

Subacute meningitis develops over days to a few weeks. Chronic meningitis lasts ≥ 4 weeks. Possible causes include fungi, Mycobacterium tuberculosis, rickettsiae, spirochetes, Toxoplasma gondii, HIV, enteroviruses, and disorders such as autoimmune rheumatic disorders (eg, systemic lupus erythematosus [SLE], rheumatoid arthritis [RA]) and cancer. Symptoms and signs are similar to those of other meningitides but more indolent. Cranial nerve palsies and infarction (due to vasculitis) may occur. Diagnosis requires analysis of a large volume of cerebrospinal fluid (CSF) that is typically obtained via repeated lumbar punctures or sometimes ventricular or cisternal puncture with or without biopsy, followed by next-generation sequencing of DNA in CSF (if available). Treatment is directed at the cause.
(See also Overview of Meningitis.)
Chronic meningitis may last > 10 years. Rarely, chronic meningitis has a protracted benign course, then resolves spontaneously.
Subacute and chronic meningitis may result from a wide variety of organisms and conditions.
Major Infectious Causes of Subacute or Chronic Meningitis
Organisms | Circumstances |
|---|---|
Bacteria | |
Mycobacteria: (Mycobacterium tuberculosis, rarely other mycobacteria) | — |
Spirochetes: Lyme disease, syphilis, rarely leptospirosis | For Lyme disease, East Coast, upper Midwest, California, Oregon |
Brucella species | Associated with livestock Unusual in the United States or other high-resource countries |
Ehrlichia species | Tick bites |
Leptospira species | Associated with exposure to urine of rats, mice, and other animals Unusual in Western countries |
Fungi | |
Cryptococcus neoformans | Most common among immunocompromised patients, particularly those with HIV infection |
C. gattii | Predominantly northern Pacific coast Appears to have a widespread distribution |
Coccidioides immitis | Southwestern United States |
Histoplasma capsulatum | Central and Eastern United States |
Blastomyces species | Predominantly Central and Eastern United States |
Sporothrix species (unusual) | No geographic distribution, but infection associated with rose thorns or brush |
Parasites | |
Toxoplasma gondii | Cat feces, contaminated meat |
Viruses | |
Retroviruses: HIV; human T-lymphotropic virus, type 1 | In patients with known HIV or risk factors |
Enteroviruses | In patients with a congenital immunodeficiency syndrome |
Tuberculous meningitis
Mycobacterium tuberculosis are aerobic bacteria that replicate in host cells; thus, control of these bacteria depends largely on T cell–mediated immunity. These bacteria may infect the central nervous system (CNS) during primary or reactivated infection. In high-resource countries, meningitis usually results from reactivated infection. Reactivation may occur in patients treated with immunosuppressants such as tumor necrosis factor (TNF)-alpha antagonists (eg, infliximab, adalimumab, golimumab, certolizumab, etanercept).are aerobic bacteria that replicate in host cells; thus, control of these bacteria depends largely on T cell–mediated immunity. These bacteria may infect the central nervous system (CNS) during primary or reactivated infection. In high-resource countries, meningitis usually results from reactivated infection. Reactivation may occur in patients treated with immunosuppressants such as tumor necrosis factor (TNF)-alpha antagonists (eg, infliximab, adalimumab, golimumab, certolizumab, etanercept).
Meningeal symptoms usually develop over days to a few weeks but may develop much more rapidly or gradually.
Characteristically, M. tuberculosis causes a basilar meningitis that results in 3 complications:
Hydrocephalus due to obstruction of the foramina of Luschka and Magendie or the aqueduct of Sylvius
Vasculitis, sometimes causing arterial or venous occlusion and stroke
Cranial nerve deficits, particularly of the 2nd, 7th, and 8th cranial nerves

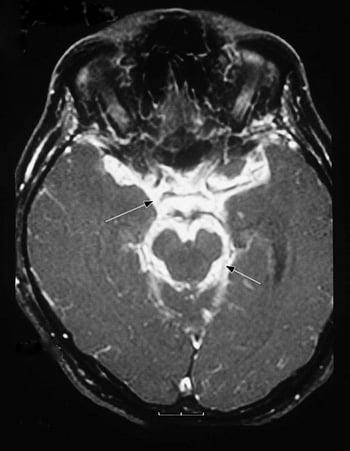
This magnetic resonance imaging (MRI) scan of a patient with tuberculous meningitis shows intense inflammatory exudate at the base of the brain (basilar meninges [arrows]) and surrounding the brain stem.
