



Esophageal infection occurs mainly in patients with impaired host defenses. Primary infectious agents include Candida albicans, herpes simplex virus, and cytomegalovirus. Symptoms are odynophagia and chest pain. Diagnosis is by endoscopic visualization and culture. Treatment is with antifungal or antiviral medications.
Primary esophageal defenses include saliva, esophageal motility, and cellular immunity. Thus, at-risk patients include those with advanced HIV, organ transplants, alcohol use disorder, diabetes, undernutrition, cancer, and esophageal motility disorders. Additionally, swallowed or inhaled glucocorticoids may increase the risk of infectious esophagitis. Candida infection may occur in any of these patients. Herpes simplex virus (HSV) and cytomegalovirus (CMV) infections occur mainly in patients with HIV or a transplant. Esophageal infection is rare but possible in patients with normal host defenses (1, 2).
General references
1. O'Rourke A. Infective oesophagitis: epidemiology, cause, diagnosis and treatment options. Curr Opin Otolaryngol Head Neck Surg. 2015;23(6):459-463. doi:10.1097/MOO.0000000000000199
2. Reddy CA, McGowan E, Yadlapati R, Peterson K. AGA Clinical Practice Update on Esophageal Dysfunction Due to Disordered Immunity and Infection: Expert Review. Clin Gastroenterol Hepatol. 2024;22(12):2378-2387. doi:10.1016/j.cgh.2024.08.027
Candida Esophagitis
Patients with Candida esophagitis usually have odynophagia and, less commonly, dysphagia. In addition to the general risk factors for infectious esophagitis, proton pump inhibitor use also appears to be a risk factor (1, 2).
Many patients with Candida esophagitis have signs of oral thrush, but the absence of oral thrush does not exclude esophageal involvement. Patients with odynophagia and typical thrush may be given empiric treatment, but if significant improvement does not occur in 5 to 7 days, endoscopic evaluation is required (3). Barium swallow is less accurate.

