



Deep venous thrombosis (DVT) is clotting of blood in a deep vein of an extremity (usually calf or thigh) or the pelvis. DVT is the primary cause of pulmonary embolism. DVT results from conditions that impair venous return, lead to endothelial injury or dysfunction, or cause hypercoagulability. DVT may be asymptomatic or cause pain and swelling in an extremity; pulmonary embolism is an immediate complication. Diagnosis is by history, physical examination, and testing, typically with duplex ultrasound. D-Dimer testing is sometimes used when DVT is suspected; a negative result helps to exclude DVT, whereas a positive result is nonspecific and requires additional testing to confirm DVT. Treatment is with anticoagulants. Prognosis is generally good with prompt, adequate treatment. Common long-term complications include venous insufficiency with or without the post-thrombotic syndrome.
DVT occurs most commonly in the lower extremities or pelvis (see figure ). DVT is less common in deep veins of the upper extremities (< 5% of DVT cases) (1).
Deep Veins of the Legs

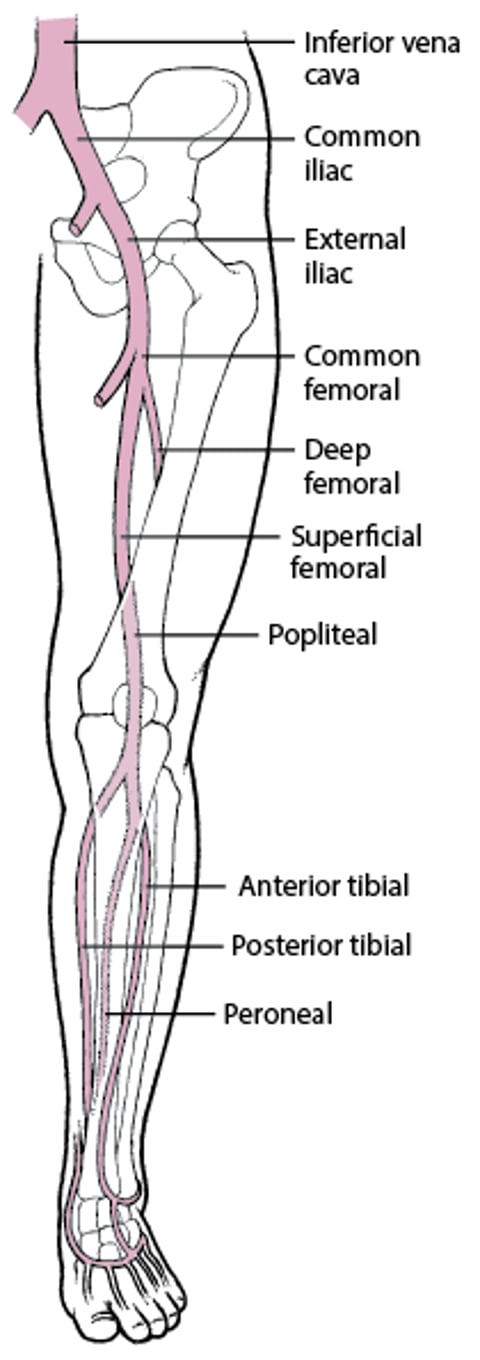
Lower extremity DVT is much more likely to cause pulmonary embolism (PE) than upper extremity DVT, possibly because of the higher clot burden (2). Most proximal DVTs involve the femoral or popliteal veins and up to 38% extend more proximally to involve the iliofemoral veins (2, 3, 4). DVT of the distal or calf veins usually involves the posterior tibial or peroneal veins. Distal or calf vein DVT is less likely to be a source of large emboli but can propagate to the proximal thigh veins and from there cause PE. Approximately 50% of patients with DVT have occult PE, and at least 30% of patients with PE have demonstrable DVT (5).
