



Caries is tooth decay, commonly called cavities. The symptoms—tender, painful teeth—appear late. Diagnosis is based on inspection, probing of the enamel surface with a fine metal instrument, and dental radiographs. Treatment involves removing affected tooth structure and restoring it with various materials. Fluoride, diligent dental hygiene, sealants, and proper diet can prevent virtually all caries.
Etiology of Caries
The etiology of caries is best described as multifactorial and dynamic. Many caries result from buildup of plaque, or dental biofilm, that accumulates in the mouth each day (1). Certain bacteria in dental plaque are able to ferment carbohydrates, producing acids that can result in demineralization of hard tooth structure. Plaque is, at first, a soft, thin film of bacteria, mucin, dead epithelial cells, and food debris that develops on the tooth surface within about 24 hours after the tooth is cleaned. Streptococcus mutans species, a group of related bacteria, grow in plaque and can cause caries. Some strains are more cariogenic than others. Eventually (commonly, after 72 hours), soft plaque mineralizes, mainly with calcium and phosphate, becoming calculus (hard plaque or tartar), which cannot easily be removed with a toothbrush.
Risk factors
There are several risk factors for caries:
Inadequate control of plaque and tartar
Dental defects
Diet, particularly frequent consumption of carbohydrates (including sugars) and highly acidic foods and liquids
Low intake of oral fluoride
Characteristics of saliva, including reduced salivary flow (eg, due to medications, radiation therapy, systemic disorders that cause salivary gland dysfunction), buffering capacity, and pH
Genetic factors
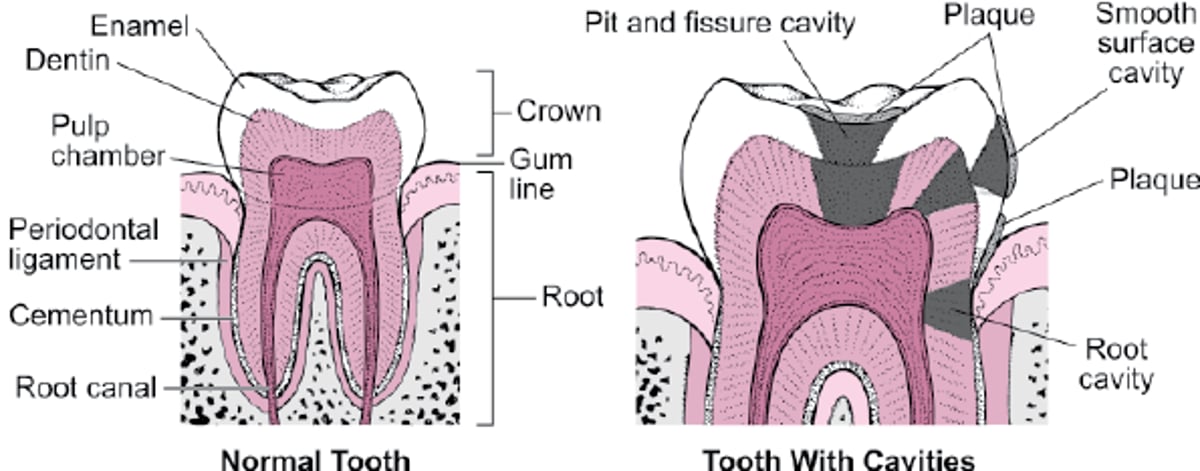
Many teeth have open enamel pits, fissures, and grooves, which may extend from the surface to the dentin (see figure ). These defects may be wide enough to harbor bacteria but too narrow to clean effectively. They predispose teeth to caries.
Frequent dietary exposure to carbohydrates and sugars promotes the growth of plaque-forming bacteria. Development of severe early childhood caries (rampant caries) in deciduous teeth suggests prolonged contact with infant formula, milk, or juice, typically when an infant goes to bed with a bottle (baby or nursing bottle caries). Thus, bedtime bottles should contain only water.
