



The esophageal-tracheal double lumen tube (eg, Combitube) and the laryngeal tube (eg, King) are supraglottic airway devices (also called retroglottic airway devices).
(See also Tracheal Intubation, Airway Establishment and Control and Airway and Respiratory Devices.)
The esophageal-tracheal double lumen tube and the laryngeal tube are twin-lumen tubes that have fundamental similarities:
A large, proximal balloon cuff seals the hypopharynx
A ventilating, proximal lumen terminates at side ports overlying the laryngeal inlet
A distal lumen and its smaller balloon cuff terminate in and seal the upper esophagus (in > 90% of insertions)
Supraglottic airways are useful for providing rescue ventilation to unconscious patients or patients without a gag reflex.
The esophageal-tracheal double lumen tube and laryngeal tube have some advantages over other methods of ventilation:
Unlike endotracheal tubes, they can be successfully inserted blindly and by operators with only basic training.
Unlike bag-valve-mask (BVM) ventilation, they avoid the difficulties of attaining and maintaining an adequate face-mask seal.
They cause less gastric insufflation or aspiration than BVM ventilation or laryngeal mask (LMA) ventilation because they better isolate the esophagus from the trachea and the distal lumen permits gastric tube insertion.
Like the other supraglottic airways, the esophageal-tracheal double lumen tube and laryngeal tube are temporary airways that must be removed or replaced by a definitive airway such as an endotracheal tube or surgical airway (cricothyrotomy or tracheostomy).
Indications for Esophageal-Tracheal Double Lumen Tube or Laryngeal Tube Insertion
Apnea, severe respiratory failure, or impending respiratory arrest in which endotracheal intubation cannot be accomplished
Situations where BVM ventilation is difficult or impossible (eg, in patients with severe facial deformity [traumatic or natural], thick beard, or other factors that interfere with the face mask seal and in patients with upper airway blockage due to obstructing soft tissues)
Contraindications to Esophageal-Tracheal Double Lumen Tube or Laryngeal Tube Insertion
Absolute contraindications:
There is no medical contraindication to providing ventilatory support to a patient; however, a legal contraindication (do-not-resuscitate order or specific advance directive) may be in force
Restricted mouth opening that blocks tube insertion (nasotracheal intubation or a surgical airway would be indicated in this case)
Impassable upper airway obstruction (surgical airway would be indicated in this case)
Relative contraindications:
Consciousness or presence of a gag reflex
Hypopharyngeal or esophageal abnormalities or trauma (which increase the risk of further local damage by a supraglottic airway)
Esophageal-tracheal double lumen tube is not recommended for patients < 4 feet (approximately 122 cm) tall; laryngeal tubes come in various sizes based on the patient's height starting at 4 to 5 feet (122 to 152 cm) in height.
Complications of Esophageal-Tracheal Double Lumen Tube or Laryngeal Tube Insertion
Complications include:
Vomiting and aspiration during tube insertion or after placement in patients who regain a gag reflex
Dental, oropharyngeal, or esophageal/aerodigestive soft tissue trauma during tube insertion
Tongue edema due to prolonged placement or balloon overinflation
Equipment for Esophageal-Tracheal Double Lumen Tube or Laryngeal Tube Insertion
Gloves, mask, gown, and eye protection (ie, universal precautions)
Syringes for balloon cuff inflation
Sterile water-soluble lubricant or anesthetic jelly
Esophageal-tracheal double lumen tube or laryngeal tube, appropriately sized to patient based on manufacturer's specifications
Oxygen source (100 % oxygen, 15 L/minute)
Suctioning apparatus to clear the pharynx as needed
Pulse oximeter, capnometer (end-tidal carbon dioxide monitor), and appropriate sensors
Equipment for alternate methods of airway control should insertion fail (eg, laryngeal mask airway, bag-valve-mask ventilation, endotracheal intubation, cricothyrotomy)
Additional Considerations for Esophageal-Tracheal Double Lumen Tube or Laryngeal Tube Insertion
The balloon cuffs of the esophageal-tracheal double lumen tubes are inflated individually. The balloon cuffs of the laryngeal tubes share a single pilot tube and inflate simultaneously.
In one study, as many as 16% of esophageal-tracheal double lumen tube insertions enter the trachea (1); in these cases, if this placement is recognized, the cuffed distal lumen can be used to function as an endotracheal tube.
The ventilating lumen of the laryngeal tube is suitable for stylet insertion to facilitate conversion of the laryngeal tube to an endotracheal tube. However, visualization of the glottis through this lumen is often impossible.
Relevant Anatomy for Esophageal-Tracheal Double Lumen Tube or Laryngeal Tube Insertion
Aligning the ear with the sternal notch may help open the upper airway and establishes the best position to view the airway if endotracheal intubation becomes necessary.