Pearls & Pitfalls
|
General references
1. Yamashita Y, Morimoto T, Amano H, et al. Deep vein thrombosis in upper extremities: Clinical characteristics, management strategies and long-term outcomes from the COMMAND VTE Registry. Thromb Res. 2019;177:1-9. doi:10.1016/j.thromres.2019.02.029
2. Freund Y, Cohen-Aubart F, Bloom B. Acute Pulmonary Embolism: A Review. JAMA. 2022;328(13):1336-1345. doi:10.1001/jama.2022.16815
3. Broholm R, Bækgaard N, Hansen S, et al. Significance of Partial or Complete Thrombosis of the Common and Deep Femoral Vein in Patients With Deep Vein Thrombosis. Eur J Vasc Endovasc Surg. 2019;58(4):570-575. doi:10.1016/j.ejvs.2019.06.016
4. De Maeseneer MG, Bochanen N, van Rooijen G, Neglén P. Analysis of 1,338 Patients with Acute Lower Limb Deep Venous Thrombosis (DVT) Supports the Inadequacy of the Term "Proximal DVT". Eur J Vasc Endovasc Surg. 2016;51(3):415-420. doi:10.1016/j.ejvs.2015.11.001
5. Stevens SM, Woller SC, Kreuziger LB, et al. Antithrombotic Therapy for VTE Disease: Second Update of the CHEST Guideline and Expert Panel Report [published correction appears in Chest. 2022 Jul;162(1):269]. Chest. 2021;160(6):e545-e608. doi:10.1016/j.chest.2021.07.055
Etiology of Deep Venous Thrombosis
Many factors can contribute to DVT (see table ). Cancer is a risk factor for DVT, particularly in older patients and in patients with recurrent thrombosis. Among all patients with cancer, approximately 1 to 5% develop a venous thromboembolism (VTE) annually (1, 2, 3). The association is strongest for pancreatic, brain, hematologic, lung, and ovarian cancers (2, 4). Occult cancers may be present in patients with apparently idiopathic DVT, but extensive evaluation patients for tumors is not recommended unless patients have risk factors for specific cancers or symptoms suggestive of an occult cancer (5).
Etiology references
1. Horsted F, West J, Grainge MJ. Risk of venous thromboembolism in patients with cancer: a systematic review and meta-analysis. PLoS Med. 2012;9(7):e1001275. doi:10.1371/journal.pmed.1001275
2. Martens KL, Li A, La J, et al. Epidemiology of Cancer-Associated Venous Thromboembolism in Patients With Solid and Hematologic Neoplasms in the Veterans Affairs Health Care System. JAMA Netw Open. 2023;6(6):e2317945. doi:10.1001/jamanetworkopen.2023.17945
3. Mulder FI, Horváth-Puhó E, van Es N, et al. Venous thromboembolism in cancer patients: a population-based cohort study. Blood. 2021;137(14):1959-1969. doi:10.1182/blood.2020007338
4. Betts MB, Liu X, Junqueira DR, et al. Risk of Venous Thromboembolism by Cancer Type: A Network Meta-Analysis. Semin Thromb Hemost. 2024;50(3):328-341. doi:10.1055/s-0044-1779672
5. D'Astous J, Carrier M. Screening for Occult Cancer in Patients with Venous Thromboembolism. J Clin Med. 2020;9(8):2389. Published 2020 Jul 27. doi:10.3390/jcm9082389
Pathophysiology of Deep Venous Thrombosis
Classically, thrombosis occurs due to a combination of impaired blood flow (stasis), endothelial injury, and hypercoagulability (Virchow triad).
Deep venous thrombosis (DVT) usually begins in venous valve cusps. Thrombi consist of thrombin, fibrin, and red blood cells with relatively few platelets (red thrombi); without treatment, thrombi may propagate proximally to the lungs.
