Airway management consists of:
Clearing the upper airway
Maintaining an open air passage with a mechanical device
Sometimes assisting with respirations
There are many indications for airway control (see table ). (See also Overview of Respiratory Arrest.)
Methods of establishing an airway include:
Basic techniques such as head and neck positioning, abdominal thrusts, and back blows (see also How to Do Abdominal Thrusts and Back Blows in the Conscious Adult or Child Who Is Choking and How to Treat the Choking Conscious Infant)
Supraglottic methods such as bag-valve-mask ventilation and laryngeal mask airways
Infraglottic techniques (tracheal intubation)
Surgical airways (eg, scalpel cricothyroidotomy)
Situations Requiring Airway Control
Classification | Examples |
|---|---|
Emergencies | Acute laryngeal edema Deep coma, when the tongue relaxes to occlude the glottis Foreign body at the larynx (eg, “cafe coronary”) Head or high spinal cord injuries Laryngospasm Respiratory arrest or apnea (eg, due to central nervous system disease, medication or illicit drugs, hypoxia) Status epilepticus Upper airway trauma |
Urgencies | Pre-procedure in patients with respiratory or neurologic compromise or other conditions, such as
To reduce the work of breathing in patients experiencing shock, reduced cardiac output, or myocardial stress Need for ventilatory support (eg, in acute respiratory distress syndrome, smoke or toxic inhalation, respiratory burns, gastric aspiration, exacerbations of chronic obstructive pulmonary disease or asthma, diffuse infectious or other parenchymal lung problems, neuromuscular diseases, respiratory center depression, or extreme respiratory muscle fatigue) Respiratory failure with contraindications to or failure of noninvasive ventilation |
Elective | During induction of anesthesia or deep sedation |
Clearing and Opening the Upper Airway
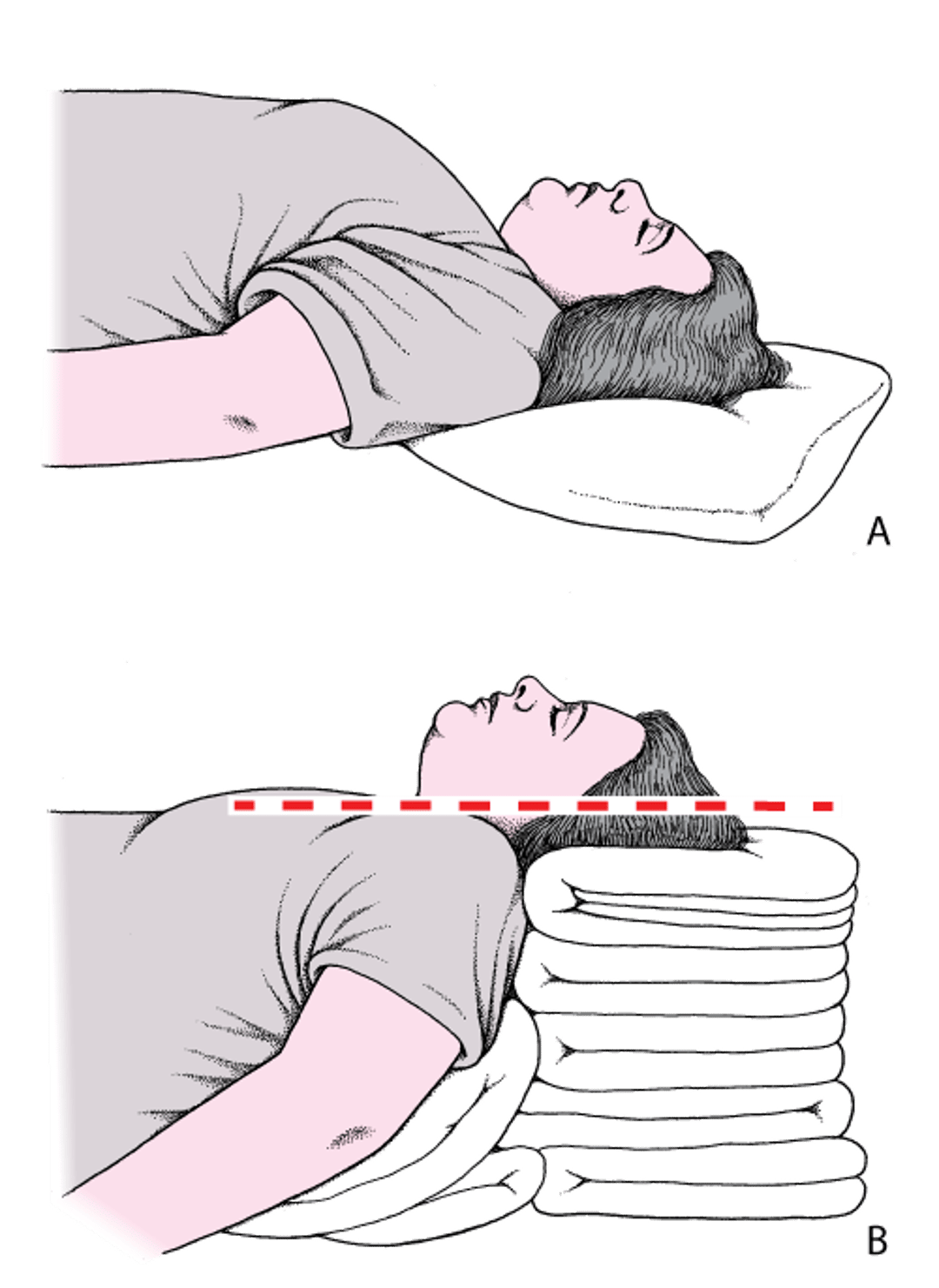
To relieve airway obstruction caused by soft tissues of the upper airway and position optimally for bag-valve-mask ventilation and laryngoscopy, the operator flexes the patient’s neck to elevate the head until the external auditory meatus is in the same plane as the sternum and positions the face roughly parallel to the ceiling (see figure ); this position is slightly different from the commonly taught head-tilt position. The mandible should be displaced upward by lifting the lower jaw and submandibular soft tissue or by pushing the rami of the mandible upward (see figure ).