The degree of head elevation that best aligns the ear and sternal notch varies depending on the patient's age and body habitus.
Positioning for Esophageal-Tracheal Double Lumen Tube or Laryngeal Tube Insertion
Optimal position for tube insertion is the sniffing position.
The operator stands at the head of the stretcher.
An assistant may stand at the side.
The sniffing position is used only in the absence of cervical spine injury:
Position the patient supine on the stretcher.
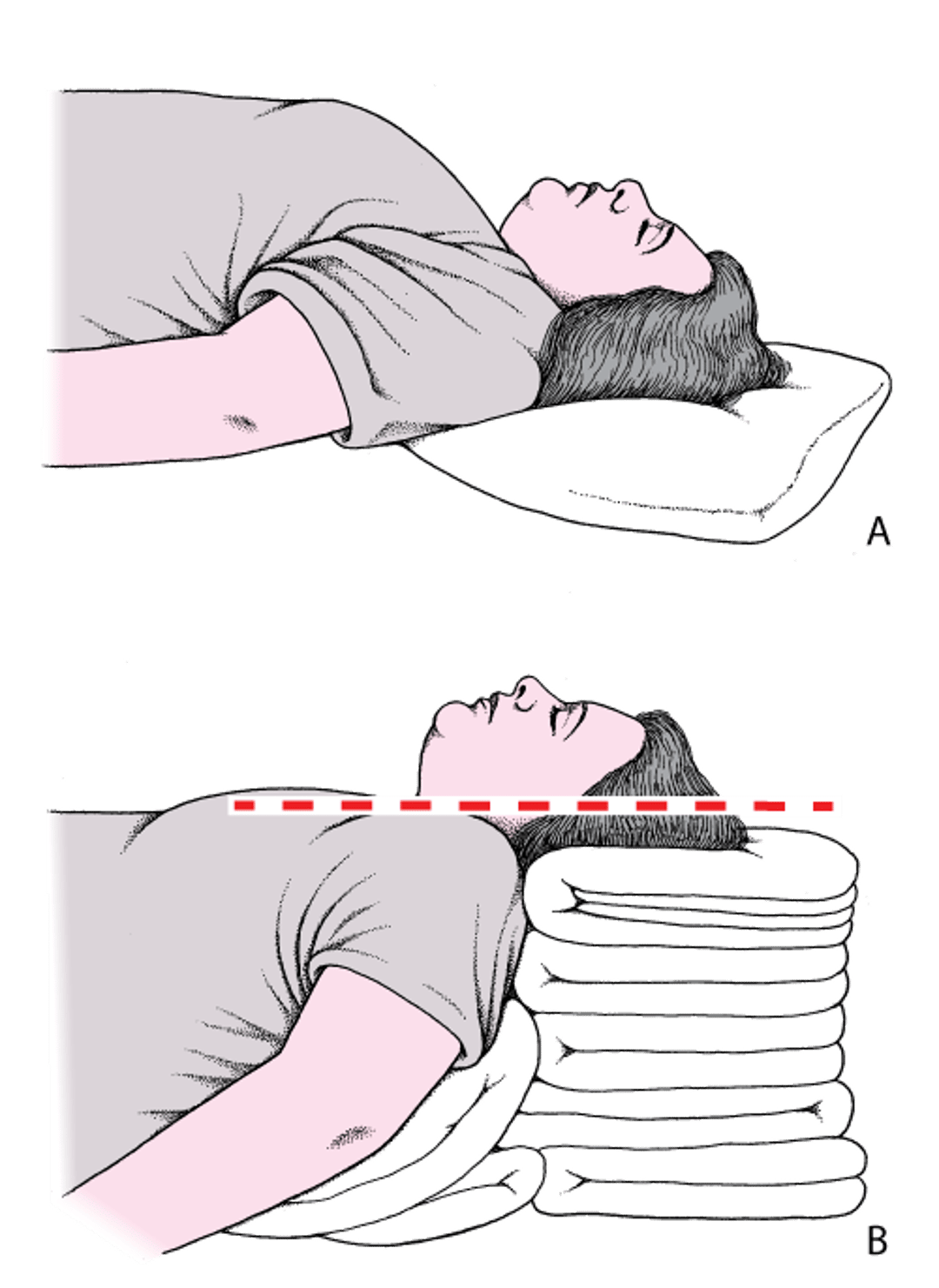
Place folded towels or other materials under the head, neck, and shoulders, flexing the neck so as to elevate the head until the external auditory meatus lies in the same horizontal plane as the sternal notch. Then, tilt the head so that the face aligns on a parallel horizontal plane; this second plane will be above the first. In patients with obesity, many folded towels or a commercial ramp device may be needed to sufficiently elevate the shoulders and neck (see figure ).