Lower extremity DVT most often results from:
Impaired venous return (eg, in immobilized patients)
Endothelial injury or dysfunction (eg, after leg fractures)
Hypercoagulability
Upper extremity DVT most often results from (1):
Endothelial injury due to central venous catheters, pacemakers, or injection drug use
Upper extremity DVT occasionally occurs as part of superior vena cava (SVC) syndrome (compression or invasion of the superior vena cava by a tumor and causing symptoms such as facial swelling, dilated neck veins, and facial flushing) or results from a hypercoagulable state or subclavian vein compression at the thoracic outlet (1). The compression may be due to a normal or an accessory first rib or fibrous band (thoracic outlet syndrome) or occur during strenuous arm activity (effort thrombosis, or Paget-Schroetter syndrome, which is rare).
Complications
Common complications of DVT include:
Post-thrombotic syndrome (chronic venous insufficiency )
Much less commonly, acute massive DVT leads to phlegmasia alba dolens or phlegmasia cerulea dolens, both of which, unless promptly diagnosed and treated, can result in venous gangrene.
In phlegmasia alba dolens, a rare complication of DVT during pregnancy, the leg turns milky white or paler than the surrounding skin. Pathophysiology is unclear, but edema may increase soft-tissue pressure beyond capillary perfusion pressures, resulting in tissue ischemia and venous gangrene. Phlegmasia alba dolens may progress to phlegmasia cerulea dolens.
In phlegmasia cerulea dolens, massive iliofemoral venous thrombosis causes near-total venous occlusion; the leg becomes ischemic, extremely painful, and cyanotic or violaceous. Pathophysiology may involve complete stasis of venous and arterial blood flow in the lower extremity because venous return is occluded or massive edema cuts off arterial blood flow. Venous gangrene may result.
Infection rarely develops in venous clots. Jugular vein suppurative thrombophlebitis (Lemierre syndrome), a bacterial (usually anaerobic) infection of the internal jugular vein and surrounding soft tissues, may follow tonsillopharyngitis and is often complicated by bacteremia and sepsis. In septic pelvic thrombophlebitis, pelvic thromboses develop postpartum and become infected, causing intermittent fever. Suppurative (septic) thrombophlebitis, a bacterial infection of a superficial peripheral vein, comprises infection and clotting and usually is caused by venous catheterization.
Pathophysiology reference
1. Bosch FTM, Nisio MD, Büller HR, van Es N. Diagnostic and Therapeutic Management of Upper Extremity Deep Vein Thrombosis. J Clin Med. 2020;9(7):2069. doi:10.3390/jcm9072069
Symptoms and Signs of Deep Venous Thrombosis
DVT may occur in ambulatory patients or as a complication of surgery or major medical illness. Among patients who are hospitalized and are at high risk, deep vein thrombosis is often asymptomatic since typical features of swelling, redness, and tenderness may be less prominent in recumbent than ambulatory patients.
When present, symptoms and signs of DVT (eg, vague aching pain, tenderness along the distribution of the veins, edema, erythema) are nonspecific, vary in frequency and severity, and are similar in arms and legs. Dilated collateral superficial veins may become visible or palpable. Calf discomfort elicited by ankle dorsiflexion with the knee extended (Homans sign) occasionally occurs with distal leg DVT but is neither sensitive nor specific. Tenderness, swelling of the whole leg, > 3 cm difference in circumference between calves, pitting edema, and collateral superficial veins may be most specific; DVT is likely with a combination of ≥ 3 in the absence of another likely diagnosis (see table ).
Low-grade fever may be present; DVT may be the cause of fever without an obvious source, especially in postoperative patients. Symptoms of pulmonary embolism, if it occurs, may include shortness of breath and pleuritic chest pain.
