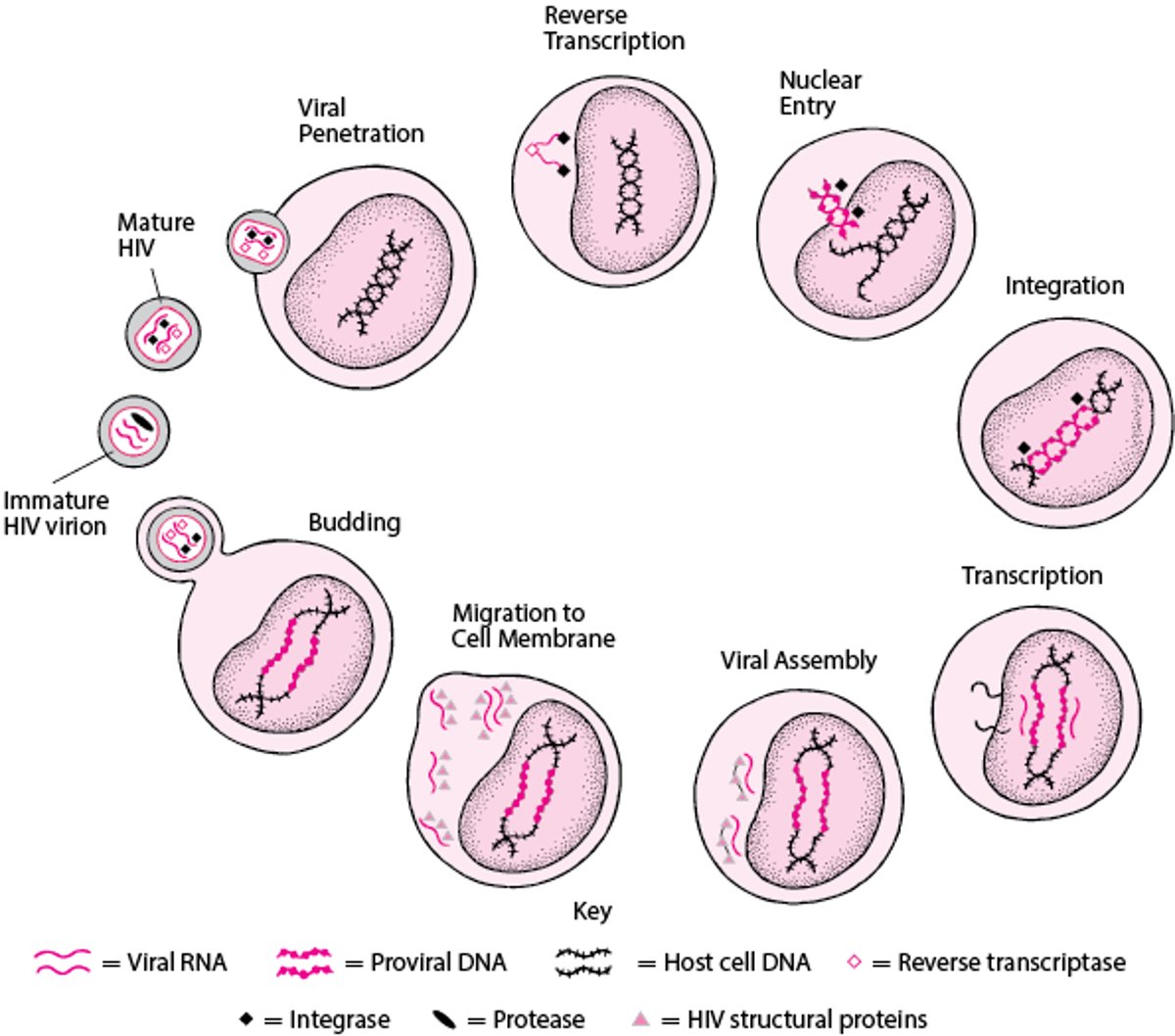
HIV attaches to and penetrates host T cells via CD4+ molecules and chemokine receptors (see figure ). After attachment, HIV RNA and several HIV-encoded enzymes are released into the host cell.
Viral replication requires that reverse transcriptase (an RNA-dependent DNA polymerase) copy HIV RNA, producing proviral DNA; this copying mechanism is prone to errors, resulting in frequent mutations and, thus, new HIV genotypes. These mutations facilitate the generation of HIV that can resist control by the host’s immune system and by antiretroviral drugs.
Proviral DNA enters the host cell’s nucleus and is integrated into the host DNA in a process that involves integrase, another HIV enzyme. With each cell division, the integrated proviral DNA is duplicated along with the host DNA. Subsequently, the proviral HIV DNA can be transcribed to HIV RNA and translated to HIV proteins, such as the envelope glycoproteins 41 and 120. These HIV proteins are assembled into HIV virions at the host cell inner membrane and budded from the cell surface within an envelop of modified human cell membrane. Each host cell may produce thousands of virions.
After budding, protease, another HIV enzyme, cleaves viral proteins, converting the immature virion into a mature, infectious virion.
Simplified HIV Life Cycle
HIV attaches to and penetrates host T cells, then releases HIV RNA and enzymes into the host cell. HIV reverse transcriptase copies viral RNA as proviral DNA. Proviral DNA enters the host cell’s nucleus, and HIV integrase facilitates the proviral DNA’s integration into the host’s DNA. The host cell then produces HIV RNA and HIV proteins. HIV proteins are assembled into HIV virions and bud from the cell surface. HIV protease cleaves viral proteins, converting the immature virion to a mature, infectious virus. |

Infected CD4+ lymphocytes produce > 98% of plasma HIV virions. A subset of infected CD4+ lymphocytes constitutes a reservoir of HIV that can reactivate (eg, if antiviral treatment is stopped).
In moderate to heavy HIV infection, about 108 to 109 virions are created and removed daily. The HIV average half-life in plasma is about 36 hours, about 24 hours intracellularly, and about 6 hours as an extracellular virus. Every day, roughly 30% of the total HIV burden in an infected individual is turned over. Also, 5 to 7% of CD4 cells turn over daily, and the entire pool of CD4 cells turns over every 2 days (1). Hence, end-stage HIV infection (AIDS) results from a continuous and consistent replication of HIV, leading to the virus and immune-mediated killing of CD4 lymphocytes. Further, the high volume of HIV replication and high frequency of transcription errors by HIV reverse transcriptase result in many mutations, increasing the chance of producing strains resistant to host immunity and drugs.
Infection with another type of retrovirus, human T-lymphotropic virus 1 (HTLV-1), is less common but can also cause serious disease.
Immune system
Two main consequences of HIV infection are
Damage to the immune system, specifically depletion of CD4+ lymphocytes
Immune activation
CD4+ lymphocytes are involved in cell-mediated and, to a lesser extent, humoral immunity. CD4+ depletion may result from the following:
Direct cytotoxic effects of HIV replication
Cell-mediated immune cytotoxicity
Thymic damage that impairs lymphocyte production
Infected CD4+ lymphocytes have a half-life of about 2 days, which is much shorter than that of uninfected CD4+ cells. Rates of CD4+ lymphocyte destruction correlate with plasma HIV level. Typically, during the initial or primary infection, HIV levels are highest (> 106 copies/mL), and the CD4 count drops rapidly.
The normal CD4 count is about 750/mcL, and immunity is minimally affected if the count is > 350/mcL. If the count drops below about 200/mcL, loss of cell-mediated immunity allows a variety of opportunistic pathogens to reactivate from latent states and cause clinical disease.
The humoral immune system is also affected. Hyperplasia of B cells in lymph nodes causes lymphadenopathy, and secretion of antibodies to previously encountered antigens increases, often leading to hyperglobulinemia. Total antibody levels (especially IgG and IgA) and titers against previously encountered antigens may be unusually high. However, antibody response to new antigens (eg, in vaccines) decreases as the CD4 count decreases.
Abnormal elevation of immune activation may be caused in part by absorption of components of bowel bacteria. Immune activation contributes to CD4+ depletion and immunosuppression by mechanisms that remain unclear.
Other tissues
HIV also infects nonlymphoid monocytic cells (eg, dendritic cells in the skin, macrophages, brain microglia) and cells of the brain, genital tract, heart, and kidneys, causing disease in the corresponding organ systems.
HIV strains in several compartments, such as the nervous system (brain and cerebrospinal fluid) and genital tract (semen, cervico-vaginal fluid), can acquire mutations and become genetically distinct from those in plasma, suggesting that they have been selected by or have adapted to these anatomic compartments (2–4). Thus, HIV levels and resistance patterns in these compartments may vary independently from those in plasma.
Disease progression
During the first few weeks of primary infection, there are humoral and cellular immune responses:
Humoral: Antibodies to HIV are usually measurable within a few weeks after primary infection; however, antibodies cannot fully control HIV infection because mutated forms of HIV that are not controlled by the patient’s current anti-HIV antibodies are generated.
Cellular: Cell-mediated immunity is a more important means of controlling the high levels of viremia (usually over 106 copies/mL) at first. But rapid mutation of viral antigens that are targeted by lymphocyte-mediated cytotoxicity subvert control of HIV in all but a small percentage of patients.
Plasma HIV virion levels, expressed as number of HIV RNA copies/mL, stabilize after about 6 months at a level (set point) that varies widely among patients but averages 30,000 to 100,000/mL (4.2 to 5 log10/mL). This variability depends on how host factors interact and impact HIV viral genetic diversity (5). The higher this set point, the more quickly the CD4 count decreases to a level that seriously impairs immunity (< 200/mcL) and results in the opportunistic infections and cancers that define end-stage HIV (6, 7).
Risk and severity of opportunistic infections, end-stage HIV, and AIDS-related cancers are determined by 2 factors:
CD4 count
Exposure to potentially opportunistic pathogens
Risk of specific opportunistic infections increases below threshold CD4 counts of about 200/mcL for some infections and 50/mcL for others, as in the following:
CD4 count < 200/mcL: Increased risk of Pneumocystis jirovecii pneumonia, toxoplasmic encephalitis, and cryptococcal meningitis
CD4 count < 50/mcL: Increased risk of cytomegalovirus (CMV) and Mycobacterium aviuim complex (MAC) infections
For every 3-fold (0.5 log10) increase in plasma HIV RNA in untreated patients, risk of progression to end-stage HIV or death over the next 2 to 3 years increases about 50% (6).