A tooth surface is more susceptible to caries when it is poorly calcified, has low fluoride exposure, and/or is in an acidic environment. Typically, decalcification begins when the pH at the tooth falls below 5.5. This occurs when lactic acid–producing bacteria colonize the area or when people drink soft drinks, sports drinks, or energy drinks, all of which commonly have pH values below 5.5.


New and recurrent dental caries in a patient with dry mouth.
Image provided by Jonathan A. Ship, DMD.
Older patients often take medications that reduce salivary flow, predisposing to caries. They also have a higher incidence of root caries because of gingival recession, exposure of root surfaces, and declining manual dexterity (causing ineffective oral hygiene).
Types of Cavities

Complications
Untreated caries leads to tooth destruction, infections, and the need for extractions and replacement prostheses. Caries in children can lead to premature loss of deciduous teeth with shift of adjacent teeth, hindering eruption of their permanent successors.
Reference
1. Wong A, Subar PE, Young DA. Dental caries: An update on dental trends and therapy. Adv Pediatr 64(1):307-330, 2017. doi: 10.1016/j.yapd.2017.03.011
Symptoms and Signs of Caries
Caries initially involves only the enamel and causes no symptoms. Caries that invades the dentin causes pain, first when hot, cold, or sweet foods or beverages contact the involved tooth, and later with chewing or percussion. Pain can be intense and persistent when the pulp is severely involved (pulpitis).
Diagnosis of Caries
Direct visual inspection and careful use of dental explorer
Periodic dental radiographs
Sometimes special adjunctive tests


Image provided by James Ubertalli, DMD.
Routine, frequent clinical evaluation (every 3 to 12 months depending on a patient's caries risk as assessed by a dentist) identifies early caries at a time when minimal intervention prevents progression. A thin probe, sometimes special dyes, and transillumination by fiberoptic lights are used, although infrequently these are supplemented by new devices that detect caries by changes in electrical conductivity, laser reflectivity, or transillumination (including use of near-infrared light devices). However, radiographs are still most important for detecting caries, determining the depth of involvement, and identifying caries under existing restorations.
Treatment of Caries
Restorative therapy
Sometimes a root canal and crown
Remineralization of teeth
For teeth with incipient caries (affected area confined to the enamel), remineralization is usually attempted by improved home care (brushing and flossing), more frequent cleanings, prescriptions for high-fluoride toothpastes, and multiple fluoride applications at the dental office (1). Incipient carious lesions confined to enamel may also be treated with resin infiltration (2).
Other topical products for remineralization that contain only calcium and phosphates are less effective than fluoride. Silver diamine fluoride (SDF) can arrest and remineralize carious lesions (3). However, because most SDF permanently stains caries black, it is generally reserved for use on deciduous teeth.
Restoration of teeth
The primary treatment of caries that has entered dentin is mechanical removal by drilling, followed by filling the resultant defect.
Restorative materials for treating caries vary depending on the location and size of the carious lesion. Fillings for occlusal surfaces of posterior teeth, which bear the brunt of mastication, must be composed of strong materials, including
Silver amalgam
Composite resins
Reinforced glass ionomers
Silver amalgam combines silver, mercury, copper, tin, and occasionally zinc, palladium, or indium. Amalgam is inexpensive and lasts an average of 14 years. However, if oral hygiene is good and if amalgam was placed using a rubber dam for isolation from saliva, many amalgam fillings last > 40 years. In general, amalgam restorations last longer and are more resistant to secondary caries than composite restorations (4).
There is a trend toward using dental materials other than amalgam (5). Amalgam use is decreasing for several reasons:
Cosmetic results are not as aesthetically pleasing as those achieved with either composites or glass ionomers.
The durability of composite resins has improved.
Updated dental school curricula now commonly include use of restorative materials other than amalgam.
Environmental concerns about the removal and disposal of the mercury content of amalgam are more commonly taken into consideration.
Although concern has been raised about "mercury poisoning," blood mercury levels do not correlate with the number of amalgam fillings a person has. Replacing amalgam is not recommended because it is expensive, damages tooth structure, actually increases patient exposure to mercury, and requires the use of amalgam separators to prevent dispersal of its mercury content into the environment.