Note that in infants and young children (under about 2 years old), the relative size of the occiput requires elevation of the shoulders, rather than the head, to maintain a neutral, open airway position.

Head and Neck Positioning to Open the Airway
A: The head is flat on the stretcher; the airway is constricted. B: The ear and sternal notch are aligned, with the face parallel to the ceiling, opening the airway. Adapted from Levitan RM, Kinkle WC: The Airway Cam Pocket Guide to Intubation, ed. 2. Wayne (PA), Airway Cam Technologies, 2007. |

Jaw Thrust

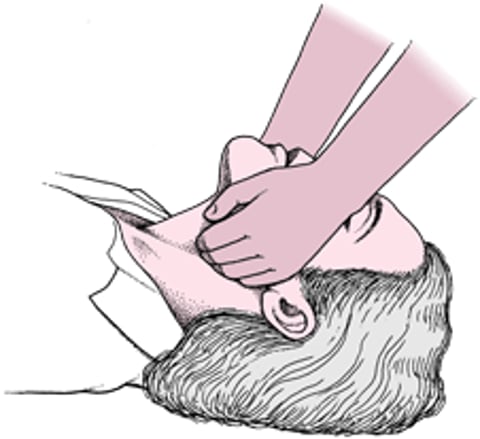
Anatomic restriction, various abnormalities, or considerations caused by trauma (eg, potential cervical spine injury) may be a contraindicaiton to moving the neck; in such cases a jaw thrust is the preferred maneuver to open the airway.
Careful attention to optimal positioning when possible can maximize airway patency and improve bag-valve-mask ventilation and laryngoscopy.
Obstruction by dentures or oropharyngeal foreign material (eg, blood, secretions) may be removed by finger sweep of the oropharynx and/or suction, taking care not to push the material deeper (more likely in infants and young children, in whom a blind finger sweep is contraindicated). Deeper material can be removed with Magill forceps or by suction.
Treating the conscious, choking patient
People who are choking are initially conscious but unable to make audible noise. They may point to their throat or place their hands to their throat. A rescuer asks "are you choking?" and, upon receiving an affirmative answer, proceeds immediately with rescue maneuvers.
Subdiaphragmatic abdominal thrusts (Heimlich maneuver )
Subdiaphragmatic abdominal thrusts (for more detailed instructions, see How To Do Abdominal Thrusts and Back Blows in the Conscious Adult or Child Who Is Choking) are manual thrusts to the upper abdomen or, in the case of patients who are pregnant or have extreme obesity, chest thrusts until the airway is clear or the patient becomes unconscious; it is the preferred initial method in a patient who is awake and choking.