Without treatment, risk of progression to end-stage HIV is about 1 to 2%/year in the first 2 to 3 years of infection and about 5 to 6%/year thereafter. Eventually, end-stage HIV almost invariably develops in untreated patients.
Pathophysiology references
1. Ho DD, Neumann AU, Perelson AS, et al: Rapid turnover of plasma virions and CD4 lymphocytes in HIV-1 infection. Nature 373(6510):123-126, 1995. doi: 10.1038/373123a0
2. Bednar MM, Sturdevant CB, Tompkins LA, et al: Compartmentalization, viral evolution, and viral latency of HIV in the CNS. Curr HIV/AIDS Rep 12(2):262-271, 2015. doi:10.1007/s11904-015-0265-9
3. Mabvakure BM, Lambson BE, Ramdayal K, et al: Evidence for both intermittent and persistent compartmentalization of HIV-1 in the female genital tract. J Virol 93(10):e00311-e00319, 2019. doi:10.1128/JVI.00311-19
4. Ghosn J, Viard JP, Katlama C, et al: Evidence of genotypic resistance diversity of archived and circulating viral strains in blood and semen of pre-treated HIV-infected men. AIDS (London, England). 18(3):447-457, 2004. doi: 10.1097/00002030-200402200-00011
5. Bartha I, McLaren PJ, Brumme C, et al: Estimating the respective contributions of human and viral genetic variation to HIV control. PLoS Comput Biol 13(2):e1005339, 2017. Published 2017 Feb 9. doi:10.1371/journal.pcbi.1005339
6. Lavreys L, Baeten JM, Chohan V, et al: Higher set point plasma viral load and more-severe acute HIV type 1 (HIV-1) illness predict mortality among high-risk HIV-1-infected African women. Clin Infect Dis 42(9):1333-9, 2006. doi: 10.1086/503258
7. Lyles RH, Muñoz A, Yamashita TE, et al: Natural history of human immunodeficiency virus type 1 viremia after seroconversion and proximal to AIDS in a large cohort of homosexual men. Multicenter AIDS cohort study. J Infect Dis 181(3):872-80, 2000. doi: 10.1086/315339
Symptoms and Signs of HIV Infection
Initial HIV infection
Initially, primary HIV infection may be asymptomatic or cause transient nonspecific symptoms (acute retroviral syndrome).


© Springer Science+Business Media


© Springer Science+Business Media
Acute retroviral syndrome usually begins within 1 to 4 weeks of infection and usually lasts 3 to 14 days. Symptoms and signs are often mistaken for infectious mononucleosis or benign, nonspecific viral syndromes and may include fever, malaise, fatigue, several types of dermatitis, sore throat, arthralgias, generalized lymphadenopathy, and septic meningitis.
After the first symptoms disappear, most patients, even without treatment, have no symptoms or only a few mild, intermittent, nonspecific symptoms for a highly variable time period (2 to 15 years).
Symptoms during this relatively asymptomatic period may result from HIV directly or from opportunistic infections. The following are most common:
Lymphadenopathy
White plaques due to oral candidiasis
Herpes zoster
Diarrhea
Fatigue
Fever with intermittent sweats
Asymptomatic, mild-to-moderate cytopenias (eg, leukopenia, anemia, thrombocytopenia) are also common. Some patients experience progressive wasting (which may be related to anorexia and increased catabolism due to infections) and low-grade fevers or diarrhea.
Worsening HIV infection
When the CD4 count drops to < 200/mcL, nonspecific symptoms may worsen and a succession of AIDS-defining illnesses develop.
In patients with HIV infection, certain syndromes are common and may require different considerations (see table ). Some patients present with cancers (eg, Kaposi sarcoma, B-cell lymphomas) that occur more frequently, are unusually severe, or have unique features in patients with HIV infection (see Cancers Common in HIV-Infected Patients). In other patients, neurologic dysfunction may occur.
Evaluation may detect infections that do not typically occur in the general population, such as
Disseminated mycobacterial infections
Pneumocystis jirovecii infection
Cryptococcus neoformans infection
Other fungal infections
Infections that also occur in the general population but suggest advanced HIV infection if they are unusually severe or frequently recur include
Invasive pneumococcal infections
Salmonella septicemia


This patient with HIV has disseminated cutaneous papules on the face as well as exophytic nodules on the eyelids.
This patient with HIV has disseminated cutaneous papules on the face as well as exophytic nodules on the eyelids.
© Springer Science+Business Media


This photo shows diffuse scaling and hyperkeratotic plaques in a patient with HIV and crusted scabies.
This photo shows diffuse scaling and hyperkeratotic plaques in a patient with HIV and crusted scabies.
© Springer Science+Business Media


AIDS-associated Kaposi sarcoma is an aggressive, multicentric tumor that may involve the face, trunk, mucosal surfaces, lymphatics, or gastrointestinal tract. Lesions appear as bluish to violaceous macules, plaques, or tumors.
AIDS-associated Kaposi sarcoma is an aggressive, multicentric tumor that may involve the face, trunk, mucosal surfaces,
Photo courtesy of Sol Silverman, Jr., via the Public Health Image Library of the Centers for Disease Control and Prevention.

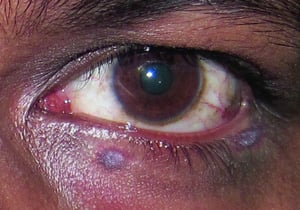
This photo shows purplish red nodules consistent with Kaposi sarcoma over the lower eyelid skin in a patient with HIV infection.
This photo shows purplish red nodules consistent with Kaposi sarcoma over the lower eyelid skin in a patient with HIV i
© Springer Science+Business Media


This photo shows Kaposi sarcoma on the face, ear, and neck.
This photo shows Kaposi sarcoma on the face, ear, and neck.
© Springer Science+Business Media


This photo shows disseminated oval plaques of Kaposi sarcoma on the shoulders of a patient with HIV infection.
This photo shows disseminated oval plaques of Kaposi sarcoma on the shoulders of a patient with HIV infection.
© Springer Science+Business Media


This photo shows violaceous plaques on the forearm in a patient with HIV infection.
This photo shows violaceous plaques on the forearm in a patient with HIV infection.
© Springer Science+Business Media

Oral hairy leukoplakia appears as verrucous white outgrowths on the lateral margins of the tongue.
Oral hairy leukoplakia appears as verrucous white outgrowths on the lateral margins of the tongue.
Image courtesy of J.S. Greenspan, BDS, University of California, San Francisco and Sol Silverman, Jr., DDS via the Public Health Image Library of the Centers for Disease Control and Prevention.


This photo shows condylomata (1) and squamous cell invasive cancer (2) caused by persistent human papillomavirus (HPV) infection in a person with HIV infection.
This photo shows condylomata (1) and squamous cell invasive cancer (2) caused by persistent human papillomavirus (HPV)
Image courtesy of Dr. Edward R. Cachay.
This patient with HIV has disseminated cutaneous papules on the face as well as exophytic nodules on the eyelids.
This patient with HIV has disseminated cutaneous papules on the face as well as exophytic nodules on the eyelids.
© Springer Science+Business Media
This photo shows diffuse scaling and hyperkeratotic plaques in a patient with HIV and crusted scabies.
This photo shows diffuse scaling and hyperkeratotic plaques in a patient with HIV and crusted scabies.
© Springer Science+Business Media
AIDS-associated Kaposi sarcoma is an aggressive, multicentric tumor that may involve the face, trunk, mucosal surfaces, lymphatics, or gastrointestinal tract. Lesions appear as bluish to violaceous macules, plaques, or tumors.
AIDS-associated Kaposi sarcoma is an aggressive, multicentric tumor that may involve the face, trunk, mucosal surfaces,
Photo courtesy of Sol Silverman, Jr., via the Public Health Image Library of the Centers for Disease Control and Prevention.
This photo shows purplish red nodules consistent with Kaposi sarcoma over the lower eyelid skin in a patient with HIV infection.
This photo shows purplish red nodules consistent with Kaposi sarcoma over the lower eyelid skin in a patient with HIV i
© Springer Science+Business Media
This photo shows Kaposi sarcoma on the face, ear, and neck.
This photo shows Kaposi sarcoma on the face, ear, and neck.
© Springer Science+Business Media
This photo shows disseminated oval plaques of Kaposi sarcoma on the shoulders of a patient with HIV infection.
This photo shows disseminated oval plaques of Kaposi sarcoma on the shoulders of a patient with HIV infection.
© Springer Science+Business Media
This photo shows violaceous plaques on the forearm in a patient with HIV infection.
This photo shows violaceous plaques on the forearm in a patient with HIV infection.
© Springer Science+Business Media
Oral hairy leukoplakia appears as verrucous white outgrowths on the lateral margins of the tongue.
Oral hairy leukoplakia appears as verrucous white outgrowths on the lateral margins of the tongue.
Image courtesy of J.S. Greenspan, BDS, University of California, San Francisco and Sol Silverman, Jr., DDS via the Public Health Image Library of the Centers for Disease Control and Prevention.
This photo shows condylomata (1) and squamous cell invasive cancer (2) caused by persistent human papillomavirus (HPV) infection in a person with HIV infection.
This photo shows condylomata (1) and squamous cell invasive cancer (2) caused by persistent human papillomavirus (HPV)
Image courtesy of Dr. Edward R. Cachay.