Diagnosis of tuberculous meningitis may be difficult. There may be no evidence of systemic tuberculosis. Inflammation of the basilar meninges, shown by contrast-enhanced CT or MRI, suggests the diagnosis.
Characteristically, cerebrospinal fluid (CSF) findings include
Mixed pleocytosis with lymphocytic predominance
Low glucose
Elevated protein
Occasionally, the first CSF abnormality is extremely low glucose.
Detecting the causative organism is often difficult because
CSF acid-fast staining is < 20% sensitive, even using immunofluorescence techniques.
CSF mycobacterial cultures are only about 70% sensitive and require up to 6 weeks.
CSF PCR is about 50 to 70% sensitive.
An automated rapid nucleic acid amplification test called Xpert MTB/RIF has been recommended by the World Health Organization (WHO) for the diagnosis of tuberculous meningitis. This test detects M. tuberculosis DNA and resistance to rifampicin in CSF specimens. Skin testing with controls for anergy or QuantiFERON-TB Gold testing can document prior exposure to M. tuberculosis; however, results may be negative, particularly in older or immunosuppressed patients. Chest x-rays may show evidence of prior or ongoing infection (in 40 to 50% of cases), and chest CT is positive in up to two-thirds of cases.
Because tuberculous meningitis has a rapid and destructive course and because diagnostic tests are limited, this infection should be treated based on clinical suspicion. Currently, the WHO recommends treatment with the anti-tuberculosis agents isoniazid, rifampin, pyrazinamide, and ethambutol for 2 months followed by isoniazid and rifampin for 6 to 7 months. Corticosteroids (prednisone or dexamethasone) may be added if patients present with stupor, coma, or neurologic deficits (isoniazid, rifampin, pyrazinamide, and ethambutol for 2 months followed by isoniazid and rifampin for 6 to 7 months. Corticosteroids (prednisone or dexamethasone) may be added if patients present with stupor, coma, or neurologic deficits (1).
Meningitis due to spirochetes
Lyme disease is a chronic spirochetal infection caused by Borrelia burgdorferi in the United States and by B. afzelii and B. garinii in Europe. Lyme disease is spread by Ixodes ticks, usually the deer tick in the United States. In the United States, 12 states account for 95% of cases. The states include mid-Atlantic and northeastern coastal states, Wisconsin, California, Oregon, and Washington. Up to 8% of children and some adults who contract Lyme disease develop meningitis. The meningitis may be acute or chronic; usually, it begins more slowly than acute viral meningitis.
Clues to the diagnosis include
Time spent in wooded areas and travel to an endemic area (including in Europe)
History of erythema migrans or other symptoms of Lyme disease
Unilateral or bilateral facial palsy (common in Lyme disease but rare in most viral meningitides)
Papilledema (well-described in children with Lyme disease but rare in viral meningitis)
CSF findings typically include
Lymphocytic pleocytosis
Moderately elevated protein
Normal glucose
Diagnosis of Lyme disease is based on serologic tests with enzyme-linked immunosorbent assay (ELISA), followed by Western blot analysis to confirm. In some laboratories, false-positive rates may be unacceptably high.
Treatment of Lyme meningitis is with cefotaxime or ceftriaxone given over 14 days. Treatment of Lyme meningitis is with cefotaxime or ceftriaxone given over 14 days.
Clinicians should remember that concomitant anaplasmosis or babesiosis is possible in patients with severe disease.
Syphilitic meningitis
Syphilitic meningitis is less common; it is usually a feature of meningovascular syphilis. The meningitis may be acute or chronic. It may be accompanied by complications such as cerebrovascular arteritis (possibly causing thrombosis with ischemia or infarction), retinitis, cranial nerve deficits (especially of the 7th cranial nerve), or myelitis.