Wells Score: Probability of Deep Venous Thrombosis Based on Clinical Factors
Factors |
Tenderness along distribution of the veins in calf or thigh |
Swelling of entire leg |
Calf swelling (> 3 cm difference in circumference between calves, measured 10 cm below the tibial tuberosity) |
Pitting edema greater in affected leg |
Dilated collateral superficial veins |
Active cancer (treatment ongoing or given within the previous 6 months) |
Immobilization of lower extremity (eg, due to paralysis, paresis, casting, or recent long-distance travel) |
Surgery leading to immobility for > 3 days within the past 4 weeks |
Previous DVT |
Probability |
Probability equals the number of factors, subtracting 2 if another diagnosis is as likely as or more likely than deep venous thrombosis.
|
Based on Wells PS, Owen C, Doucette S, Fergusson D, Tran H. Does this patient have deep vein thrombosis? JAMA. 2006;295(2):199-207. doi: 10.1001/jama.295.2.199 and Scarvelis D, Wells PS. Diagnosis and treatment of deep-vein thrombosis. CMAJ. 2006;175(9):1087-1092. doi: 10.1503/cmaj.060366 |
Common causes of asymmetric leg swelling that mimic DVT are:
Soft-tissue trauma
Compression of a pelvic vein
Obstruction of a lymphatic vessel in the pelvis
Popliteal cyst (including Baker cyst) that obstructs venous return
Less common causes include abdominal or pelvic tumors that obstruct venous or lymphatic return.
Symmetric bilateral leg swelling is the typical result of use of medications that cause dependent edema (eg, dihydropyridine calcium channel blockers, estrogen, high-dose opioids), venous hypertension (usually due to right heart failure), and hypoalbuminemia; however, such swelling may be asymmetric if venous insufficiency coexists and is worse in one leg.
Common causes of calf pain that mimic acute DVT include:
Cellulitis that causes painful erythema of the calf
Ruptured popliteal cyst (pseudo-DVT), which causes calf swelling, pain, and sometimes bruising in the region of the medial malleolus
Partial or complete tears of the calf muscles or tendons
Diagnosis of Deep Venous Thrombosis
Ultrasound
Sometimes D-dimer testing
History and physical examination help determine probability of DVT before testing (see table ). Diagnosis is typically by ultrasound with Doppler flow studies (duplex ultrasound). The need for additional tests (eg, D-dimer testing) and their choice and sequence depend on pretest probability and sometimes ultrasound results. (See figure .)
One Approach to Testing for Suspected Deep Venous Thrombosis (DVT)
* Based on a clinical decision tool such as the Wells criteria. † The age-adjusted D-dimer threshold is calculated as the patient’s age multiplied by 10 ng/mL (10 mcg/L) and is used for patients > 50 years with suspected venous thromboembolism. Data from Chopard R, Albertsen IE, Piazza G. Diagnosis and Treatment of Lower Extremity Venous Thromboembolism: A Review. JAMA. 2020;324(17):1765-1776. doi:10.1001/jama.2020.17272 |


No single testing protocol is best; one approach is for clinicians to first estimate the probability of a DVT using a validated clinical prediction rule such as the Wells score (1). In patients with a low probability, a negative D-dimer is considered sufficient to exclude DVT and avoid further imaging (2, 3). In patients with a high probability estimated by the clinical prediction rule, or those with a positive D-dimer, compression ultrasound is used to diagnose (or exclude) DVT (4).