Common Manifestations Associated With HIV Infection by Organ System
Syndrome | Cause | Diagnostic Evaluation | Treatment* | Symptoms/Comments |
|---|---|---|---|---|
Cardiac | ||||
Direct viral damage to cardiac myocytes | Echocardiography | Antiretroviral drugs | Symptoms of heart failure | |
Gastrointestinal | ||||
Candidiasis, CMV, or herpes simplex virus | Esophagoscopy with biopsy of ulcers | Treatment of cause with antiviral and antimicrobial drugs | Dysphagia, anorexia | |
Gastroenteritis or colitis | Intestinal Salmonella, MAC, Cryptosporidium (cryptosporidiosis), Cyclospora (cyclosporiasis), CMV, microsporidia, Cystoisospora (Isospora) belli (cystoisosporiasis), or Clostridioides difficile | Cultures and stains of stools or biopsy, but determination of cause possibly difficult | Treatment of cause:
| Diarrhea, weight loss, abdominal cramping |
CMV, Cryptosporidium, Cyclospora, or microsporidia | Ultrasonography or endoscopy | Antimicrobial drugs for Cryptosporidium, Cyclospora, and microsporidia | Possibly pain or obstruction | |
Rectal and perirectal lesions | Proctitis caused by Neisseria gonorrhoeae or Chlamydia trachomatis (particularly LGV), HSV, syphilis | Examination Gram staining and culture Nucleic acid amplification testing (NAAT) RPR/treponemal antibody test Biopsy | Treatment of cause | High incidence in women and men who have sex with men via anal receptive sexual intercourse† |
Hepatocellular damage due to hepatitis viruses, opportunistic infections, or antiviral drug toxicity | TB, MAC, CMV, or peliosis (bartonellosis), chronic hepatitis B or chronic hepatitis C, which may be worsened by HIV | Differentiation from hepatitis due to antiretroviral or other drugs Liver biopsy sometimes necessary | Treatment of cause | Symptoms of hepatitis (eg, anorexia, nausea, vomiting, jaundice) |
Genital/Reproductive Tract | ||||
Anal and external genital lesions | Herpes simplex virus (HSV) Genital warts or anal or cervical cancer induced by HPV | Examination Gram staining and culture Nucleic acid amplification testing (NAAT) Biopsy | Treatment of cause | High incidence in women and men who have sex with men via anal receptive sexual intercourse† |
Pelvic inflammatory disease | Neisseria gonorrhoeae, Chlamydia trachomatis, or other usual pathogens | Possibly increased in severity, atypical presentation, and more difficult to treat in women with HIV | ||
Vaginal candidiasis | Candida spp. | Possibly increased in severity or recurrence in women with HIV | ||
Hematologic | ||||
Anemia | Multifactorial: HIV-induced bone marrow suppression Immune-mediated peripheral destruction Anemia of chronic disease Infections, particularly human parvovirus B-19, disseminated MAC, or histoplasmosis Cancers | For parvovirus B19 infection, bone marrow examination (to check for multinucleated erythroblasts) or serum or bone marrow PCR | Treatment of cause Transfusion as needed Erythropoietin for anemia due to antineoplastic drugs or zidovudine if severity warrants transfusion and erythropoietin level is Erythropoietin for anemia due to antineoplastic drugs or zidovudine if severity warrants transfusion and erythropoietin level is< 500 mU/L IVIG for parvovirus | With parvovirus, sometimes acute severe anemia |
Immune thrombocytopenia, drug toxicity, HIV-induced bone marrow suppression, immune-mediated peripheral destruction, infections, or cancer | CBC, clotting tests, PTT, peripheral smear, bone marrow biopsy, or von Willebrand factor measurementCBC, clotting tests, PTT, peripheral smear, bone marrow biopsy, or von Willebrand factor measurement | Antiretroviral drugs IVIG for bleeding or preoperatively Possibly anti-Rho (D) IgG, vincristine, danazol, or interferonPossibly anti-Rho (D) IgG, vincristine, danazol, or interferon If severe and intractable, splenectomy | Often asymptomatic and may occur in otherwise asymptomatic HIV infection | |
HIV-induced bone marrow suppression, immune-mediated peripheral destruction, infections, cancer, or drug toxicity | For severe neutropenia (< 500/mcL) plus fever, immediate broad-spectrum antibiotics If drug-induced, granulocyte or granulocyte-macrophage colony-stimulating factors | — | ||
Neurologic | ||||
Mild to severe cognitive impairment with or without motor deficits | Direct virus-induced brain damage | HIV RNA level in CSF CT or MRI to check for brain atrophy (nonspecific) | Antiretroviral drugs, which may reverse damage and improve function, although low levels of cognitive dysfunction commonly persist, even in treated patients | Progression to dementia uncommon in treated patients |
Ascending paralysis | Guillain-Barré syndrome or CMV polyradiculopathy | Spinal cord MRI CSF testing | Treatment of CMV polyradiculopathy Supportive care for Guillain-Barré syndrome | Neutrophilic pleocytosis in patients with CMV polyradiculopathy, possibly simulating bacterial meningitis |
Acute or subacute focal encephalitis | Toxoplasma gondii (toxoplasmosis) | CT or MRI to check for ring-enhancing lesions, especially in basal ganglia Antibody testing of CSF (sensitive but not specific) PCR testing to check for T. gondii DNA in CSF Brain biopsy (rarely indicated) | Pyrimethamine, folinic acid, sulfadiazine, and possibly sulfamethoxazole/trimethoprim, SMX-TMP, Cotrimoxazole (clindamycin if allergic to sulfa—see Pyrimethamine, folinic acid, sulfadiazine, and possibly sulfamethoxazole/trimethoprim, SMX-TMP, Cotrimoxazole (clindamycin if allergic to sulfa—seeToxoplasmosis: Treatment of patients with AIDS or other immunocompromising conditions) Often lifelong maintenance therapy | Primary prophylaxis with clindamycin and pyrimethamine or sulfamethoxazole/trimethoprim, SMX-TMP, Cotrimoxazole (as for Primary prophylaxis with clindamycin and pyrimethamine or sulfamethoxazole/trimethoprim, SMX-TMP, Cotrimoxazole (as forPneumocystis pneumonia) indicated for patients with a CD4 count of < 100/mcL and previous toxoplasmosis or positive antibodies; can be stopped if CD4 counts increase to > 200/mcL for ≥ 3 months in response to antiretroviral therapy |
Subacute encephalitis | Less often, herpes simplex virus or varicella-zoster virus | CSF PCR Response to treatment | Antiviral drugs | With CMV, often delirium, cranial nerve palsies, myoclonus, seizures, and progressively impaired consciousness at presentation Often responds rapidly to treatment |
Myelitis or polyradiculopathy | CMV | Spinal cord MRI CSF PCR | Antiviral drugs | Simulates Guillain-Barré syndrome |
Progressive encephalitis of white matter only | Progressive multifocal leukoencephalopathy due to reactivation of latent JC virus infection HIV | Brain MRI CSF testing | Antiretroviral drugs to reverse the immunodeficiency (no drugs are effective for JC virus) | Usually fatal within a few months May respond to antiretroviral drugs |
Coccidioidomycosis, Cryptococcus (cryptococcosis), Histoplasma (histoplasmosis), or Mycobacterium tuberculosis | CT or MRI CSF stains, antigen tests, PCR, and cultures | Treatment of cause | Outcomes improved by early treatment | |
Direct effects of HIV or CMV or antiviral drug toxicity | History Sensory and motor testing | Treatment of cause or withdrawal of toxic drugs | Very common Not quickly reversible | |
Ophthalmologic | ||||
Retinitis | CMV or VZV | Direct retinoscopy | Specific anti-CMV or anti-VZV drugs | Requires examination by specialist VZV causes acute retinal necrosis in some patients with end-stage HIV |
Oral | ||||
Oral candidiasis | Immunosuppression by HIV | Examination | Systemic antifungals | Possibly painless in early stages |
Mpox (formerly monkeypox) virus | Examination PCR of fluid from vesicles | Antiviral drugs | Painful, vesicular rash can begin in mouth then spread High incidence in men who have sex with men† | |
Intraoral ulcers | Herpes simplex virus or aphthous stomatitis | For aphthous ulcers, intralesional or systemic corticosteroids and systemic montelukast and thalidomide, intralesional or systemic corticosteroids and systemic montelukast and thalidomide For herpes, acyclovirFor herpes, acyclovir | May be severe and result in undernutrition | |
Mixed oral bacterial flora | Examination | Improved hygiene and nutrition Antibiotics | May be severe, with bleeding, swelling, and tooth loss | |
Painless intraoral mass | Kaposi sarcoma, lymphoma, or tumors induced by HPV | Biopsy | Treatment of neoplasm | — |
Painless white filiform patches on the sides of the tongue (oral hairy leukoplakia) | Examination | AcyclovirAcyclovir | Usually asymptomatic | |
Pulmonary | ||||
Subacute (occasionally acute) pneumonia | Mycobacteria Fungi such as P. jirovecii, C. neoformans, H. capsulatum, Coccidioides immitis, or Aspergillosis | Pulse oximetry Chest x-ray Skin tests (sometimes false-negative because of anergy) Bronchoscopy with special stains and cultures of bronchial lavage specimens sometimes necessary | Treatment of cause | Possibly cough, tachypnea, and chest discomfort at presentation Mild hypoxia or increased alveolar-arterial oxygen gradient possibly occurring before evidence of pneumonia on x-ray |
Acute (occasionally subacute) pneumonia | Typical bacterial pathogens or Haemophilus, Pseudomonas, Nocardia, or Rhodococcus | In patients with known or suspected HIV and pneumonia, exclusion of opportunistic or unusual pathogens | Treatment of cause | Possibly cough, tachypnea, and chest discomfort at presentation |
Tracheobronchitis | Candida spp. or herpes simplex virus (HSV) | — | Treatment of cause | Possibly cough, tachypnea, and chest discomfort at presentation |
Subacute or chronic pneumonia or mediastinal adenopathy | Kaposi sarcoma or B-cell lymphoma | Chest CT Bronchoscopy | Treatment of cause | Possibly cough, tachypnea, and chest discomfort at presentation |
Renal | ||||
Nephrotic syndrome or renal insufficiency | Direct viral damage, resulting in focal glomerulosclerosis | Renal biopsy | Antiretroviral drugs or ACE inhibitors possibly useful | Increased incidence in African Americans and patients with a low CD4 count |
Tubular dysfunction (glucosuria, proteinuria) | Some antiviral drugs | Urinalysis and/or blood tests | Dose reduction or discontinuation of the antiviral drug | — |
Skin | ||||
Varicella-zoster virus (VZV) | PCR-based testing DNA testing on scrapings from vesicular skin lesions that have not yet crusted Culture (best if done on unroofed and recently ruptured vesicles) | Acyclovir or related drugsAcyclovir or related drugs | Common Possible prodrome of mild to severe pain or tingling before skin lesions PCR-based testing is most sensitive | |