In conscious adults, the rescuer stands behind the patient with arms encircling the patient’s midsection. One fist is clenched and placed midway between the umbilicus and xiphoid. The other hand grabs the fist, and a firm inward and upward thrust is delivered by pulling with both arms (see figure ).
An unconscious adult with an upper airway obstruction is initially managed with CPR (cardiopulmonary resuscitation). In such patients, chest compressions increase intrathoracic pressure in the same manner that abdominal thrusts do in conscious patients. Rescuers should provide cycles of 30 chest compressions at a rate of 100 to 120 compressions/minute followed with 2 rescue breaths. Rescuers should examine the oropharynx before each set of breaths and use their fingers to remove any visible objects. Direct laryngoscopy with suction or Magill forceps can also be used to remove a foreign body in the proximal airway, but once an object has passed through the vocal folds positive pressure from below the obstruction is more likely to be successful. Lay rescuers who do not know how or are unwilling to give rescue breaths should perform compressions-only CPR.
Procedures for choking in infants and small children
Abdominal Thrusts With Victim Standing or Sitting (Conscious)

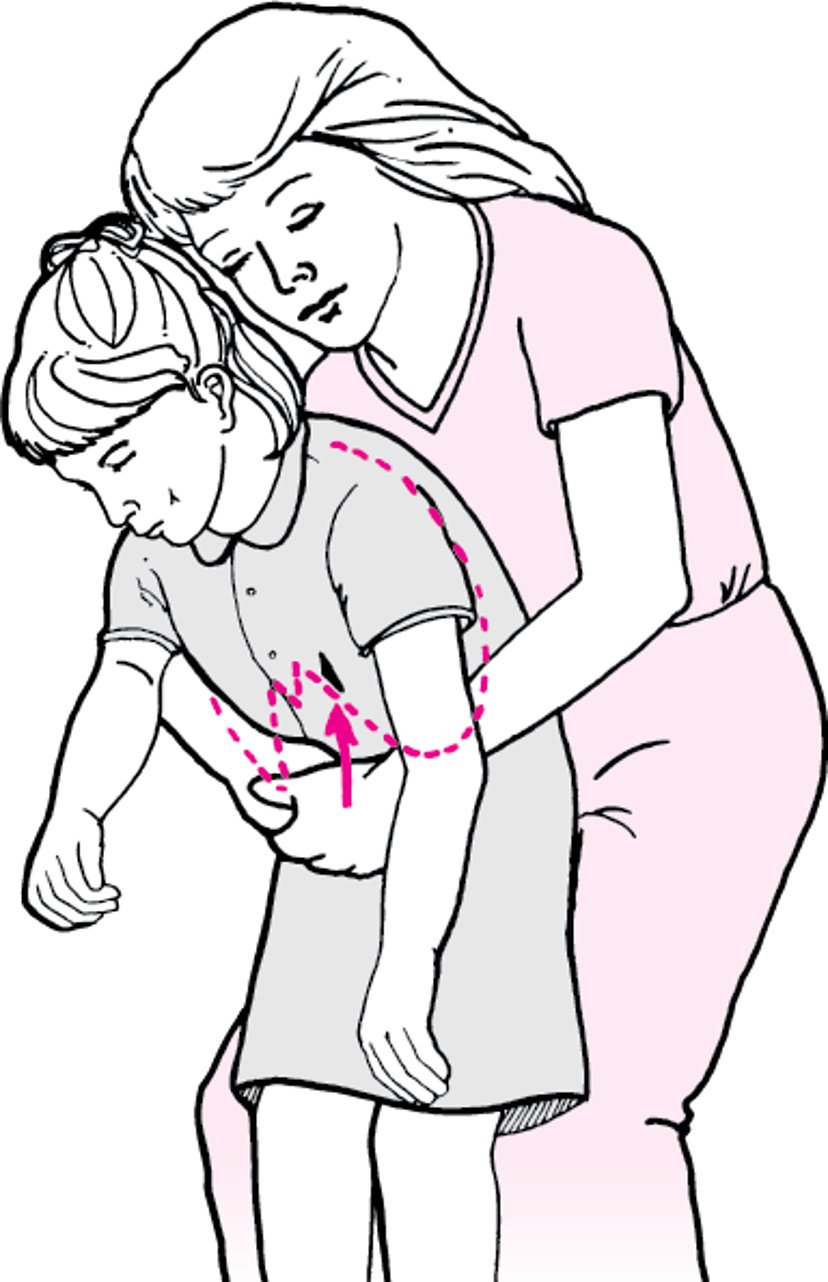
In older children, the abdominal thrusts may be used. However, in children < 20 kg (typically < 5 years), moderate pressure should be applied, and the rescuer should kneel at the child’s feet rather than astride.