CSF findings may include
Pleocytosis (usually lymphocytic)
Elevated protein
Low glucose
These abnormalities may be more pronounced in patients with late stage HIV infection.
Diagnosis of syphilitic meningitis is based on serum and CSF serologic tests, followed by fluorescent treponemal antibody absorption (FTA-ABS) testing to confirm. Magnetic resonance angiography and cerebral angiography may accurately differentiate between parenchymal disease and arteritis. Nontreponemal tests, RPR and VDRL, may also be performed on CSF. These tests detect IgG evidence of exposure to T. pallidum.
Patients with syphilitic meningitis are treated with aqueous penicillin 12 to 24 million units IV/day given in divided doses every 4 hours (eg, 2 to 4 million units every 4 hours) for 10 to 14 days.
Cryptococcal meningitis
Cryptococcal meningitis is the most common cause of chronic meningitis in the Western hemisphere and the most common opportunistic infection in patients with AIDS. Common causes of cryptococcal meningitis in the United States are
Cryptococcus neoformans var. neoformans (serotype D strains)
C. neoformans var. grubii (serotype A strains)
C. neoformans var. grubii causes 90% of cases of cryptococcal meningitis. C. neoformans can be in soil, trees, and pigeon or other bird excreta. Meningitis due to C. neoformans usually develops in immunocompromised patients but occasionally develops in patients without apparent underlying disease.
Another cryptococcal species, C. gattii, has caused meningitis in the Pacific region and Washington state; it may cause meningitis in people with a normal immune status.
Cryptococci cause a basilar meningitis with hydrocephalus and cranial nerve deficits; vasculitis is less common. Meningeal symptoms usually begin insidiously, at times with protracted relapses and remissions. Cryptococcal meningitis may develop and persist over months or years.
CSF findings typically include
Lymphocytic pleocytosis
Elevated protein
Low glucose
However, cellular response may be minimal or absent in patients with advanced AIDS or another severe immunocompromised state.
Diagnosis of cryptococcal meningitis is based on cryptococcal antigen tests and fungal culture. India ink preparation may also be used (2). Occasionally, diagnosis is extremely difficult and may require examination of multiple large (20 to 30 mL) amounts of CSF over a period of time. Tests for cryptococcal antigen and fungal culture should be done each time.
Patients who have C. neoformans meningitis but do not have advanced HIV infection are traditionally treated with the synergistic combination of 5-fluorocytosine and amphotericin B. Patients with cryptococcal meningitis and advanced HIV infection are treated with amphotericin B plus flucytosine (if tolerated) followed by fluconazole. Maintenance therapy with fluconazole 200 mg daily has been shown to be highly effective at preventing relapse (meningitis but do not have advanced HIV infection are traditionally treated with the synergistic combination of 5-fluorocytosine and amphotericin B. Patients with cryptococcal meningitis and advanced HIV infection are treated with amphotericin B plus flucytosine (if tolerated) followed by fluconazole. Maintenance therapy with fluconazole 200 mg daily has been shown to be highly effective at preventing relapse (3).
Fungal meningitis that develops after epidural methylprednisolone injection
Occasionally, outbreaks of fungal meningitis have occurred in patients given spinal epidural injections of methylprednisolone. In each case, the drug had been prepared by a compounding pharmacy, and there were significant violations of sterile technique during drug preparation.Occasionally, outbreaks of fungal meningitis have occurred in patients given spinal epidural injections of methylprednisolone. In each case, the drug had been prepared by a compounding pharmacy, and there were significant violations of sterile technique during drug preparation.
The first outbreak in the United States (in 2002) resulted in 5 cases of meningitis. The most recent outbreak (in late 2012 and 2013) resulted in 753 cases of meningitis, stroke, myelitis, or other fungal infection-related complications and in 61 deaths. Outbreaks have also occurred in Sri Lanka (7 cases) and Minnesota (1 case). Most cases were caused by Exophiala dermatitidis in 2002 and by Exserohilum rostratum in 2012 and 2013; a few cases were caused by Aspergillus or Cladosporium species.