Herpes simplex ulcers | PCR-based testing of ulcer HSV culture of ulcer | Antiviral drugs if lesions are severe, extensive, persistent, or disseminated | Atypical lesions of herpes simplex are extensive, severe, or persistent PCR-based testing is most sensitive | |
Sarcoptes scabiei | Clinical evaluation and scrapings | Possibly severe hyperkeratotic lesions | ||
Vesicular painful rash | Examination PCR of fluid from vesicles, pustules, and/or dry crusts | Antiviral drugs | Rash can spread Lymphadenopathy is common | |
Violaceous or red papules or nodules | Kaposi sarcoma or bartonellosis | Biopsy | Antiretroviral drugs and treatment of cause | — |
Centrally umbilicated skin lesions | Cryptococcosis or molluscum contagiosum | See Molluscum contagiosum: Diagnosis and Cryptococcosis: Diagnosis | May be the presenting sign of cryptococcemia | |
Systemic | ||||
Sepsis and septic shock due to nosocomial gram-negative bacillary and staphylococcal infections, disseminated opportunistic infections | Gram-negative bacilli, Staphylococcus aureus, Candida spp., Salmonella, M. tuberculosis, MAC, or H. capsulatum | Blood cultures Bone marrow examination | Treatment of cause | — |
Wasting syndrome (substantial weight loss) | Multifactorial, including AIDS, AIDS-related opportunistic infections, AIDS-related cancers, and/or AIDS-induced hypogonadism | Defined as weight loss of > 10% of body weight | Antiretroviral drugs (the primary treatment for this syndrome) Treatment of underlying infections; treatment of AIDS-induced hypogonadism when indicated Measures to improve appetite and caloric intake | — |
CBC = complete blood count; CMV = cytomegalovirus; CSF = cerebrospinal fluid; HPV = human papillomavirus; HSV = herpes simplex virus; IVIG = IV immune globulin; MAC = Mycobacterium avium complex; Mpox = monkeypox; PCR = polymerase chain reaction; PTT = partial thromboplastin time; TMP/SMX = trimethoprim/sulfamethoxazole/; TB partial thromboplastin time; TMP/SMX = trimethoprim/sulfamethoxazole/; TB= tuberculosis; VZV =varicella-zoster virus | ||||
* Antiretroviral drugs are always part of the treatment plan. They are listed in this treatment section only when there is no more specific treatment. † These diagnoses are surrogates of behaviors that increase the risk of HIV infection; when present, these diagnoses should prompt HIV testing. | ||||
Acquired immune deficiency syndrome (AIDS)
AIDS is defined as HIV infection with one or more of the following:
One or more AIDS-defining illnesses (1)
A CD4+ T lymphocyte (helper cell) count of < 200/mcL
A CD4+ cell percentage of ≤ 14% of the total lymphocyte count
AIDS-defining illnesses include
Serious opportunistic infections
Certain cancers (eg, Kaposi sarcoma, non-Hodgkin lymphoma) to which defective cell-mediated immunity predisposes
Neurologic dysfunction
Wasting syndrome
AIDS-Defining Illnesses
|
See also Centers for Disease Control and Prevention Morbidity and Mortality Weekly Report (MMWR): Revised Surveillance Case Definition for HIV Infection, United States, 2014. * Only among children aged < 6 years † Only among adults, adolescents, and children aged ≥ 6 years |


Image courtesy of Dr. Edward R. Cachay.
Symptoms and signs reference
1. Selik RM, Mokotoff ED, Branson, B, et al: Revised Surveillance Case Definition for HIV Infection—United States, 2014. MMWR63(RR03):1–10, 2014.
Diagnosis of HIV Infection
HIV antibody testing with or without HIV P24 antigen tests
Nucleic acid amplification assays to determine HIV RNA level (viral load)
HIV infection is suspected in patients with persistent, unexplained, generalized adenopathy or any of the AIDS-defining illnesses (see sidebar ). It may also be suspected in high-risk patients with symptoms that could represent acute primary HIV infection.
Diagnostic tests
Detection of antibodies to HIV is sensitive and specific except during the first few weeks after infection (termed the "window period" of acute HIV infection). However, the HIV p24 antigen (a core protein of the virus) is already present in the blood during most of this time and can be detected by assays.
Currently, a fourth-generation antigen/antibody combination immunoassay is recommended; it detects antibodies to both HIV-1 and HIV-2 as well as the p24 HIV antigen. The laboratory version is probably preferred over the point-of-care test for diagnosing early infection, but both can be done quickly (within 30 minutes). If the test result is positive, an assay to differentiate HIV-1 and HIV-2 and an HIV RNA assay are done.
Earlier-generation enzyme-linked immunosorbent assay (ELISA) antibody assays are highly sensitive, but because they do not test for antigen, they are not positive as early as the fourth-generation combination test. Also, results are rarely false-positive. Positive ELISA results are therefore confirmed with a more specific test such as Western blot. However, these tests have drawbacks:
ELISA requires complex equipment.
Western blot requires well-trained technicians, is expensive, and takes several days or weeks for results to be available.
The full testing sequence takes at least a day.
Most settings use an HIV-1/HIV-2 differentiation assay as their preferred confirmatory test, replacing the cumbersome Western blot. Additionally, HIV-1 Western blot assays do not reliably detect subtype O virus prevalent in some African regions; if HIV-2 is being considered, a special HIV-2 Western blot needs to be requested (1). Point-of-care tests using blood or saliva (eg, particle agglutination, immunoconcentration, immunochromatography) can be done quickly (in 15 minutes) and simply, allowing testing in a variety of settings and immediate reporting to patients. Positive results of these rapid tests should be confirmed by standard blood tests (eg, ELISA with or without Western blot) in high-resource countries and repetition with one or more other rapid tests in high HIV burden countries. Negative tests need not be confirmed.
If HIV infection is suspected despite negative antibody test results (eg, during the first few weeks after infection), the plasma HIV RNA level should be measured. The nucleic acid amplification assays used are highly sensitive and specific. HIV RNA assays require advanced technology, such as reverse transcription–polymerase chain reaction (RT-PCR), which is sensitive to extremely low HIV RNA levels. Measuring p24 HIV antigen by ELISA is less sensitive and less specific than directly detecting HIV RNA in blood.
Staging
HIV infection can be staged based on the CD4 count. In patients ≥ 6 years old, stages are as follows:
Stage 1: ≥ 500 cells/mcL
Stage 2: 200 to 499 cells/mcL
Stage 3: < 200 cells/mcL
The CD4 count after 1 to 2 years of treatment provides an indication of ultimate immune recovery; CD4 counts may not return to the normal range despite prolonged suppression of HIV.
Monitoring
When HIV is diagnosed, the following should be determined:
CD4 count
Plasma HIV RNA level
Both are useful for determining prognosis and monitoring treatment.
The CD4 count is calculated as the product of the following:
White blood cell count (eg, 4000 cells/mcL)
Percentage of white blood cells that are lymphocytes (eg, 30%)
Percentage of lymphocytes that are CD4+ (eg, 20%)
Using the numbers above, the CD4 count (4000 × 0.3 × 0.2) is 240 cells/mcL, or about 1/3 of the normal CD4 count in adults, which is about 750 ± 250/mcL.
Plasma HIV RNA level (viral load) reflects HIV replication rates. The higher the set point (the relatively stable virus levels that occur after primary infection), the more quickly the CD4 count decreases and the greater the risk of opportunistic infection, even in patients without symptoms.
A baseline HIV genotype (blood test) can be ordered if the HIV viral load is > 500 copies/mL; availability of this testing varies by location. HIV genotyping is used to identify mutations known to cause resistance to certain antiretroviral drugs and to help select a drug regimen likely to be effective for a specific patient with HIV infection.
Diagnosis of HIV-related conditions
Diagnosis of the various opportunistic infections, cancers, and other syndromes that occur in patients with HIV infection is discussed elsewhere in THE MANUAL. Many have aspects unique to HIV infection.
Hematologic disorders (eg, cytopenias, lymphomas, cancers) are common and may be usefully evaluated with bone marrow aspiration and biopsy. This procedure can also help diagnose disseminated infections with MAC (Mycobacterium avium complex), M. tuberculosis, Cryptococcus, Histoplasma, human parvovirus B19, P. jirovecii, and Leishmania. Most patients have normocellular or hypercellular marrow despite peripheral cytopenia, reflecting peripheral destruction. Iron stores are usually normal or increased, reflecting anemia of chronic disease (an iron-reutilization defect). Mild to moderate plasmacytosis, lymphoid aggregates, increased numbers of histiocytes, and dysplastic changes in hematopoietic cells are common.
HIV-associated neurologic syndromes can be differentiated via lumbar puncture with cerebrospinal fluid analysis and central nervous system contrast-enhanced CT or MRI (see table ).
Diagnosis reference
1. Centers for Disease Control and Prevention (CDC): Identification of HIV-1 group O infection—Los Angeles county, California, MMWR Morb Mortal Wkly Rep 45(26):561-565, 1996.
Screening for HIV
Screening antibody tests or newer combination antigen/antibody tests should be offered routinely to adults and adolescents, particularly pregnant women early in each pregnancy, regardless of their perceived risk. For people at highest risk, especially sexually active people who have multiple sex partners and who do not practice safe sex, testing should be repeated every 6 to 12 months. Such testing is confidential and available, often free of charge, in many public and private facilities throughout the world.
Rapid tests have the advantage of offering preliminary test results at the initial encounter in less than 25 minutes. They are especially useful for people who are unlikely to return for their test results. People receiving HIV testing should also be provided information on prevention, care, and treatment services.