Composite resins, which have a more acceptable appearance, have long been used in anterior teeth where aesthetic concerns are primary and the forces of chewing are minimal. Many patients request them in posterior teeth as well, and they are now commonly used there. Early-generation composite resins under high occlusal stress lasted less than half as long as amalgam and could lead to recurrent decay because the composite resin shrinks when it hardens and expands and contracts with heat and cold more than the tooth or other filling materials. The current generation of composites more closely simulates enamel hardness, does not appear to have the same incidence of recurrent caries as earlier materials, and may also last longer. Use of bonded composite resin restorations allows for more conservation of tooth structure compared to amalgam preparations.
Glass ionomer, a tooth-colored filling, releases fluoride when in place, a benefit for patients especially prone to tooth decay. It is also used to restore areas damaged by overzealous brushing. Glass ionomer is not as aesthetic as composite and should not be used on chewing surfaces because it has a high wear rate. Resin-modified glass ionomer materials are also available and provide some improved aesthetics compared to conventional glass ionomers.
If decay leaves too little dentin to retain a full or partial coverage restoration, the missing dentin is replaced with cement, amalgam, composite, or other materials. Sometimes a post must be inserted into 1 or more roots to support a gold, silver, or composite core, which replaces the coronal dentin. This procedure necessitates a root canal filling, in which an opening is made in the tooth and the pulp is removed. The root canal system is thoroughly debrided, shaped, and then filled with gutta percha. The outer tooth surfaces (what would have been the enamel) are then reduced so that an artificial crown—usually made of metal, porcelain, or ceramic—can be placed. Crowns for anterior teeth are made of, or covered with, porcelain or ceramic.
Treatment references
1. Wong A, Subar PE, Young DA. Dental caries: An update on dental trends and therapy. Adv Pediatr 64(1):307-330, 2017. doi: 10.1016/j.yapd.2017.03.011
2. Bourouni S, Dritsas K, Kloukos D, Wierichs RJ. Efficacy of resin infiltration to mask post-orthodontic or non-post-orthodontic white spot lesions or fluorosis - a systematic review and meta-analysis. Clin Oral Investig 2021;25(8):4711-4719. doi:10.1007/s00784-021-03931-7
3. Fontana M, Gonzalez-Cabezas C. Evidence-Based Dentistry Caries Risk Assessment and Disease Management. Dent Clin North Am 2019;63(1):119-128. doi:10.1016/j.cden.2018.08.007
4. Moraschini V, Fai CK, Alto RM, et al. Amalgam and resin composite longevity of posterior restorations: A systematic review and meta-analysis. J Dent 43(9):1043-1050, 2015. doi: 10.1016/j.jdent.2015.06.005
5. Lamsal R, Estrich CG, Sandmann D, Bartelt K, Lipman RD. Declining US dental amalgam restorations in US Food and Drug Administration-identified populations: 2017-2023. J Am Dent Assoc 2024;155(10):816-824. doi:10.1016/j.adaj.2024.07.015
Prevention of Caries
Regular brushing and flossing
Fluoride in water, toothpaste, or both
Regular professional cleanings
Rarely chlorhexidine rinses and topical fluoride applications
For most people, caries are preventable. Cavities first form on permanent teeth in the early teens to late 20s. Caries-prone people typically have low exposure to fluoride and a relatively cariogenic microflora acquired from their mothers or through social contact.


Maintaining good oral hygiene is especially important, as are dietary factors, particularly minimizing intake of sugar and acidic drinks and eating a diet rich in sources of calcium.
Removal of plaque at least every 24 hours, usually by brushing and flossing, helps prevent dental caries. The gingival third of the tooth is the most important area to clean but is the area most often neglected. Brushing with an electric toothbrush for 2 minutes is excellent; brushing with a manual soft toothbrush for 3 to 4 minutes suffices. Using excess toothpaste, particularly an abrasive type, may erode the teeth. Dental floss is placed between each of the teeth, curved against the side of each tooth, and moved up and down 3 times, going just beneath the gingival margin. Flosses that are very thin or coated with wax or polytetraethylene can be used for exceptionally tight contacts between teeth or rough filling margins. Water flossers can be considered for patients with dexterity problems or patients undergoing orthodontic therapy.
