

Renal cortical necrosis is destruction of cortical tissue resulting from renal arteriolar injury and leading to acute kidney injury. This rare disorder typically occurs in neonates and in pregnant or postpartum patients when sepsis or pregnancy complications occur. Symptoms and signs include gross hematuria, flank pain, decreased urine output, fever, and symptoms of uremia. Symptoms of the underlying disorder may predominate. Diagnosis is by ultrasound, CT, or renal biopsy. Mortality rate at 1 year is > 20%. Treatment is directed at the underlying disorder and at preserving kidney function.
In renal cortical necrosis, which may be patchy or diffuse, bilateral renal arteriolar injury results in destruction of cortical tissues and acute kidney injury. Renal cortical tissues eventually calcify. The juxtamedullary cortex, medulla, and the area just under the capsule are spared.
Etiology of Renal Cortical Necrosis
Injury usually results from reduced renal artery perfusion secondary to vascular spasm, microvascular injury, or intravascular coagulation.
Renal cortical necrosis can occur but is uncommon in infants and children. Pregnancy complications, especially placental abruption, increase risk of this disorder in neonates and in women, as does sepsis. Other causes (eg, disseminated intravascular coagulation [DIC]) are less common (see table ).
Causes of Renal Cortical Necrosis
Patient Group | Causes |
|---|---|
Neonates | Placental abruption (causes about 50% of cases) Congenital heart disease (severe) Dehydration Fetomaternal transfusion Perinatal asphyxia |
Children | Dehydration |
Pregnant and postpartum women | Pregnancy complications (cause > 50% of cases among women): Placental abruption, amniotic fluid embolism, intrauterine fetal death, placenta previa, preeclampsia, puerperal sepsis, uterine hemorrhage Sepsis (causes about 30%) |
Others | Burns Disseminated intravascular coagulation Drugs and medications (eg, nonsteroidal anti-inflammatory drugs) Hyperacute renal allograft rejection Incompatible blood transfusion Nephrotoxic contrast agents Poisoning (eg, phosphorus, arsenic) Trauma |
Symptoms and Signs of Renal Cortical Necrosis
Gross hematuria, flank pain, and sometimes decreased urine output or abrupt anuria occur. Fever is common, and hypertension will occur as chronic kidney disease develops. However, these symptoms and signs are often overshadowed by symptoms of the underlying disorder.
Diagnosis of Renal Cortical Necrosis
Imaging study or renal biopsy
Diagnosis is suspected when typical symptoms occur in patients with a potential cause.
The diagnosis can usually be established by ultrasound or CT. Renal biopsy is performed only if the diagnosis is unclear and no contraindications exist. It provides definitive diagnosis and prognostic information.
Urinalysis, complete blood count (CBC), serum electrolytes, liver tests, and kidney function tests are done. These tests may confirm renal dysfunction (eg, by elevated creatinine, blood urea nitrogen, and potassium) and suggest a cause. Severe electrolyte abnormalities may be present depending on the cause (eg, hyperkalemia, hyperphosphatemia, hypocalcemia). CBC often detects leukocytosis (even when sepsis is not the cause) and may detect anemia and thrombocytopenia if hemolysis, disseminated intravascular coagulation (DIC), or sepsis is the cause. Transaminases may be increased in relative hypovolemic states (eg, septic shock, postpartum hemorrhage). If DIC is suspected, coagulation studies are done. They may detect low fibrinogen levels, increased fibrin-degradation products, and increasing prothrombin time (PT)/INR and partial thromboplastin time (PTT). Urinalysis typically detects proteinuria and hematuria.