The meningitis tends to develop insidiously, often with infection at the base of the brain; blood vessels may be affected, resulting in vasculitis and stroke. Headache is the most common presenting symptom, followed by altered cognition, nausea or vomiting, or fever. Symptoms may be delayed by as much as 6 months after the epidural injection. Signs of meningeal irritation are absent in about one-third of patients.
Typical CSF findings include
Neutrophilic pleocytosis
Elevated protein
Frequently low glucose
The most sensitive test for Exserohilum meningitis is a CSF polymerase chain reaction (PCR) test, available through the Centers for Disease Control and Prevention (CDC); in a few cases, the diagnosis can be based on culture.
Aspergillus meningitis may be suspected if galactomannan levels in CSF are elevated; diagnosis is based on culture.
Meningitis due to Exophiala or Exserohilum species is rare, and definitive treatment is not known. However, voriconazole 6 mg/kg/day IV is recommended initially. Dosage should be adjusted based on blood levels of the medication. Liver enzyme and sodium levels should be measured periodically during the 2 to 3 weeks after initiation of treatment.species is rare, and definitive treatment is not known. However, voriconazole 6 mg/kg/day IV is recommended initially. Dosage should be adjusted based on blood levels of the medication. Liver enzyme and sodium levels should be measured periodically during the 2 to 3 weeks after initiation of treatment.
Prognosis is guarded, and appropriate treatment does not guarantee survival.
Other fungal meningitides
Coccidioides, Histoplasma, Blastomyces, Sporothrix, and Candida species may all cause chronic meningitis similar to that caused by C. neoformans. Coccidioides species are confined to the American Southwest (predominantly southern Utah, New Mexico, Arizona, and California). Histoplasma and Blastomyces species occur predominantly in the central and eastern United States. Cranial nerve deficits are common. Thus, if patients with subacute meningeal symptoms reside in or travel to this region, clinicians should suspect the appropriate fungal causes.
CSF findings typically include
Lymphocytic pleocytosis
Elevated protein
Low glucose
Candida species may also cause polymorphonuclear pleocytosis.
Coccidioidal meningitis tends to resist treatment and may require lifelong treatment with fluconazole. Voriconazole and amphotericin B have also been used. Treatment of the other fungal meningitides is usually with amphotericin B.Coccidioidal meningitis tends to resist treatment and may require lifelong treatment with fluconazole. Voriconazole and amphotericin B have also been used. Treatment of the other fungal meningitides is usually with amphotericin B.
Chronic meningitis in patients with HIV infection
Meningitis is common among HIV-infected patients. Most CSF abnormalities result from HIV, which invades the CNS early in the infection. Onset of meningitis and meningeal symptoms often coincides with seroconversion. Meningitis may then remit or follow a steady or fluctuating course.
However, many other organisms can cause chronic meningitis in patients with HIV infection. They include C. neoformans (the most common), M. tuberculosis, Treponema pallidum, and Coccidioides immitis in endemic areas. CNS lymphoma can also cause symptoms and signs similar to those of meningitis in patients with HIV infection.
Regardless of the cause, parenchymal lesions may develop.
Carcinomatous meningitis
In patients with cancer, tumor cells may spread to the meninges. Spread most commonly occurs in patients with lung or breast cancer and melanoma but can occur in many other cancers. Carcinomatous meningitis is usually a late complication of cancer and should be considered if any patient with cancer has a change in mental status, hydrocephalus, or clinical signs referable to cranial or spinal nerve roots.
Similar leptomeningeal involvement can also occur in patients with leukemias or lymphomas, including primary CNS lymphoma.
CSF changes may be nonspecific (pleocytosis, low glucose, elevated protein); detection of malignant cells may require multiple lumbar punctures. MRI with gadolinium is used to detect metastatic deposits on nerve roots or other structures.
Treatment is directed against the underlying tumor, but prognosis is poor; the cancer usually recurs within 6 months.