Ultrasound

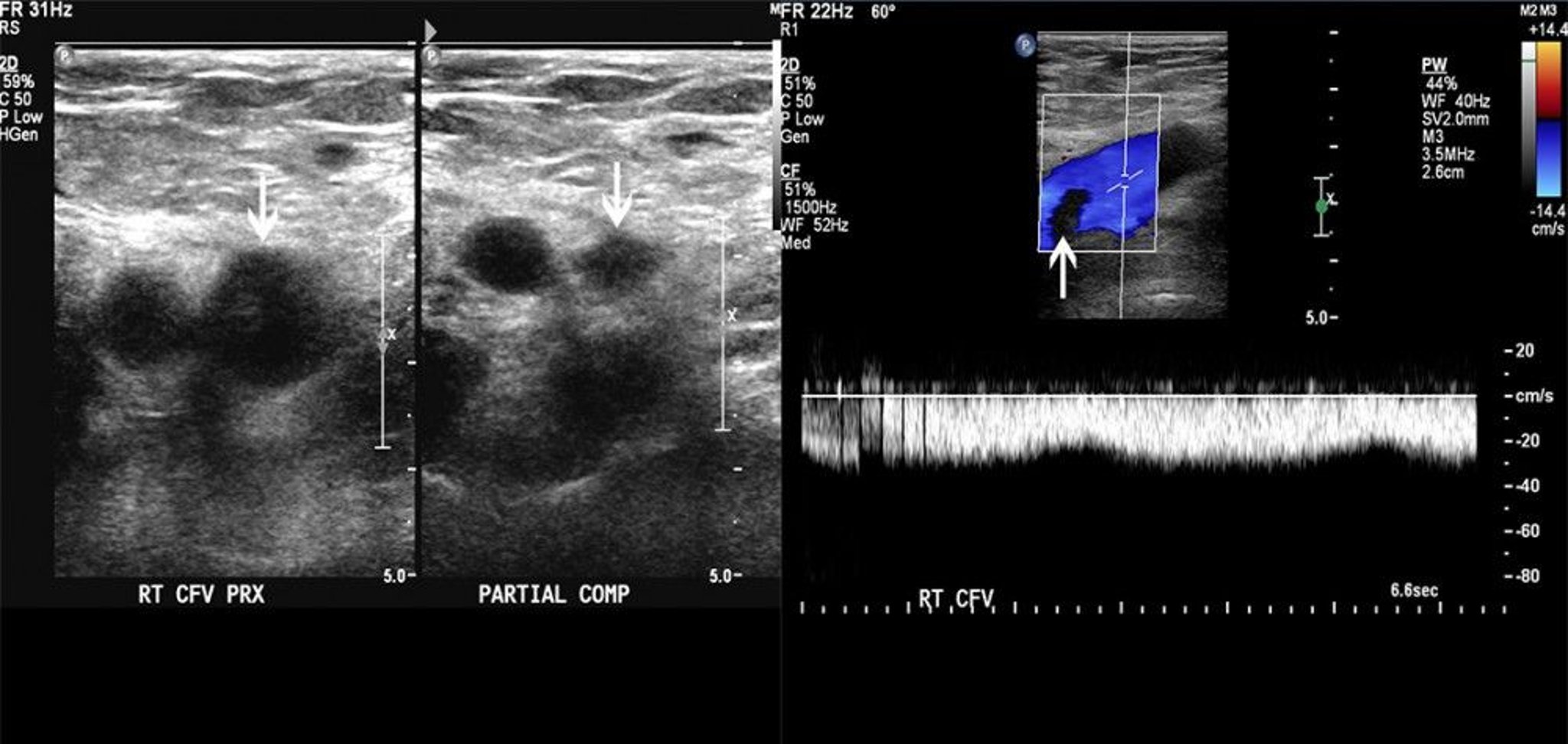
The image on the left shows partial compressibility of the common femoral vein (arrows). The image on the right shows a filling defect on color Doppler flow. These findings are consistent with thrombus.
© 2017 Elliot K. Fishman, MD.
Ultrasound identifies thrombi by directly visualizing the venous lining and by demonstrating abnormal vein compressibility or, with Doppler flow studies, impaired venous flow. The test is approximately 90% sensitive and 98% specific for lower extremity DVT (5).
D-Dimer
D-Dimer is a byproduct of fibrinolysis; elevated levels suggest recent presence and lysis of thrombi. In contrast to compression ultrasound, D-dimer is highly sensitive (sensitivity approximately 96%) but nonspecific (specificity approximately 37%) (4). A positive test result is nonspecific because levels can be elevated by other conditions (eg, liver disease, trauma, pregnancy, positive rheumatoid factor, inflammation, recent surgery, cancer), and further testing is necessary. D-dimer levels also increase with age, which further decreases the specificity in older patients (6).
