

An esophageal diverticulum is an outpouching of mucosa through the muscular layer of the esophagus. It can be asymptomatic or cause dysphagia and regurgitation. Diagnosis is made by barium swallow and sometimes endoscopy; surgical repair is rarely required.

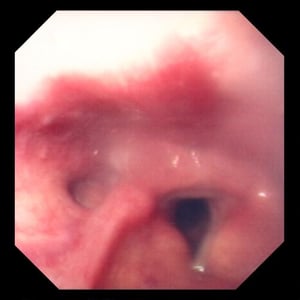
Zenker diverticula are posterior outpouchings of mucosa and submucosa through the cricopharyngeal muscle. In this image, the diverticulum is on the left, next to the triangular opening of the trachea formed by the vocal cords.
Zenker diverticula are posterior outpouchings of mucosa and submucosa through the cricopharyngeal muscle. In this image
Image provided by David M. Martin, MD.
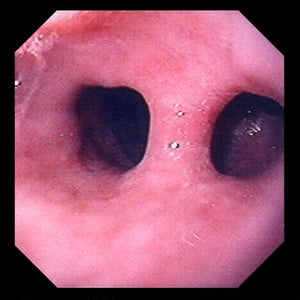
Traction diverticula are midesophageal outpouchings of mucosa and submucosa caused by motility disorders or by traction resulting from mediastinal processes. In this image, the diverticulum is to the right of the esophagus and gives the appearance of a double lumen.
Traction diverticula are midesophageal outpouchings of mucosa and submucosa caused by motility disorders or by traction
Image provided by David M. Martin, MD.
Zenker diverticula are posterior outpouchings of mucosa and submucosa through the cricopharyngeal muscle. In this image, the diverticulum is on the left, next to the triangular opening of the trachea formed by the vocal cords.
Zenker diverticula are posterior outpouchings of mucosa and submucosa through the cricopharyngeal muscle. In this image
Image provided by David M. Martin, MD.
Traction diverticula are midesophageal outpouchings of mucosa and submucosa caused by motility disorders or by traction resulting from mediastinal processes. In this image, the diverticulum is to the right of the esophagus and gives the appearance of a double lumen.
Traction diverticula are midesophageal outpouchings of mucosa and submucosa caused by motility disorders or by traction
Image provided by David M. Martin, MD.
There are several types of esophageal diverticula, each of different origin:
Zenker (pharyngeal) diverticula are posterior outpouchings of mucosa and submucosa through the cricopharyngeal muscle, probably resulting from an incoordination between pharyngeal propulsion and cricopharyngeal relaxation.
Midesophageal traction (Rokitansky) diverticula are caused by traction resulting from mediastinal inflammatory lesions or, secondarily, by esophageal motility disorders. Historically, they were associated with pulmonary tuberculosis.
Epiphrenic diverticula occur just above the diaphragm and usually accompany a motility disorder (eg, achalasia, distal esophageal spasm).
Symptoms and Signs of Esophageal Diverticula
Symptoms of esophageal diverticula include dysphagia, chest pain, and regurgitation (1).
A Zenker diverticulum fills with food that might be regurgitated when the patient bends or lies down. Aspiration pneumonitis may result if regurgitation is nocturnal. Rarely, the pouch becomes large, causing dysphagia and sometimes a palpable neck mass.
Traction and epiphrenic diverticula are rarely symptomatic, although their underlying cause may be.
Symptoms and signs reference
1. Constantin A, Constantinoiu S, Achim F, Socea B, Costea DO, Predescu D. Esophageal diverticula: from diagnosis to therapeutic management-narrative review. J Thorac Dis. 2023;15(2):759-779. doi:10.21037/jtd-22-861
Diagnosis of Esophageal Diverticula
Barium swallow
Sometimes endoscopy
Esophageal diverticula are diagnosed by barium swallow and often confirmed on upper endoscopy.
Treatment of Esophageal Diverticula
Usually none
Sometimes surgical resection or endoscopic treatment
Specific treatment is usually not required, although resection is occasionally necessary for large or symptomatic diverticula.
Diverticula associated with motility disorders require treatment of the primary disorder. For example, cricopharyngeal myotomy along with open diverticulectomy is used for Zenker diverticula (1). There are also endoscopic treatment options for diverticulectomy; for example, an endoscopic diverticulectomy for Zenker diverticula, or myotomy for achalasia with an epiphrenic diverticulum (2).
Treatment references
1. Bhatt NK, Mendoza J, Kallogjeri D, Hardi AC, Bradley JP. Comparison of Surgical Treatments for Zenker Diverticulum: A Systematic Review and Network Meta-analysis. JAMA Otolaryngol Head Neck Surg. 2021;147(2):190-196. doi:10.1001/jamaoto.2020.4091
2. Sato H, Takeuchi M, Hashimoto S, et al. Esophageal diverticulum: New perspectives in the era of minimally invasive endoscopic treatment. World J Gastroenterol. 2019;25(12):1457-1464. doi:10.3748/wjg.v25.i12.1457