In the United States, screening for HIV infection is recommended in all adolescents and adults aged 13 to 64 years and in younger adolescents and older adults who are at increased risk of infection (see Centers for Disease Control and Prevention: Screening for HIV). Screening is also recommended in all pregnant persons, including those who present in labor or at delivery whose HIV status is unknown.
The World Health Organization suggests that, in settings with a high HIV burden, HIV testing be done using rapid antibody tests and enzyme immunoassays (see Consolidated Guidelines on HIV Testing services, July 2019).
Treatment of HIV Infection
Combinations of antiretroviral medications (antiretroviral therapy [ART], sometimes called highly active ART [HAART] or combined ART [cART])
Chemoprophylaxis for opportunistic infections in patients at high risk
(See also Antiretroviral Treatment of HIV Infection.)
Treatment with ART is recommended for all patients, because disease-related complications can occur even in untreated patients with high CD4 counts and because the toxicity of antiretrovirals has decreased as new medications have been developed.
The benefits of ART outweigh the risks in every patient group and setting that has been carefully studied. In the Strategic Timing of AntiRetroviral Treatment (START) study, 5472 treatment-naïve patients with HIV infection and CD4 counts > 350 cells/mcL were randomized to start ART immediately (immediate initiation) or to defer ART until their CD4 count decreased to < 250 cells/mcL (deferred initiation). Risk of AIDS-related events (eg, tuberculosis, Kaposi sarcoma, malignant lymphomas) and non-AIDS–related events (eg, non-AIDS cancer, cardiovascular disease) was lower in the immediate-initiation group (1).
A few exceptional patients can control their HIV strain without treatment; they maintain normal CD4 counts and very low blood levels of HIV (long-term nonprogressors) or normal CD4 counts and undetectable blood levels of HIV (elite controllers). These patients may not require ART, but studies to determine whether treating them is helpful have not been done and would be difficult because there are few of these patients and they would likely do well not taking ART for long periods.
Antiretroviral therapy: General principles
ART aims to
Reduce the plasma HIV RNA level to undetectable (ie, < 20 to 50 copies/mL)
Restore the CD4 count to a normal level (immune restoration or reconstitution)
A poor CD4 count response is more likely if the CD4 count at initiation of treatment is low (especially if < 50/mcL) and/or the HIV RNA level is high. However, marked improvement is likely even in patients with advanced immunosuppression.
An increased CD4 count correlates with markedly decreased risk of opportunistic infections, other complications, and death. With immune restoration, patients, even those with complications that have no specific treatment (eg, HIV-induced cognitive dysfunction) or that were previously considered untreatable (eg, progressive multifocal leukoencephalopathy), may improve. Outcomes are also improved for patients with cancers (eg, lymphoma, Kaposi sarcoma) and most opportunistic infections.
Patients with most acute opportunistic infections benefit from early ART (initiated during the management of the opportunistic infection). However, for some opportunistic infections, such as tuberculous meningitis or cryptococcal meningitis, the evidence suggests that ART should be delayed (2 to 4 weeks in most cases) until the first phase of antimicrobial therapy for these infections is finished because of the increased frequency of adverse events and death.
Almost everyone who takes HIV medicine as prescribed can reach the goals of ART therapy usually within 6 months after starting treatment (Viral Suppression and an Undetectable Viral Load). However, maintaining this degree of adherence is difficult. Partial suppression (failure to lower plasma HIV RNA levels to undetectable levels) may select for single or multiple accumulated mutations in HIV that make viruses partially or completely resistant to a single drug or entire classes of drugs. Unless subsequent treatment uses drugs of other classes to which HIV remains sensitive, treatment is more likely to fail.
The success of ART is assessed by measuring plasma HIV RNA levels every 8 to 12 weeks for the first 4 to 6 months or until HIV levels are undetectable and every 6 months thereafter. Increasing HIV levels are the earliest evidence of treatment failure and may precede a decreasing CD4 count by months. Maintaining patients on failing medication regimens selects for HIV mutants that are more drug-resistant. However, compared with wild-type HIV, these mutants appear less able to reduce the CD4 count, and failing medication regimens are often continued when no fully suppressive regimen can be found.
If treatment fails, drug susceptibility (resistance) assays can determine the susceptibility of the dominant HIV strain to all available medications. Genotypic and phenotypic assays are available and can help clinicians select a new regimen that should contain at least 2 and preferably 3 medications to which the HIV strain is more susceptible. The dominant HIV strain in the blood of patients who are taken off antiretroviral therapy may revert over months to years to the wild-type (ie, susceptible) strain because the resistant mutants replicate more slowly and are replaced by the wild type. Thus, if patients have not been treated recently, the full extent of resistance may not be apparent through resistance testing, but when treatment resumes, strains with resistance mutations often reemerge from latency and again replace the wild-type HIV strain.
Many patients with HIV infection are taking complex regimens involving multiple pills to control the HIV RNA level (viral load), but often, no conventional HIV RNA resistance tests were done when viral treatment failed. With the availability of new co-formulated HIV medications, many patients could benefit from simplification of their ART regimen, guided by HIV DNA archive genotype testing (GenoSure Archive). The HIV DNA genotype archive provides HIV-1 antiretroviral drug resistance data when conventional HIV RNA resistance testing cannot be done because patients have a low plasma HIV RNA level (< 500 copies/mL). The HIV DNA archive genotype test analyzes integrated and unintegrated archived HIV-1 proviral DNA embedded in host cells. The test amplifies cell-associated HIV-1 DNA from infected cells in whole blood samples, then uses next-generation sequencing technology to analyze the HIV-1 polymerase region. The positive predictive value of the HIV DNA archive resistance test results may enable clinicians to identify HIV-resistance mutations that were previously unidentified and to select a potentially simpler regimen with co-formulated drugs (≥ 2 drugs in a single pill).
Immune reconstitution inflammatory syndrome (IRIS)
Patients beginning ART sometimes deteriorate clinically, even though HIV levels in their blood are suppressed and their CD4 count increases, because of an immune reaction to subclinical opportunistic infections or to residual microbial antigens after successful treatment of opportunistic infections. IRIS usually occurs in the first months of HIV treatment but is occasionally delayed. IRIS can complicate virtually any opportunistic infection and even tumors (eg, Kaposi sarcoma) but is usually self-limited or responds to brief regimens of corticosteroids.
IRIS has 2 forms:
Paradoxical IRIS, which refers to worsening symptoms due to a previously diagnosed infection
Unmasked IRIS, which refers to the first appearance of symptoms of an infection not previously diagnosed
Paradoxical IRIS typically occurs during the first few months of HIV treatment and usually resolves on its own. If it does not, corticosteroids, given for a short time, are often effective. Paradoxical IRIS is more likely to cause symptoms and symptoms are more likely to be severe when ART is started soon after treatment of an opportunistic infection is started. Thus, for some opportunistic infections, ART is delayed until treatment of the opportunistic infection has reduced or eliminated the infection.
In patients with unmasked IRIS, the newly identified opportunistic infection is treated with antimicrobial drugs. Occasionally, when the symptoms are severe, corticosteroids are also used. Usually, when unmasked IRIS occurs, ART is continued. An exception is cryptococcal meningitis. Then ART is temporarily interrupted until the infection is controlled.
Determining whether clinical deterioration is caused by treatment failure, IRIS, or both requires assessment of the persistence of active infections with cultures and can be difficult.
Interruption of antiretroviral therapy
Interruption of ART is usually safe if all drugs are stopped simultaneously, but levels of slowly metabolized medications (eg, nevirapine, efavirenz) may remain high and thus increase the risk of resistance. Interruption may be necessary if intervening illnesses require treatment or if medication toxicity is intolerable or needs to be evaluated. After interruption to determine which drug is responsible for toxicity, clinicians can safely restart most medications as monotherapy for up to a few days. NOTE: The most important exception is abacavir; patients who had fever or rash during previous exposure to abacavir may develop severe, potentially fatal hypersensitivity reactions with reexposure. Risk of an adverse reaction to abacavir is 100-fold higher in patients with HLA-B*57:01, which can be detected by genetic testing.Interruption of ART is usually safe if all drugs are stopped simultaneously, but levels of slowly metabolized medications (eg, nevirapine, efavirenz) may remain high and thus increase the risk of resistance. Interruption may be necessary if intervening illnesses require treatment or if medication toxicity is intolerable or needs to be evaluated. After interruption to determine which drug is responsible for toxicity, clinicians can safely restart most medications as monotherapy for up to a few days. NOTE: The most important exception is abacavir; patients who had fever or rash during previous exposure to abacavir may develop severe, potentially fatal hypersensitivity reactions with reexposure. Risk of an adverse reaction to abacavir is 100-fold higher in patients with HLA-B*57:01, which can be detected by genetic testing.
Pearls & Pitfalls
|
Prevention of opportunistic infections
(See also the United States Public Health Service and the HIV Medicine Association of the Infectious Diseases Society of America’s Guidelines for the Prevention and Treatment of Opportunistic Infections in Adults and Adolescents With HIV.)
Effective chemoprophylaxis is available for many opportunistic infections and reduces rates of disease due to P. jirovecii, Candida, Cryptococcus, and MAC (Mycobacterium avium complex). If therapy restores CD4 counts to above threshold values for > 3 months, chemoprophylaxis can be stopped.