Alternative imaging
Contrast-enhanced computed tomographic venography and magnetic resonance venography are other imaging modalities, generally reserved for cases in which ultrasound results are negative or indeterminate and the clinical suspicion for DVT remains high. These imaging tests are less well validated for DVT, are more costly, and may be associated with other complications (eg, related to exposure to radiation and contrast agents).
Testing for pulmonary embolism
If symptoms and signs suggest PE, additional imaging (eg, CT pulmonary angiography or, less often, ventilation/perfusion [V/Q] scanning) is required. For more detail, see Pulmonary Embolism.
Determination of cause
Patients with confirmed DVT and an obvious risk factor (eg, immobilization, surgical procedure, leg trauma), as well as most patients with a first unprovoked DVT need no further testing.
Patients in whom testing to detect thrombophilia may be useful to guide duration of treatment include (7):
Patients with recurrent unprovoked thrombosis
Patients with unprovoked thrombosis at an unusual site (e.g., splanchnic, cerebral sinus)
Women who develop thrombosis within 6 months of starting hormonal therapy (eg, oral contraceptives)
Some evidence suggests that testing for the presence of hypercoagulability in patients with or without clinical risk factors does not predict DVT recurrence (8, 9, 10).
Screening patients with DVT for cancer has a low yield (11). Selective testing guided by complete history and physical examination and basic "routine" tests (complete blood count, chest radiograph, urinalysis, liver enzymes, serum electrolytes, blood urea nitrogen [BUN], creatinine) aimed at detecting cancer is probably adequate. In addition, patients should have any appropriate cancer screening (eg, mammography, colonoscopy) that is due.
Treatment of Deep Venous Thrombosis
Anticoagulation
Sometimes thrombolytic therapy, surgery, or inferior vena cava filter
It is preferable and safer to prevent DVT than to treat it, particularly in patients who are at high risk. For a complete discussion, see DVT Prevention.
Treatment is aimed primarily at pulmonary embolism prevention and secondarily at symptom relief and prevention of DVT recurrence, chronic venous insufficiency, and post-thrombotic syndrome. Treatment of lower and upper extremity DVT is generally the same.
General supportive measures include pain control with analgesics, which may include short (3- to 5-day) courses of a nonsteroidal anti-inflammatory drug (NSAID). Extended treatment with NSAIDs and aspirin should be avoided because their antiplatelet effects may increase the risk of bleeding complications. In addition, elevation of legs (supported by a pillow or other soft surface to avoid venous compression) is recommended during periods of inactivity (1). Patients may be as physically active as they can tolerate; there is no evidence that early activity increases risk of clot dislodgement and PE and may help to reduce the risk of the post-thrombotic syndrome (2).
Anticoagulation strategies for DVT
(For details on specific medications and their complications, see Medications for Deep Venous Thrombosis.)
There are several strategies for anticoagulation of patients with DVT:
Initial treatment with an injectable heparin (unfractionated or low molecular weight) followed after several days by long-term treatment with an oral medication (warfarin, a factor Xa inhibitor, or a direct thrombin inhibitor)
Initial and long-term treatment with a low molecular weight heparin (LMWH)
Initial and long-term treatment with certain oral factor Xa inhibitors (rivaroxaban or apixaban)
Almost all patients with DVT are treated with anticoagulants (3, 4). The exception is patients with isolated distal thrombi without severe symptoms, in whom serial imaging and anticoagulation are needed only if the thrombus extends. Various anticoagulants are suitable for initial therapy, and the choice of agent is influenced by patient comorbidities (eg, renal dysfunction, cancer), preferences, cost, and convenience.
Inadequate anticoagulation in the first 24 to 48 hours may increase risk of recurrence or of PE. Acute DVT can be treated on an outpatient basis unless severe symptoms require parenteral analgesics, other disorders preclude safe outpatient discharge, or other factors (eg, functional, socioeconomic) might prevent the patient from adhering to prescribed treatments. Dosing regimens for treatment of DVT differ from those used for prevention of thromboembolism in patients with atrial fibrillation.