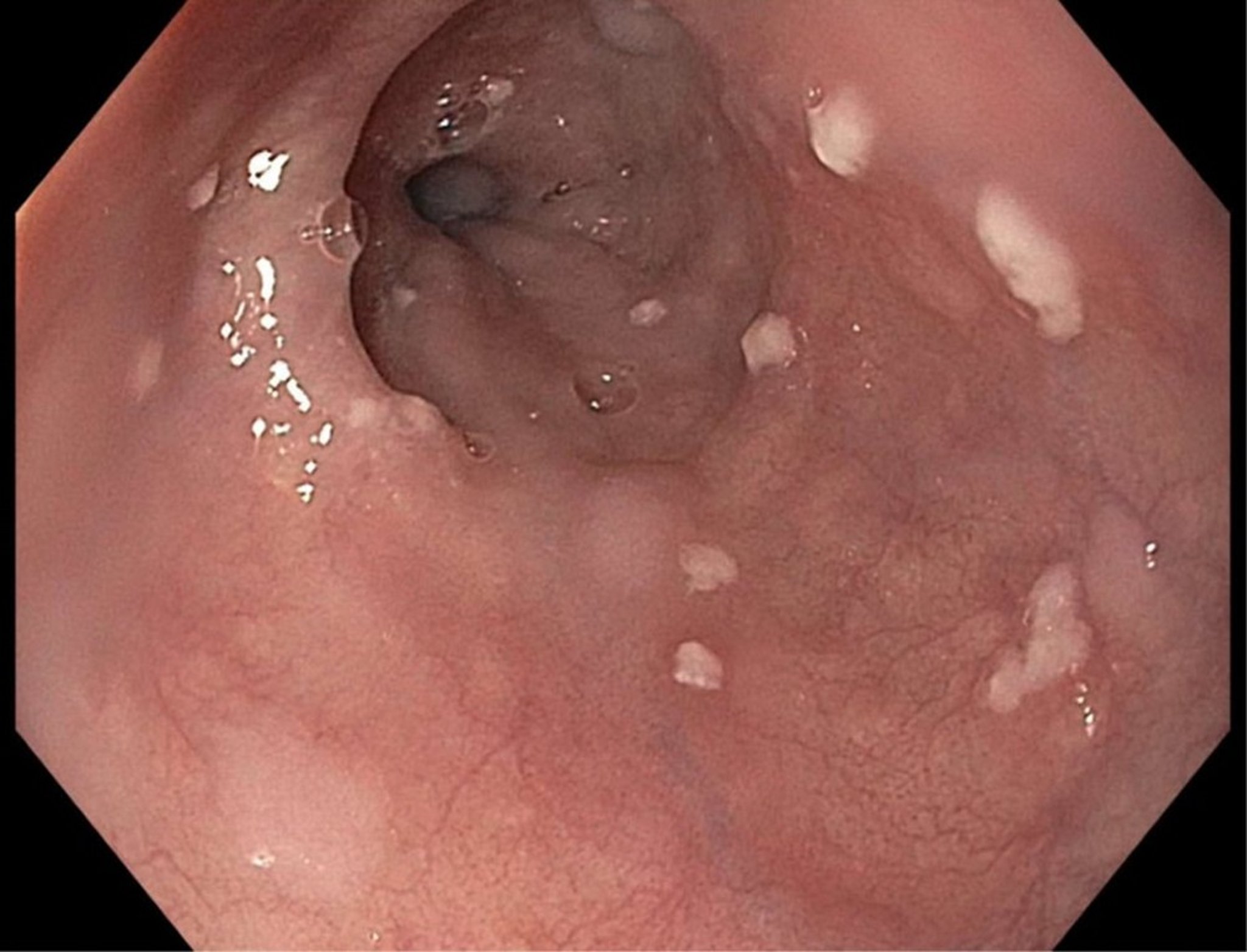
Diffuse whitish plaques are typical of Candida esophagitis.
Image provided by Kristle Lynch, MD.
Treatment of Candida esophagitis is with fluconazole 200 to 400 mg orally or IV once a day for 14 to 21 days (3). Alternatives include other azoles (eg, itraconazole, voriconazole, posaconazole) or echinocandins (eg, caspofungin, micafungin, anidulafungin). Topical therapy has no role in treatment of Candida esophagitis. Suppressive therapy is recommended for recurrent Candida esophagitis.
Candida esophagitis references
1. O'Rourke A. Infective oesophagitis: epidemiology, cause, diagnosis and treatment options. Curr Opin Otolaryngol Head Neck Surg. 2015;23(6):459-463. doi:10.1097/MOO.0000000000000199
2. Reddy CA, McGowan E, Yadlapati R, Peterson K. AGA Clinical Practice Update on Esophageal Dysfunction Due to Disordered Immunity and Infection: Expert Review. Clin Gastroenterol Hepatol. 2024;22(12):2378-2387. doi:10.1016/j.cgh.2024.08.027
3. Pappas PG, Kauffman CA, Andes DR, et al. Clinical Practice Guideline for the Management of Candidiasis: 2016 Update by the Infectious Diseases Society of America. Clin Infect Dis. 2016;62(4):e1-e50. doi: 10.1093/cid/civ933
Herpes Simplex Virus Esophagitis and Cytomegalovirus Esophagitis
In patients who have undergone solid organ transplantation, HSV esophagitis occurs within weeks after transplantation and CMV esophagitis occurs within months (1). Both can occur in patients with HIV or other forms of immunosuppression; HSV tends to exhibit more and smaller focal ulcerations, while CMV has fewer, larger lesions (2). Severe odynophagia results from either infection.


Multiple discrete, shallow, well-circumscribed ulcerations of herpes simplex virus esophagitis are noted on these endoscopic images.
Image provided by Kristle Lynch, MD.
Endoscopy, with cytology or biopsy, is usually necessary for diagnosis.
HSV is treated with oral or IV acyclovir, valacyclovir, or famciclovir. Patients with immunocompromise are usually treated for a longer duration (21 days) than those who are not (up to 10 days) (2).
CMV is usually treated with IV ganciclovir or oral valganciclovir, for up to 6 weeks in patients with immunocompromise (2). Alternatives include foscarnet and cidofovir.
HSV esophagitis and CMV esophagitis references
1. Tabbara IA, Zimmerman K, Morgan C, Nahleh Z. Allogeneic hematopoietic stem cell transplantation: complications and results. Arch Intern Med. 2002;162(14):1558-1566. doi:10.1001/archinte.162.14.1558
2. Reddy CA, McGowan E, Yadlapati R, Peterson K. AGA Clinical Practice Update on Esophageal Dysfunction Due to Disordered Immunity and Infection: Expert Review. Clin Gastroenterol Hepatol. 2024;22(12):2378-2387. doi:10.1016/j.cgh.2024.08.027
Drug Information for the Topic