Primary prophylaxis depends on the CD4 count:
CD4 count < 200/mcL or oropharyngeal candidiasis (active or previous): Prophylaxis against P. jirovecii pneumonia is recommended. Double-strength sulfamethoxazole/trimethoprim, SMX-TMP, Cotrimoxazole tablets given once/day or 3 times/week are effective. Some adverse effects can be minimized with the 3 times/week dose or by gradual dose escalation. Some patients who cannot tolerate TMP/SMX can tolerate dapsone (100 mg once/day). Patients with glucose-6-phosphate dehydrogenase (pneumonia is recommended. Double-strength sulfamethoxazole/trimethoprim, SMX-TMP, Cotrimoxazole tablets given once/day or 3 times/week are effective. Some adverse effects can be minimized with the 3 times/week dose or by gradual dose escalation. Some patients who cannot tolerate TMP/SMX can tolerate dapsone (100 mg once/day). Patients with glucose-6-phosphate dehydrogenase (G6PD) deficiency are at risk for developing severe hemolysis with dapsone use and, therefore, should be screened for G6PD deficiency before using dapsone. For the few patients who cannot tolerate either drug because of a troublesome adverse effect (eg, fever, neutropenia, rash), aerosolized pentamidine 300 mg once/month or atovaquone 1500 mg once/day can be used.) deficiency are at risk for developing severe hemolysis with dapsone use and, therefore, should be screened for G6PD deficiency before using dapsone. For the few patients who cannot tolerate either drug because of a troublesome adverse effect (eg, fever, neutropenia, rash), aerosolized pentamidine 300 mg once/month or atovaquone 1500 mg once/day can be used.
CD4 count < 50/mcL: Primary prophylaxis against disseminated MAC disease is not recommended for adults and adolescents with HIV who immediately initiate ART. People with HIV who are not receiving ART or who remain viremic on ART but have no current options for a fully suppressive ART regimen should receive chemoprophylaxis against disseminated MAC disease if they have CD4 counts <50 cells/mm3 (2). Prophylaxis against disseminated MAC consists of azithromycin or clarithromycin; if neither of these drugs is tolerated, rifabutin can be used. Azithromycin can be given weekly as two 600-mg tablets; it provides protection (70%) similar to daily clarithromycin and does not interact with other medications.). Prophylaxis against disseminated MAC consists of azithromycin or clarithromycin; if neither of these drugs is tolerated, rifabutin can be used. Azithromycin can be given weekly as two 600-mg tablets; it provides protection (70%) similar to daily clarithromycin and does not interact with other medications.
If latent tuberculosis is suspected (based on tuberculin skin tests, interferon-gamma release assays, high-risk exposure, personal history of active tuberculosis, or residence in a region with high tuberculosis prevalence), regardless of CD4 count, patients should be given isoniazid 5 mg/kg (up to 300 mg) orally once/day plus pyridoxine (vitamin B6) 10 to 25 mg orally once/day for 9 months to prevent reactivation. is suspected (based on tuberculin skin tests, interferon-gamma release assays, high-risk exposure, personal history of active tuberculosis, or residence in a region with high tuberculosis prevalence), regardless of CD4 count, patients should be given isoniazid 5 mg/kg (up to 300 mg) orally once/day plus pyridoxine (vitamin B6) 10 to 25 mg orally once/day for 9 months to prevent reactivation.
For primary prophylaxis against some fungal infections (eg, esophageal candidiasis), oral fluconazole 100 to 200 mg once/day is successful but is infrequently used because the cost per infection prevented is high and diagnosis and treatment of these infections are usually successful (For primary prophylaxis against some fungal infections (eg, esophageal candidiasis), oral fluconazole 100 to 200 mg once/day is successful but is infrequently used because the cost per infection prevented is high and diagnosis and treatment of these infections are usually successful (3).
Secondary prophylaxis (after control of the initial infection) is indicated if patients have had the following:
Recurrent oral, vaginal, or esophageal candidiasis; coccidioidomycosis; or cryptococcal infections: Fluconazole is used.: Fluconazole is used.
Histoplasmosis: Itraconazole is used.: Itraconazole is used.
Latent toxoplasmosis: This asymptomatic condition is indicated by serum antibodies (IgG) to Toxoplasma gondii. TMP/SMX (in doses used to prevent P. jirovecii pneumonia) is used to prevent reactivation and consequent toxoplasmic encephalitis. Latent infection is less common (about 15% of adults) in the United States than in Europe and most high HIV burden countries (up to 70 to 80% of adults).
Aspergillosis (possibly)
Detailed guidelines for prophylaxis of fungal (including Pneumocystis), viral, mycobacterial, and toxoplasmic infections are available at Clinical Info: Federally Approved Clinical Practice Guidelines for HIV/AIDS.
Immunization
The CDC 2024 recommendations for vaccination of patients aged ≥ 19 years with HIV infection include the following:
Patients who have not received a conjugate pneumococcal vaccine or whose previous vaccination history is unknown should be given PCV15 or PCV20; if PCV15 is given, follow with PPSV23 ≥ 8 weeks after the PCV15 dose.
All patients should be given the influenza vaccine annually.
All patients should be given the hepatitis B vaccine.
Patients at risk of hepatitis A or desiring protection from it should be given the hepatitis A vaccine.
At the appropriate age, males and females should be given the human papillomavirus (HPV) vaccine to prevent HPV-related cervical and anal cancers.
Adults who have not been previously vaccinated with the meningococcal vaccine should be given a 2-dose primary series of MenACWY ≥ 8 weeks apart and be revaccinated every 5 years.
Patients who did not receive tetanus-diphtheria-pertussis vaccine (Tdap) as part of their completed tetanus-diphtheria vaccine (Td) series should be given Tdap for their next Td booster. For patients who are beginning or continuing their Td series and have not yet been given Tdap, Tdap should be substituted for one of the Td boosters.
All patients should be given the recombinant zoster vaccine.
The varicella vaccine and the measles, mumps, and rubella (MMR) vaccine may be given to patients with CD4 percentage ≥ 15% and CD4 count ≥ 200/mcL, but these vaccines are contraindicated in patients with CD4 percentage < 15% or CD4 count < 200/mcL.
People with HIV should receive the full series of a COVID-19 vaccine, regardless of CD4 count or viral load because the potential benefits outweigh potential risks (4).
Mpox vaccination is recommended for people with HIV at risk for MPox. The only Mpox vaccine recommended for people with HIV is the modified vaccinia Ankara (Jynneos in the United States), which is made from a highly attenuated, nonreplicating vaccinia virus and has an excellent safety profile.
Generally, inactivated vaccines should be used. These vaccines are effective less often in patients who are HIV-positive than in those who are HIV-negative.
Pregnant women with HIV should receive the routine vaccinations recommended during pregnancy. Because live-virus vaccines are potentially dangerous for patients with severe immunosuppression, expert opinion should be sought when dealing with patients at risk of primary varicella; recommendations vary (see vaccination information in HIV in Infants and Children and see table ).
Treatment references
1. INSIGHT START Study Group, Lundgren JD, Babiker AG, et al: Initiation of antiretroviral therapy in early asymptomatic HIV infection. N Engl J Med 373 (9):795–807, 2015. doi:10.1056/NEJMoa1506816
2. Guidelines for the Prevention and Treatment of Opportunistic Infections in Adults and Adolescents with HIV: Disseminated Mycobacterium Avium Complex Disease. Accessed May 7, 2024.
3. Guidelines for the Prevention and Treatment of Opportunistic Infections in Adults and Adolescents with HIV: Cryptococcosis. Accessed May 7, 2024.
4. COVID Vaccine Guidance for COVID-19 and People With HIV: Accessed May 7, 2024.
Prognosis for HIV Infection
Risk of end-stage HIV, death, or both is predicted by the
CD4 count in the short term
Plasma HIV RNA level in the longer term
For every 3-fold (0.5 log10) increase in viral load, mortality over the next 2 to 3 years increases about 50% (1-3). HIV-associated morbidity and mortality vary by the CD4 count, with the most deaths from HIV-related causes occurring at counts of < 50/mcL. However, with effective treatment, the HIV RNA level decreases to undetectable levels, CD4 counts often increase dramatically, and risk of illness and death falls but remains higher than that for age-matched populations without HIV infection (4). Hence, prompt diagnosis of HIV before the disease is too advanced and immediate initiation of HIV treatment are essential to prognosis.
Another, less well-understood prognostic factor is the level of immune activation as determined by evaluating the expression of activation markers on CD4 and CD8 lymphocytes. Activation, which may be caused by leakage of bacteria across the HIV-damaged colonic mucosa, is a strong prognostic predictor but is not used clinically because this test is not widely available and antiretroviral therapy changes the prognosis, making this test less important.
A subgroup of people with HIV (termed long-term nonprogressors) remain asymptomatic with high CD4 counts and low HIV levels in the blood without antiretroviral treatment. These people usually have vigorous cellular and humoral immune responses to their infecting HIV strain as measured by assays in vitro. The specificity of this effective response is shown by the following: When these people acquire a superinfection with a second strain of HIV to which their immune response is not as effective, they convert to a more typical pattern of progression. Thus, their unusually effective response to the first strain does not apply to the second strain. These cases provide a rationale for counseling people with HIV infection that they still need to avoid exposure to possible HIV superinfection through unsafe sex or needle sharing.
Cure of HIV infection has not been thought possible, and thus lifelong drug treatment is considered necessary. Patients with HIV infection should be urged to take their antiretroviral drugs consistently. An instance of a possible functional cure was widely reported in an infant with transient eradication of replication-competent HIV after about 15 months of antiretroviral therapy (5). However, HIV replication subsequently resumed (6). Periodic HIV treatment interruption is also detrimental. In a large international clinical trial, risk of opportunistic infection or death from any cause, particularly from premature coronary artery disease, cerebrovascular events, or liver and kidney disorders, was significantly higher when antiretroviral therapy was taken episodically (guided by the CD4 count) than when it was taken continuously (7).
End-of-life care
Although antiretroviral therapy has dramatically increased life expectancy for patients with AIDS, many patients still deteriorate and die. Death may result from the following:
Inability to take ART consistently, resulting in progressive immunosuppression
Occurrence of untreatable opportunistic infections and cancers
Liver failure due to hepatitis B or C
Accelerated aging and age-related disorders
Non-AIDS–related cancers that occur at a higher rate in patients with otherwise well-controlled HIV infection
Death is rarely sudden; thus, patients usually have time to make plans. Nonetheless, patients should record their plans for health care early, with clear instructions for end-of-life care. Other legal documents, including powers of attorney and wills, should be in place.