Appropriate treatment with anticoagulation, particularly warfarin with close international normalized ratio (INR) monitoring, reduces but does not eliminate the risk of post-thrombotic syndrome (5).
Direct Oral Anticoagulants
Direct oral anticoagulants (DOAC), including apixaban, dabigatran, edoxaban, and rivaroxaban, are preferred over warfarin as first-line treatment for DVT and PE, including cancer-associated thromboses. (see table ) (3, 4, 6). Compared to warfarin, these medications have been shown to give similar protection against recurrent DVT and have similar (or with apixaban, perhaps lower) risk of serious bleeding (3). Also, they are given as a fixed dose and thus, unlike warfarin, do not require ongoing laboratory testing. The main disadvantage is the higher cost compared to warfarin and the high cost of DOAC reversal agents in the case of bleeding or need for an urgent surgery or procedure.
For patients who are to start edoxaban (an oral factor Xa inhibitor) or dabigatran (an oral direct thrombin inhibitor), the oral agent is started after 5 days of injectable heparin (7). Alternatively, selected direct oral anticoagulants (rivaroxaban or apixaban) may be initiated immediately without first giving an injectable heparin.
Warfarin
Some patients are initially given an injectable heparin (typically low molecular weight) for 5 to 7 days, followed by longer term treatment with warfarin, which is started within 24 hours after the start of the injectable heparin. Although heparin acts rapidly and provides immediate anticoagulation, warfarin takes about 5 days to achieve a therapeutic effect; hence, heparin is required for 5 to 7 days. Warfarin is the recommended approach for patients with antiphospholipid syndrome (4).
Low molecular weight heparin
For selected patients (eg, with extensive iliofemoral DVT or cancer), continued treatment with a low-molecular-weight heparin rather than switching to an oral agent may be preferred (6).
Fondaparinux, a parenteral factor Xa inhibitor, is sometimes substituted for low molecular weight heparin and can also be used to treat acute DVT.
Duration of Treatment
The initial duration of anticoagulation is 3 to 6 months (3, 4). Patients with transient risk factors for DVT (eg, immobilization, surgery) can usually discontinue anticoagulation after 3 to 6 months. Patients with idiopathic (or unprovoked) DVT with no known risk factors, recurrent DVT, or DVT due to a chronic and persistent risk factor (including cancer and hypercoagulable states such as antiphospholipid syndrome or protein C, protein S, or antithrombin deficiency) should continue anticoagulation indefinitely (extended anticoagulation) for secondary prevention of recurrent DVT and prevention of PE, with periodic re-evaluation of risks and benefits. In some patients, lifelong anticoagulation is needed.
For selected patients who require extended anticoagulation, reduced-dose apixaban or rivaroxaban regimens may be considered. The use of reduced-dose apixaban for patients with cancer-associated DVT and reduced-dose rivaroxaban for patients at high risk for DVT recurrence appear to be as effective as full-dose regimens for extended anticoagulation, while also conferring a lower risk of significant bleeding (1, 8, 9).
Inferior vena cava (IVC) filter
An IVC filter may help prevent PE in patients with lower extremity DVT who have contraindications to anticoagulant therapy (3, 4). An IVC filter is placed in the inferior vena cava just below the renal veins via catheterization of an internal jugular or femoral vein. Some IVC filters are retrievable and can be used temporarily (eg, until contraindications to anticoagulation resolve).


This CT scan shows an implanted IVC filter.
ZEPHYR/SCIENCE PHOTO LIBRARY
Although IVC filters reduce the risk of acute pulmonary embolism after DVT, they do not reduce mortality and do increase the risk of subsequent DVT, as well as other longer-term complications (eg, venous collaterals can develop, providing a pathway for emboli to circumvent the filter) (4, 10). There is also an increased risk of recurrent DVT. Also, IVC filters can dislodge or become obstructed by a clot. A clotted filter may cause bilateral lower extremity venous congestion (including acute phlegmasia cerulea dolens), lower body ischemia, and acute kidney injury. Treatment for a dislodged filter is removal, using angiographic or, if necessary, surgical methods.