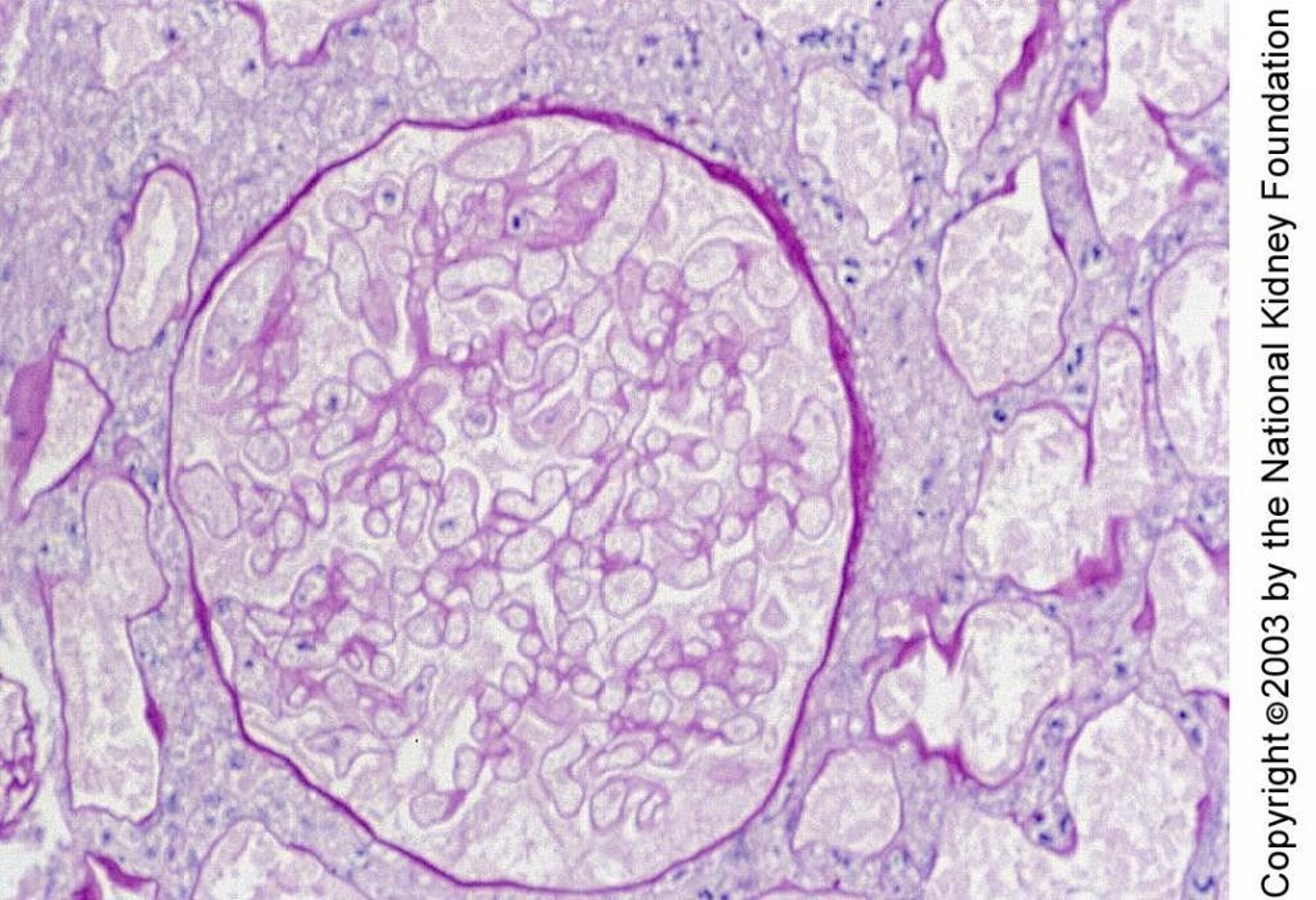
Renal cortical necrosis is characterized histologically by necrosis of glomeruli and tubules. Necrosis in this biopsy specimen is manifest by small nuclei and ghostlike outlines of cells (periodic acid-Schiff stain, × 400).
Image provided by Agnes Fogo, MD, and the American Journal of Kidney Diseases' Atlas of Renal Pathology (see www.ajkd.org).
Treatment of Renal Cortical Necrosis
Treatment of underlying disorder
Preservation of kidney function
Treatment is directed at the underlying disorder and at preserving renal function (eg, early dialysis).
Prognosis for Renal Cortical Necrosis
With aggressive supportive therapy, 1-year mortality is about 20%, and up to 20% of survivors may recover some kidney function (1).
Prognosis reference
1. Prakash J, Vohra R, Wani IA, et al. Decreasing incidence of renal cortical necrosis in patients with acute renal failure in developing countries: a single-centre experience of 22 years from Eastern India. Nephrol Dial Transplant 2007;22(4):1213-1217. doi:10.1093/ndt/gfl761
Key Points
Renal cortical necrosis is rare, often occurring in neonates and in pregnant or postpartum patients with sepsis or pregnancy complications.
Suspect the diagnosis in patients at risk who develop typical symptoms (eg, gross hematuria, flank pain, decreased urine output, fever, hypertension).
Confirm the diagnosis with renal imaging or renal biopsy.
Treat the underlying disorder.