As patients near the end of life, clinicians may need to prescribe drugs to relieve pain, anorexia, agitation, and other distressing symptoms. The profound weight loss in many people during the last stages of HIV makes good skin care difficult. The comprehensive support provided by hospice programs helps many patients because hospice providers are skilled at symptom management, and they support caregivers and patient autonomy.
Prognosis references
1. Mellors JW, Kingsley LA, Rinaldo CR, et al: Quantitation of HIV-1 RNA in plasma predicts outcome after seroconversion. Ann Internal Med 122(8):573-579, 1995. doi: 10.7326/0003-4819-122-8-199504150-00003
2. Mellors JW, Rinaldo CR, Gupta P, et al: Prognosis in HIV-1 infection predicted by the quantity of virus in plasma. Science 272(5265):1167-1170, 1996. doi:10.1126/science.272.5265.1167
3. Welles SL, Jackson JB, Yen-Lieberman B, et al: Prognostic value of plasma human immunodeficiency virus type 1 (HIV-1) RNA levels in patients with advanced HIV-1 disease and with little or no prior zidovudine therapy. AIDS Clinical Trials Group Protocol 116A/116B/117 Team. : Prognostic value of plasma human immunodeficiency virus type 1 (HIV-1) RNA levels in patients with advanced HIV-1 disease and with little or no prior zidovudine therapy. AIDS Clinical Trials Group Protocol 116A/116B/117 Team.J Infect Dis 174(4):696-703, 1996. doi:10.1093/infdis/174.4.696
4. Park LS, Tate JP, Sigel K, et al: Association of viral suppression with lower AIDS-defining and non-AIDS-defining cancer incidence in HIV-infected veterans: A prospective cohort study. Ann Intern Med 169(2):87-96, 2018. doi:10.7326/m16-2094
5. Persaud D, Gay H, Ziemniak C, et al: Absence of detectable HIV-1 viremia after treatment cessation in an infant. N Engl J Med 369(19):1828-1835, 2013. doi:10.1056/NEJMoa1302976
6. Ledford H: HIV rebound dashes hope of 'Mississippi baby' cure. Nature 2014. doi.org/10.1038/nature.2014.15535
7. Strategies for Management of Antiretroviral Therapy (SMART) Study Group, El-Sadr WM, Lundgren J, et al: CD4+ count-guided interruption of antiretroviral treatment. N Engl J Med 355(22):2283-2296, 2006. doi: 10.1056/NEJMoa062360
Prevention of HIV Infection
Vaccines against HIV have been difficult to develop because HIV surface proteins mutate easily, resulting in an enormous diversity of antigenic types. Nonetheless, various vaccine candidates are under investigation, and a few have shown promise in clinical trials. At the present time, there is no effective HIV vaccine.
Prevention of transmission
Vaginal microbicides (including antiretroviral drugs) inserted before sexual contact have thus far proved ineffective, and some appear to increase risk for women, perhaps by causing cellular damage and thus decreasing natural barriers to HIV.
Effective measures include the following:
Public education: Education is effective and appears to have decreased rates of infection in some countries, notably Thailand and Uganda. Because sexual contact accounts for most cases, teaching people to avoid unsafe sex practices is the most relevant measure (see table ).
Safer sex practices: People with HIV who are not virally suppressed (ie, do not have an undetectable viral load) should practice safer sex behaviors that are essential to prevent the spread of the infection. Virally suppressed people with HIV do not sexually transmit the virus to their partners (1). Safer sex practices should be used by a patient with HIV whose infection is not virally suppressed regardless of who they have sex with. Safer sex practices are also advised when both partners are HIV-positive and one or both partners are not virally suppressed; unprotected sex between people with virally unsuppressed-HIV infection may expose a person to resistant or more virulent strains of HIV. In addition, safer sex practices help to prevent transmission of other viruses (eg, cytomegalovirus, Epstein-Barr virus, herpes simplex virus, hepatitis B virus) that cause severe disease in end-stage HIV patients, as well as help to prevent transmission of syphilis and other sexually transmitted infections (STIs), including concerning infections such as multi-drug–resistant gonorrhea and sexually transmitted Neisseria meningitidis. Condoms offer the best protection. Oil-based lubricants should not be used because they may dissolve latex, increasing the risk of condom failure. (See also the Center for Disease Control and Prevention (CDC) information on HIV Transmission.)
Counseling for people who use parenteral drugs: Counseling about the risk of sharing needles is important but is probably more effective if combined with provision of sterile needles and syringes to reduce transmission of HIV and other bloodborne viruses that are acquired by sharing contaminated injecting equipment, treatment of drug dependence, and rehabilitation.
Confidential testing for HIV infection: Testing should be offered routinely to sexually active adolescents and adults ages 13 to 75 in virtually all health care settings. To facilitate routine testing, some states no longer require written consent or extensive pre-test counseling.
Counseling for pregnant women: Mother-to-child transmission has been virtually eliminated by HIV testing, treatment with ART, and, in high-resource countries, use of breast milk substitutes. If pregnant women are known to have HIV infection or test positive for HIV, they should be counseled about the risk of mother-to-child transmission. Pregnant women with HIV infection should be encouraged to accept therapy to prevent infection of the fetus or newborn, typically beginning at about 14 weeks gestation. Combination therapy is typically used because it is more effective than monotherapy and less likely to result in drug resistance. Some drugs can be toxic to the fetus or woman and should be avoided. If women meet criteria for ART, they should begin a regimen tailored to their history and stage of pregnancy and continue it throughout pregnancy. Cesarean delivery can also reduce risk of transmission. Regardless of the antepartum regimen used or mode of delivery, all women with HIV infection should be given IV zidovudine during labor, and after birth, neonates should be given oral zidovudine, which is continued for 6 weeks after delivery (see also has been virtually eliminated by HIV testing, treatment with ART, and, in high-resource countries, use of breast milk substitutes. If pregnant women are known to have HIV infection or test positive for HIV, they should be counseled about the risk of mother-to-child transmission. Pregnant women with HIV infection should be encouraged to accept therapy to prevent infection of the fetus or newborn, typically beginning at about 14 weeks gestation. Combination therapy is typically used because it is more effective than monotherapy and less likely to result in drug resistance. Some drugs can be toxic to the fetus or woman and should be avoided. If women meet criteria for ART, they should begin a regimen tailored to their history and stage of pregnancy and continue it throughout pregnancy. Cesarean delivery can also reduce risk of transmission. Regardless of the antepartum regimen used or mode of delivery, all women with HIV infection should be given IV zidovudine during labor, and after birth, neonates should be given oral zidovudine, which is continued for 6 weeks after delivery (see alsoPrevention of Perinatal Transmission). Some women choose to terminate their pregnancy because HIV can be transmitted in utero to the fetus or for other reasons.
Screening of blood and organs: Transmission by blood transfusion is still remotely possible in the United States because antibody results may be false-negative during early infection. Currently, screening blood for antibody and p24 antigen is mandated in the United States and probably further reduces risk of transmission. Risk is reduced further by asking people with risk factors for HIV infection, even those with recent negative HIV antibody test results, not to donate blood or organs for transplantation. The Red Cross has issued guidance for deferral of blood donation, including deferral for having had a new sex partner or more than one sex partner in the previous 3 months and having engaged in anal sex in the last 3 months (see American Red Cross Blood Donation Eligibility Criteria: Alphabetical ). However, use of sensitive HIV screening tests and deferral of donors of organs, blood, and blood products have not been implemented consistently in high HIV burden countries.
Preexposure prophylaxis with antiretrovirals (PrEP): PrEP is the use of antiretroviral medications by people without HIV infection to prevent acquisition of HIV (eg, by having a sex partner with HIV). The CDC recommends PrEP for sexually active adults and adolescents weighing ≥ 35 kg (77 lb) who are at substantial risk of HIV exposure, including those with an HIV-positive partner or engaging in condomless sex, as well as people who inject drugs and share injection equipment. Use of PrEP should be part of a comprehensive prevention strategy, which includes consistent condom use, STI screening, and harm reduction measures.
Two oral PrEP combination regimens are available: tenofovir disoproxil fumarate plus emtricitabine (TDF/FTC), which can be used for all at-risk populations, including those with injection drug use risk, and tenofovir alafenamide-emtricitabine (TAF-FTC), which can be used for individuals at sexual risk Two oral PrEP combination regimens are available: tenofovir disoproxil fumarate plus emtricitabine (TDF/FTC), which can be used for all at-risk populations, including those with injection drug use risk, and tenofovir alafenamide-emtricitabine (TAF-FTC), which can be used for individuals at sexual riskexcept those at risk via receptive vaginal sex (due to lack of efficacy data). While data on the use of oral PrEP during pregnancy are limited, TDF/FTC has not been associated with adverse effects in children born to women with HIV infection treated with TDF/FTC.
Two long-acting injectable antiretroviral agents have recently expanded PrEP options: Cabotegravir LA, an injectable integrase inhibitor, is recommended for all populations at risk of sexual HIV acquisition, including adolescents ≥ 35 kg. Lenacapavir, an HIV-1 capsid inhibitor, can be used for all individuals at risk of sexually acquired HIV, including pregnant people. Lenacapavir is administered every 6 months, with oral lead-in doses on days 1 and 2 and offers a biannual option for those who prefer less frequent dosing. For the current CDC recommendations, see Two long-acting injectable antiretroviral agents have recently expanded PrEP options: Cabotegravir LA, an injectable integrase inhibitor, is recommended for all populations at risk of sexual HIV acquisition, including adolescents ≥ 35 kg. Lenacapavir, an HIV-1 capsid inhibitor, can be used for all individuals at risk of sexually acquired HIV, including pregnant people. Lenacapavir is administered every 6 months, with oral lead-in doses on days 1 and 2 and offers a biannual option for those who prefer less frequent dosing. For the current CDC recommendations, seeClinical Guidance for PrEP.
Circumcision of men: Data from young African men show that circumcision reduces the risk of acquiring HIV infection from female partners during vaginal sex by about 50%; male circumcision is probably similarly effective in other male-patient populations. Whether male circumcision reduces HIV transmission from HIV-positive men to women or reduces the risk of acquiring HIV from an infected male partner is unknown.