Thrombolytic (fibrinolytic) therapy
Thrombolytic medications, which include alteplase, tenecteplase, and streptokinase, lyse clots and may be more effective than anticoagulation alone in selected patients, but the risk of bleeding is higher than with heparin. Consequently, thrombolytics should be considered only in highly selected patients with DVT, such as those < 60 years with extensive iliofemoral DVT who have evolving or existing limb ischemia (eg, phlegmasia cerulea dolens) and do not have risk factors for bleeding (3).
Catheter-directed thrombolysis has largely replaced systemic administration when used for DVT, and may be considered in some patients to help prevent post-thrombotic syndrome (5).
Surgery
Surgery is rarely needed. However, thrombectomy, fasciotomy, or both are mandatory for phlegmasia alba dolens or phlegmasia cerulea dolens unresponsive to thrombolytics to try to prevent limb-threatening gangrene.
Prognosis for Deep Venous Thrombosis
Even with treatment, lower extremity DVT can have approximately a < 1 to 2% risk of fatal PE (1, 2); death due to upper extremity DVT is very rare. Risk of recurrent DVT is lowest for patients with transient risk factors (eg, surgery, trauma, temporary immobility) and greatest for patients with persistent risk factors (eg, cancer), idiopathic DVT, or incomplete resolution of past DVT (residual thrombus). A normal D-dimer level obtained after anticoagulation is stopped for 3 to 4 weeks may help predict a relatively low risk of DVT or PE recurrence, more so in women than in men (3). Risk of venous insufficiency is difficult to predict. Risk factors for post-thrombotic syndrome include proximal (iliofemoral) thrombosis, recurrent ipsilateral DVT, increased body mass index, older age, and suboptimal anticoagulation (4).
Prognosis references
1. Douketis JD, Gu CS, Schulman S, Ghirarduzzi A, Pengo V, Prandoni P. The risk for fatal pulmonary embolism after discontinuing anticoagulant therapy for venous thromboembolism. Ann Intern Med. 2007;147(11):766-774. doi:10.7326/0003-4819-147-11-200712040-00007
2. Laporte S, Mismetti P, Décousus H, et al. Clinical predictors for fatal pulmonary embolism in 15,520 patients with venous thromboembolism: findings from the Registro Informatizado de la Enfermedad TromboEmbolica venosa (RIETE) Registry. Circulation. 2008;117(13):1711-1716. doi:10.1161/CIRCULATIONAHA.107.726232
3. Xu Y, Khan F, Kovacs MJ, et al. Serial D-dimers after anticoagulant cessation in unprovoked venous thromboembolism: Data from the REVERSE cohort study. Thromb Res. 2023;231:32-38. doi:10.1016/j.thromres.2023.09.012
4. Chopard R, Albertsen IE, Piazza G. Diagnosis and Treatment of Lower Extremity Venous Thromboembolism: A Review. JAMA. 2020;324(17):1765-1776. doi:10.1001/jama.2020.17272
Key Points
Symptoms and signs are nonspecific, so clinicians must be alert, particularly in high-risk patients.
Low-risk patients may have D-dimer testing, as a normal result essentially excludes deep venous thrombosis (DVT); others should have ultrasound.
Treatment initially is with an injectable heparin (unfractionated or low molecular weight heparin [LMWH]) followed by an oral anticoagulant (warfarin, dabigatran, or a factor Xa inhibitor) or a LMWH; alternatively, the oral factor Xa inhibitors rivaroxaban and apixaban may be used for initial and ongoing treatment.
Duration of treatment is typically 3 to 6 months, depending on the presence and nature of risk factors; certain patients require extended treatment.
Drug Information for the Topic