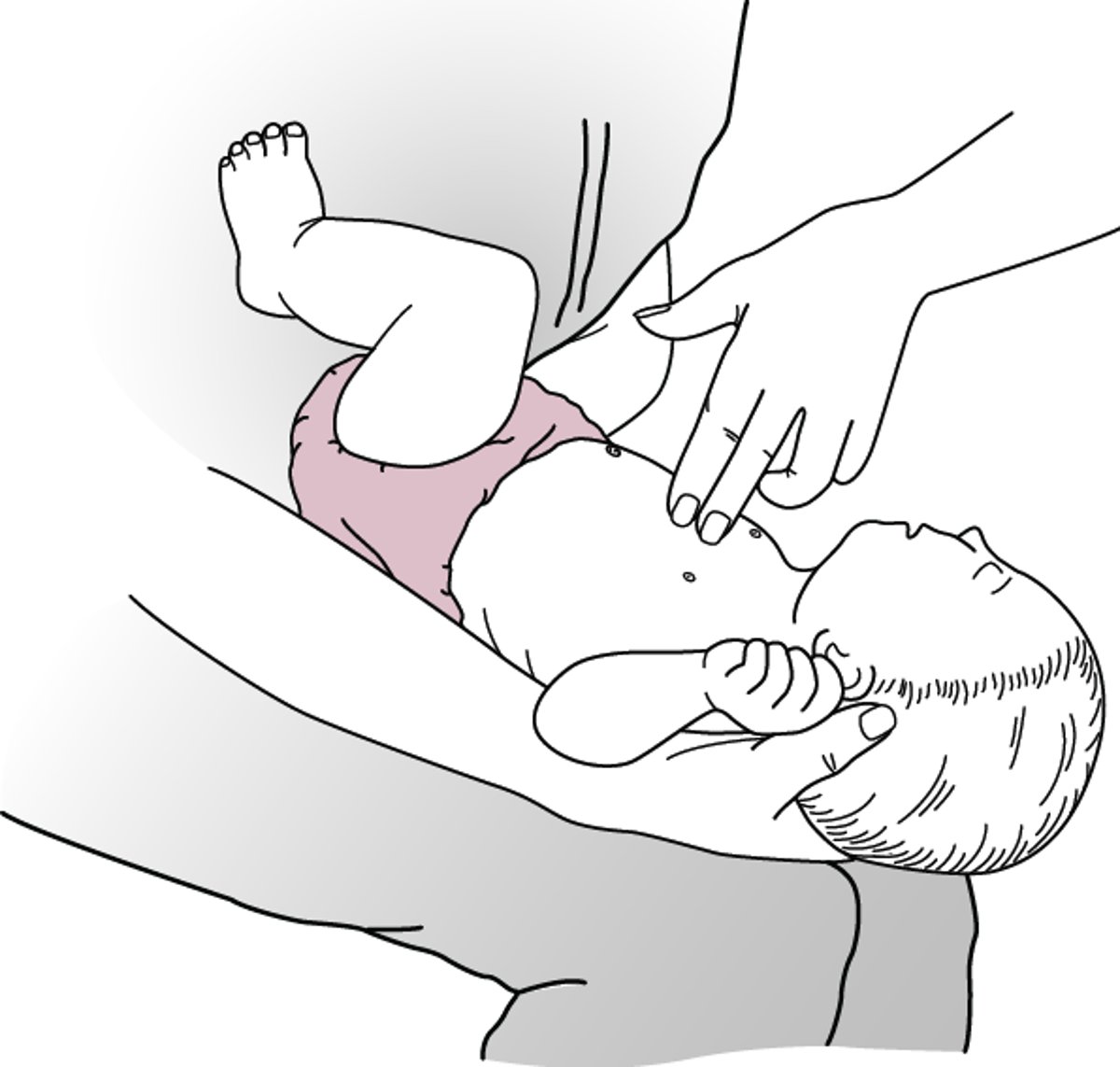
In infants < 1 year, the abdominal thrusts should not be performed. Infants should be held in a prone, head-down position. The rescuer should support the head with the fingers of one hand while delivering 5 back blows (see figure ). Five chest thrusts should then be delivered with the infant in a head-down position with the infant’s back on the rescuer’s thigh (supine—see figure ). This sequence of back blows and chest thrusts is repeated until the airway is cleared, or the infant becomes unresponsive and CPR is started. For more detailed instructions, see How To Treat the Choking Conscious Infant.