Universal precautions: Medical and dental clinicians should wear gloves in situations that may involve contact with any patient’s mucous membranes or body fluids and should be taught how to avoid needlestick accidents. Home caregivers of patients with HIV infection should wear gloves if their hands may be exposed to body fluids. Surfaces or instruments contaminated by blood or other body fluids should be cleaned and disinfected. Effective disinfectants include heat, peroxide, alcohols, phenolics, and hypochlorite (bleach). Isolation of patients with HIV infection is unnecessary unless indicated by an active opportunistic infection (eg, tuberculosis).
Treatment of HIV infection: Treatment with ART lowers the risk of transmission.
Postexposure prophylaxis (PEP)
Potential consequences of exposure to HIV have prompted the development of policies and procedures, particularly preventive treatment, to decrease risk of infection to health care workers.
Preventive treatment is indicated after
Penetrating injuries involving HIV-infected blood (usually needlesticks)
Heavy exposure of mucous membranes (eye or mouth) to infected body fluids such as semen, vaginal fluids, or other body fluids containing blood (eg, amniotic fluid)
Body fluids such as saliva, urine, tears, nasal secretions, vomitus, or sweat are not considered potentially infectious unless they are visibly bloody.
After initial exposure to blood, the exposed area is immediately cleaned with soap and water for skin exposures and with antiseptic for puncture wounds. If mucous membranes are exposed, the area is flushed with large amounts of water.
The following are documented:
Type of exposure
Time elapsed since exposure
Clinical information (including risk factors and serologic tests for HIV) about the source patient for the exposure and the person exposed
Type of exposure is defined by
Which body fluid was involved
Whether exposure involved a penetrating injury (eg, needlestick, cut with sharp object) and how deep the injury was
Whether the fluid had contact with nonintact skin (eg, abraded or chapped skin) or mucous membrane
Risk of infection is about 0.3% (1:300) after a typical percutaneous exposure and about 0.09% (1:1100) after mucous membrane exposure. These risks vary, reflecting the amount of HIV transferred to the person with the injury; the amount of HIV transferred is affected by multiple factors, including viral load of the source and type of needle (eg, hollow or solid). However, these factors are no longer taken into account in PEP recommendations.
The source is qualified by whether it is known or unknown. If the source is unknown (eg, a needle on the street or in a sharps disposal container), risk should be assessed based on the circumstances of the exposure (eg, whether the exposure occurred in an area where injection drug use is prevalent, whether a needle discarded in a drug-treatment facility was used). If the source is known but HIV status is not, the source is assessed for HIV risk factors, and prophylaxis is considered.
The goal is to start PEP as soon after exposure as possible if prophylaxis is warranted. CDC recommends providing PEP within 24 to 36 hours after exposure; a longer interval after exposure requires the advice of an expert.
Use of PEP is determined by risk of acquisition; current guidelines recommend initiation of a 28-day course of ≥ 3 antiretroviral medications (2), ideally started as soon as possible and no later than 72 hours after exposure. The medications should be carefully selected to minimize adverse effects, support once-daily dosing, and optimize adherence and completion. Preferred regimens include a combination of 2 nucleoside reverse transcriptase inhibitors (NRTIs) and an integrase inhibitor, either bictegravir-emtricitabine-tenofovir alafenamide or dolutegravir in combination with either tenofovir disoproxil fumarate-emtricitabine (TDF/FTC) or tenofovir alafenamide-emtricitabine (TAF/FTC). An alternative integrase-inhibitor-based regimen includes raltegravir (400 mg twice daily) with TDF/FTC or TAF/FTC administered once daily. In rare occasions where an integrase inhibitor-based regimen is contraindicated or not tolerated, a boosted protease inhibitor-based regimen (eg, darunavir plus TDF/FTC or TAF/FTC) may be used. (For detailed recommendations, see ), ideally started as soon as possible and no later than 72 hours after exposure. The medications should be carefully selected to minimize adverse effects, support once-daily dosing, and optimize adherence and completion. Preferred regimens include a combination of 2 nucleoside reverse transcriptase inhibitors (NRTIs) and an integrase inhibitor, either bictegravir-emtricitabine-tenofovir alafenamide or dolutegravir in combination with either tenofovir disoproxil fumarate-emtricitabine (TDF/FTC) or tenofovir alafenamide-emtricitabine (TAF/FTC). An alternative integrase-inhibitor-based regimen includes raltegravir (400 mg twice daily) with TDF/FTC or TAF/FTC administered once daily. In rare occasions where an integrase inhibitor-based regimen is contraindicated or not tolerated, a boosted protease inhibitor-based regimen (eg, darunavir plus TDF/FTC or TAF/FTC) may be used. (For detailed recommendations, seeThe 2022 Recommendations of the International Antiviral Society—USA Panel: Antiretroviral Drugs for Treatment and Prevention of HIV Infection in Adults and Antiretroviral Postexposure Prophylaxis After Sexual, Injection Drug Use, or Other Nonoccupational Exposure to HIV — CDC Recommendations, United States, 2025.)
HIV testing on the exposed patient should be done at the initial visit (using point-of-care and/or laboratory-based antigen/antibody testing). Follow-up HIV testing is recommended at should be done at 4 to 6 weeks and again at 12 weeks after exposure using a fourth-generation Ag/Ab combination assay (2).
If the source’s virus is known or suspected to be resistant to ≥ 1 drug, an expert in antiretroviral therapy and HIV transmission should be consulted. However, clinicians should not delay PEP pending expert consultation or drug susceptibility testing. Also, clinicians should provide immediate evaluation and face-to-face counseling and not delay follow-up care.
In patients who may become or are pregnant, first-line postexposure prophylaxis regimens are similar to those for nonpregnant patients, including TDF/FTC or TAF/FTC once daily plus either dolutegravir (50 mg once daily) or raltegravir (400 mg twice daily). Bictegravir-emtricitabine-tenofovir alafenamide is generally avoided in pregnant women and persons of childbearing potential who are not on effective contraception because there are limited data on its use during pregnancy (In patients who may become or are pregnant, first-line postexposure prophylaxis regimens are similar to those for nonpregnant patients, including TDF/FTC or TAF/FTC once daily plus either dolutegravir (50 mg once daily) or raltegravir (400 mg twice daily). Bictegravir-emtricitabine-tenofovir alafenamide is generally avoided in pregnant women and persons of childbearing potential who are not on effective contraception because there are limited data on its use during pregnancy (3).
Prevention references
1. Rodger AJ, Cambiano V, Bruun T, et al: Sexual activity without condoms and risk of HIV transmission in serodifferent couples when the HIV-positive partner is using suppressive antiretroviral therapy. JAMA 316(2):171-81, 2016. doi:10.1001/jama.2016.5148
2. Tanner MR, O'Shea JG, Byrd KM, et al. Antiretroviral Postexposure Prophylaxis After Sexual, Injection Drug Use, or Other Nonoccupational Exposure to HIV - CDC Recommendations, United States, 2025. MMWR Recomm Rep. 2025;74(1):1-56. Published 2025 May 8. doi:10.15585/mmwr.rr7401a1
3. Gandhi RT, Bedimo R, Hoy JF, et al: Antiretroviral drugs for treatment and prevention of HIV infection in adults: 2022 Recommendations of the International Antiviral Society-USA Panel. JAMA 329(1):63-84, 2023. doi:10.1001/jama.2022.22246
Key Points
HIV infects CD4+ lymphocytes and thus interferes with cell-mediated and, to a lesser extent, humoral immunity.
HIV is spread mainly by sexual contact, parenteral exposure to contaminated blood or transplanted tissue or organs, and vertical transmission (in utero, during childbirth, or through breastfeeding).
Frequent viral mutations combined with immune system damage significantly impair the body's ability to clear the HIV infection.
Various opportunistic infections and cancers can develop and are the usual cause of death in untreated patients.
Diagnose using antibody tests, and monitor by measuring viral load and CD4 count.
Treat with a combination of antiretroviral drugs, which can restore immune function to nearly normal in most patients if they take the drugs consistently.
Periodically counsel patients with HIV about safer sex.
Use postexposure and preexposure antiretroviral prophylaxis when indicated.
Give primary prophylaxis against opportunistic infections based on the CD4 count.
More Information
The following English-language resources may be useful. Please note that THE MANUAL is not responsible for the content of these resources.
CDC 2024 Immunization Schedule: Recommended adult immunization schedule by medical condition and other indications
Guidelines for the Use of Antiretroviral Agents in HIV-1-Infected Adults and Adolescents: Drug-Drug Interactions: Information regarding pharmacokinetic (PK) drug-drug interactions between antiretroviral (ARV) drugs and concomitant medications that are common and may lead to increased or decreased drug exposure
Guidelines on Post-Exposure Prophylaxis for HIV and the Use of Co-Trimoxazole Prophylaxis for HIV-Related Infections Among Adults, Adolescents and Children: Recommendations for a public health approach - December 2014 supplement to the 2013 consolidated ARV guidelines
National Institutes of Health's AIDSInfo: HIV-related research information from the NIH’s Office of AIDS Research (OAR), the National Institute Of Allergy and Infectious Diseases (NIAID), and the U.S. National Library of Medicine (NLM)
CDC: Post-Exposure Prophylaxis (PEP): Resources for providers and consumer regarding the use of antiretroviral drugs after a single high-risk event to stop HIV seroconversion
Primary Care Guidelines for the Management of Persons Infected with Human Immunodeficiency Virus: 2020 Update by the HIV Medicine Association of the Infectious Diseases Society of America: Evidence-based guidelines for the management of people infected with HIV
Updated U.S. Public Health Service Guidelines for the Management of Occupational Exposures to HIV and Recommendations for Postexposure Prophylaxis (PEP): Updated recommendations regarding HIV PEP regimens and the duration of HIV follow-up testing for exposed personnel
American Red Cross Blood Donation Eligibility Criteria: Alphabetical: Revised guidance document providing blood establishments that collect blood or blood components, including Source Plasma, with revised donor deferral recommendations for individuals with increased risk for transmitting HIV infection
Drugs Mentioned In This Article