Other causes of chronic meningitis
Rarely, other infectious organisms and some noninfectious disorders (see table ) cause chronic meningitis. Noninfectious causes include
Autoimmune rheumatic disorders, including systemic lupus erythematosus (SLE), rheumatoid arthritis (RA), and Sjögren syndrome
Chronic idiopathic meningitis
Occasionally, chronic, usually lymphocytic meningitis persists for months or even years, but no organisms are identified; and death does not result. In some patients, the meningitis eventually remits spontaneously. Generally, empiric trials of antifungal drugs or corticosteroids have not been helpful.
References
1. World Health Organization. WHO consolidated guidelines on tuberculosis: Module 4: treatment: drug-susceptible tuberculosis treatment.
2. Tai S, Liang C, Tao J, Zhou J. Cryptococcal invasion: a comprehensive case of adrenal and systemic infection amid immunosuppression. BMC Infect Dis. 2024;24(1):1119. Published 2024 Oct 8. doi:10.1186/s12879-024-09737-8
3. Rajasingham R, Smith RM, Park BJ, et al: Global burden of disease of HIV-associated cryptococcal meningitis: An updated analysis. Lancet Infect Dis 7(8):873-881, 2017. doi: 10.1016/S1473-3099(17)30243-8
Diagnosis of Subacute and Chronic Meningitis
CSF analysis
Clinical findings in patients with subacute or chronic meningitis are often nonspecific. However, a careful search for a systemic infection or disorder may suggest a cause for meningitis. Also, sometimes risk factors (eg, immunocompromise, HIV infection or risk factors for it, recent time spent in endemic areas) and occasionally specific neurologic deficits (eg, particular cranial nerve deficits) suggest specific causes, such as C. neoformans meningitis in HIV-infected patients or C. immitis infections in patients living in the southwestern United States.
Typically, CSF findings include lymphocytic pleocytosis. In many of the infections that cause chronic meningitis, CSF contains only a few of the organisms, making identification of the cause difficult. Thus, diagnosis of subacute or chronic meningitis based on CSF findings may require multiple large samples over time, particularly for cultures.
CSF analysis commonly includes
Aerobic and anaerobic bacterial culture
Mycobacterial and fungal culture
Cryptococcal antigen testing
Antigen or serologic testing for suspected etiologic agents
Special stains (eg, acid-fast staining, India ink)
Cytology
If available, next-generation (metagenomic) sequencing can be used to rapidly sequence large stretches of nucleic acids and thus identify otherwise undetectable pathogens in CSF.
If clinicians suspect tuberculous meningitis, they can use an automated test called Xpert MTB/RIF, which has been recommended by the WHO for the diagnosis of tuberculous meningitis. This test can detect the DNA of Mycobacterium tuberculosis in CSF specimens. Skin testing with controls for anergy or QuantiFERON-TB Gold testing can document prior exposure to M. tuberculosis; however, results may be negative, particularly in older or immunosuppressed patients. Chest x-rays may show evidence of prior or ongoing infection, and chest CT is positive in up to two-thirds of cases.
If CSF findings do not provide a diagnosis and meningitis is causing morbidity or is progressive, more invasive testing (eg, cisternal or ventricular puncture, biopsy) is indicated. Occasionally, organisms are recovered from ventricular or cisternal CSF when lumbar CSF is negative.
MRI or CT may be done to identify focal areas of inflammation for biopsy; blind meningeal biopsy has a very low yield.
Treatment of Subacute and Chronic Meningitis
Treatment of the cause
Treatment of subacute or chronic meningitis is directed at the cause (for mycobacterial, spirochetal, and fungal meningitides, see above; for other causes, see elsewhere in The Manual).
Key Points
Consider risk factors (eg, time spent in endemic areas, HIV infection or risk factors for it, immunocompromise, autoimmune rheumatic disorders) to help identify likely causes.
Carefully checking for a systemic infection or disorder may provide the diagnosis.
Many samples may be needed for CSF analysis because CSF may contain few of the causative organisms; sometimes diagnosis requires cisternal or ventricular puncture and/or biopsy.
Treatment is directed at the cause.
Drug Information for the Topic