Back Blows—Infant

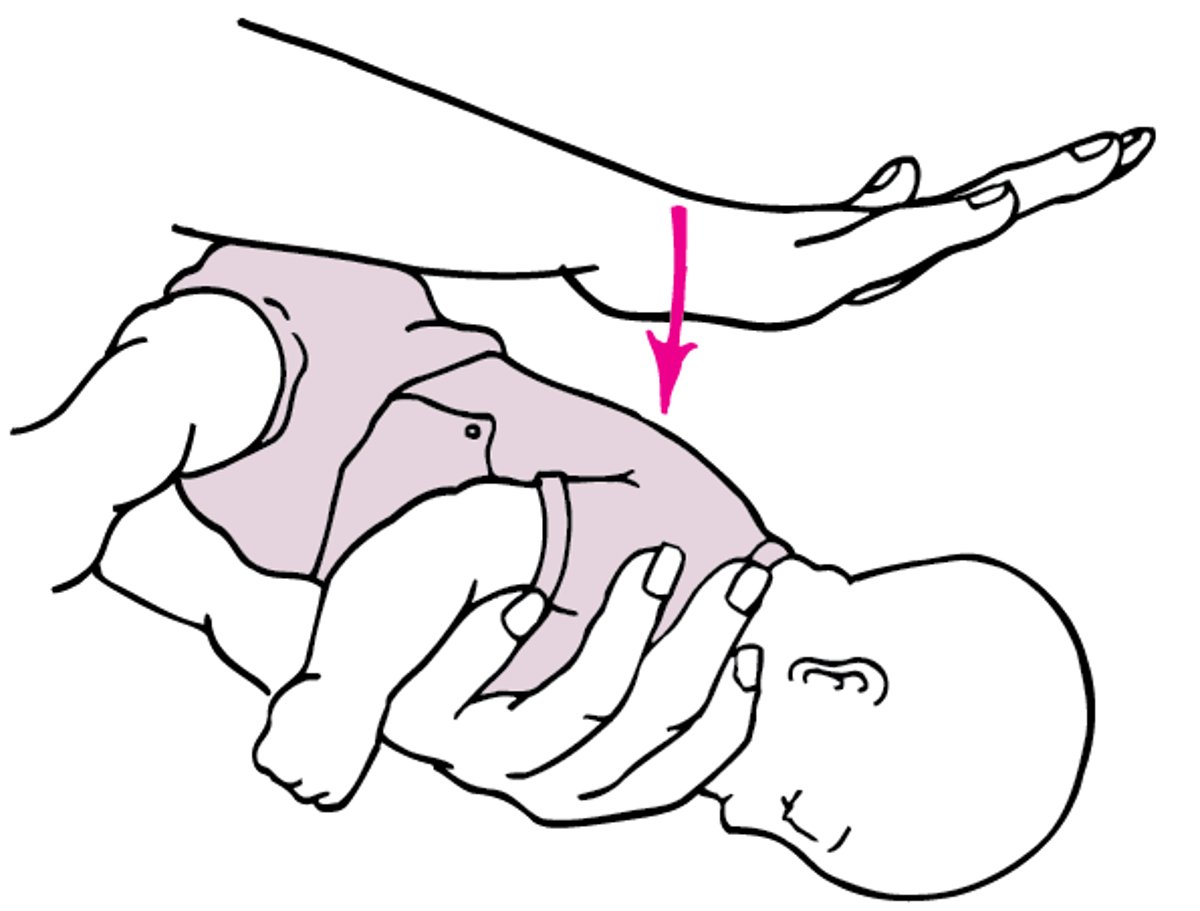
Chest Thrusts—Infant
Chest thrusts are delivered on the lower half of the sternum, just below the nipple level. |