When fluoride is incorporated into teeth, the enamel is more resistant to acidic decalcification and recalcifies more readily when pH increases. Fluoridated toothpaste should be used by people of all ages.
If drinking water is not adequately fluoridated, oral fluoride supplements are recommended for children from 6 months through 16 years. Fluoride supplements in pregnant women have not been shown to prevent caries in offspring and thus are no longer recommended (1).
Oral fluoride supplements for children are available in toothpastes, liquids (for use in a dropper for infants), gels, and tablets. Tablets should be swished in the mouth to enhance topical fluoride absorption before swallowing. The dose must be selected according to the amount of fluoride present in the drinking water and diet, the age of the child, and whether topical fluoride is being used in toothpaste and/or applied during dental care. Excessive fluoride exposure may cause dental fluorosis , causing mild to severe discoloration of teeth. Because young children may swallow toothpaste when brushing, which can lead to fluorosis, they should use children's toothpastes, which contain lower amounts of fluoride.
Fluoridation offers less protection against caries in pits and fissures than against those on smooth surfaces. Deep, narrow pits and fissures require use of sealants (resin materials that adhere tightly to the surface of the enamel) to prevent nutrients from reaching bacteria, thereby reducing bacterial growth and acid production.
If these measures do not decrease cavity formation, more intensive therapy is aimed at changing the flora. Following treatment of cavities and sealing of pits and fissures, use of a 0.12% chlorhexidine mouth rinse (60 seconds twice a day for 2 weeks) is recommended to reduce the cariogenic bacteria in plaque and allow repopulation with less cariogenic strains of S. mutans. However, the effectiveness of chlorhexidine in reducing dental caries is uncertain (2). To encourage repopulation of mouth flora with less cariogenic bacterial strains, xylitol in the form of hard candy or chewing gum (for 5 minutes) is used 3 times a day. Additionally, a 5000 ppm high-fluoride toothpaste regimen may be prescribed, or topical fluoride may be applied by a dentist or used at night in a custom-made fluoride carrier.
For pregnant women with a history of severe caries, prenatal interventions may reduce transfer of cariogenic bacteria from mother to child and delay caries formation in the child. Preventive measures in pregnancy focus on improved maternal oral health and include limiting sugary food and drinks, brushing twice daily with toothpaste containing fluoride, and daily flossing. If this is not feasible, the mother can use xylitol from the time of the child’s birth to the age at which the mother no longer samples the child’s food (a hypothesized mode of transfer).
For prevention of caries in deciduous teeth (once they have erupted) in infants, bedtime bottles should contain only water.
Prevention references
1. Richards D. No evidence that fluoride supplements taken during pregnancy prevent caries. Evid Based Dent 19(3):73, 2018. doi: 10.1038/sj.ebd.6401320
2. Walsh T, Oliveira-Neto JM, Moore D. Chlorhexidine treatment for the prevention of dental caries in children and adolescents. Cochrane Database Syst Rev 2015;2015(4):CD008457. Published 2015 Apr 13. doi:10.1002/14651858.CD008457.pub2
Key Points
Caries is caused by acids produced by bacteria in dental plaque.
Risk factors include preexisting tooth defects, low saliva flow, an acidic oral environment, frequent exposure to carbohydrates and sugar in the diet, and inadequate exposure to fluoride.
Treatment of incipient caries confined to the enamel may be attempted with remineralization through improved home care (brushing and flossing), cleanings, prescriptions for high-fluoride toothpastes, and multiple fluoride applications at the dental office.
Treatments of caries that have entered the dentin involve drilling out the decayed area and restoring the defect with amalgam, composite resin, or glass ionomer.
Prevention involves meticulous regular brushing, flossing, and professional cleaning; adequate fluoride must be available in toothpaste and, when not present in drinking water, provided as oral supplements for children.
Drug Information for the Topic