Head and Neck Positioning to Open the Airway
A: The head is flat on the stretcher; the airway is constricted. B: Establishing the sniffing position, the ear and sternal notch are aligned, with the face parallel to the ceiling, opening the airway. Adapted from Levitan RM, Kinkle WC: The Airway Cam Pocket Guide to Intubation, ed. 2. Wayne (PA), Airway Cam Technologies, 2007. |

If there is a potential cervical spine injury:
Position the patient supine or at a slight incline on the stretcher. Avoid moving the neck and use only the jaw thrust maneuver or chin lift without head tilt to manually facilitate opening of the upper airway.
Step-by-Step Description of Esophageal-Tracheal Double Lumen Tube or Laryngeal Tube Insertion

Clear the oropharynx, as necessary, of obstructing secretions, vomitus, or foreign material.
Pre-oxygenate the patient with bag-valve-mask ventilation, if possible.
Select the appropriately sized esophageal-tracheal double lumen tube or laryngeal tube based on manufacturer's guidelines and note the appropriate cuff inflation volume for laryngeal tubes. This information is on the tube packaging and the cuff of the tube itself.
Inflate and deflate the cuffs to check that there are no leaks.
Apply a small amount of sterile, water-soluble lubricant to the deflated cuffs.
Lift the chin and tongue with your non-dominant hand. Grasp the tongue and chin between your thumb inside the mouth and your fingers on the underside of the chin, and lift up.
Insert the esophageal-tracheal double lumen tube or laryngeal tube into the mouth. Insert the esophageal-tracheal double lumen tube with a midline orientation. Insert the laryngeal tube initially at the corner of the mouth 45 to 90 degrees of rotation off-center, and then rotate it to midline position when the tip of the tube is past the tongue. Do not force either tube; you may cause soft tissue damage. If resistance is encountered, pull back and re-advance the tube, trying to follow the posterior pharyngeal wall. You may need to remove the tube, alter its curvature, and then reinsert it. At the proper distance of insertion (as confirmed by markings on the tube), the proximal (ventilating) lumen will open over the laryngeal opening, and the distal lumen will have entered the esophagus (in most cases).
Release your hand from the tube before inflating the cuffs.
Inflate the cuffs to the manufacturer’s recommended volume.
Connect a bag-valve apparatus to the ventilating lumen (typically on the esophageal-tracheal double lumen tube, the blue [pharyngeal] lumen).
Begin ventilation (8 to 10 breaths/minute, each about 500 mL and lasting about 1 second).
Assess lung ventilation by auscultation and chest rise. Check end-tidal carbon dioxide to confirm tube placement. Auscultation for esophageal-tracheal double lumen tube placement is often difficult and unreliable, so rely more on capnometry. However, during cardiac arrest, capnometry may not reliably indicate proper tube placement.
With an esophageal-tracheal double lumen tube, if assessment suggests inadvertent tracheal placement (eg, gastric distention or lack of end tidal carbon dioxide), try ventilating through the distal cuff. If the patient does not appear to be getting adequate ventilation through either port, the device should be removed and the patient ventilated using bag-valve-mask ventilation.
With a laryngeal tube, if assessment suggests inadvertent tracheal placement (eg, gastric distention or lack of end tidal carbon dioxide), withdraw the tube a few centimeters to allow the distal portion of the tube to be removed from the trachea and then advanced into the esophagus.
Aftercare for Esophageal-Tracheal Double Lumen Tube or Laryngeal Tube Insertion
Fix the tube in place with tape or ties, as appropriate.
The esophageal-tracheal double lumen tube or laryngeal tube, after several hours at most, must be removed or be replaced by a definitive airway, such as an endotracheal tube or surgical airway (cricothyrotomy or tracheostomy).
Warnings and Common Errors for Esophageal-Tracheal Double Lumen Tube or Laryngeal Tube Insertion
A subset of esophageal-tracheal double lumen tube insertions will result in the distal tube entering the trachea; in this case, ventilation can be done through the distal tube.
Generally, supraglottic airways should be inserted only in patients who are unresponsive; otherwise, aspiration is a risk. Do not allow a patient to awaken during insertion or ventilation with a supraglottic airway. If necessary, prevent the patient from waking up or gagging (using adequate analgesia/sedation and paralytics), or remove the airway as clinically indicated.
Placing the dual lumen tubes too deeply may cause the balloon to obstruct the tracheal opening and inhibit ventilation. Obstruction can be remedied by pulling the airway back a few centimeters.
Reference
1. Calkins TR, Miller K, Langdorf MI. Success and complication rates with prehospital placement of an esophageal-tracheal combitube as a rescue airway. Prehosp Disaster Med. 2006;21(2):97-100. doi:10.1017/s1049023x00003423





