



Tinea versicolor refers to a skin infection with Malassezia furfur that manifests as multiple asymptomatic scaly patches varying in color from white to tan to brown to pink. Diagnosis is based on clinical appearance and potassium hydroxide (KOH) wet mount of skin scrapings. Treatment is with topical or sometimes oral antifungals. Recurrence is common.
Malassezia furfur is a fungus that can exist as both a yeast and as a mold (a dimorphic fungus). It is normally a commensal organism on normal skin but in some people causes tinea versicolor. Most affected people are healthy. Tinea versicolor is benign and is not considered contagious.
Factors that may predispose to tinea versicolor include heat and humidity and immunosuppression due to glucocorticoids, pregnancy, undernutrition, diabetes, or other disorders such as advanced HIV.
Hypopigmentation in tinea versicolor is due to the inhibition of tyrosinase caused by M. furfur production of azelaic acid.
Symptoms and Signs of Tinea Versicolor
Tinea versicolor is usually asymptomatic. Classically, it causes the appearance of multiple tan, brown, salmon, pink, or white scaling patches on the trunk, neck, abdomen, and occasionally face. The lesions may coalesce. In light-skinned patients, the condition is often diagnosed in the summer months because the lesions, which do not tan, become more conspicuous against tanned skin.


In this photo, tinea versicolor manifests as multiple hypopigmented scaly patches on the trunk.
In this photo, tinea versicolor manifests as multiple hypopigmented scaly patches on the trunk.
Image provided by Thomas Habif, MD.


A well-demarcated brown patch is visible, along with two incidental hemangiomas.
A well-demarcated brown patch is visible, along with two incidental hemangiomas.
© Springer Science+Business Media


© Springer Science+Business Media


Image courtesy of Karen McKoy, MD.

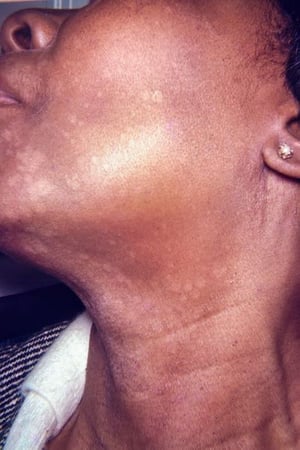
Image courtesy of Karen McKoy, MD.
In this photo, tinea versicolor manifests as multiple hypopigmented scaly patches on the trunk.
In this photo, tinea versicolor manifests as multiple hypopigmented scaly patches on the trunk.
Image provided by Thomas Habif, MD.
A well-demarcated brown patch is visible, along with two incidental hemangiomas.
A well-demarcated brown patch is visible, along with two incidental hemangiomas.
© Springer Science+Business Media
© Springer Science+Business Media
Image courtesy of Karen McKoy, MD.
Image courtesy of Karen McKoy, MD.
Diagnosis of Tinea Versicolor
Primarily physical examination
Potassium hydroxide (KOH) wet mount
The diagnosis of tinea versicolor is based on clinical appearance and by identification of hyphae and budding cells (“spaghetti and meatballs” appearance) on potassium hydroxide wet mount of fine scale scrapings. Vitiligo with depigmented macules should also be considered as a differential diagnosis.
Treatment of Tinea Versicolor
Topical antifungals
Sometimes oral antifungals
Treatment of tinea versicolor is any topical antifungal (1). (See table .) Examples include:
Selenium sulfide shampoo 2.5% applied to the skin (in 10-minute applications daily for 1 week or 24-hour applications once a week for 1 month)
Topical azoles (eg, ketoconazole 2% daily for 2 weeks)
Daily bathing with pyrithione zinc soap 2% or sodium thiosulfate/salicylic acid shampoo 2% applied to the skin for 1 to 2 weeks
Fluconazole orally for 2 to 4 weeks is indicated for patients with extensive disease and those with frequent recurrences.
Hypopigmentation resulting from tinea versicolor is reversible in months to years after the yeast has cleared.
Recurrence is frequent after treatment because the causative organism is a normal skin commensal organism. Fastidious hygiene, regular use of pyrithione zinc soap, or once-monthly use of topical antifungal therapy lowers the likelihood of recurrence.
Treatment reference
1. Hu SW, Bigby M. Pityriasis versicolor: a systematic review of interventions. Arch Dermatol. 2010;146(10):1132-1140. doi:10.1001/archdermatol.2010.259
Key Points
Although tinea versicolor can occur in patients who are immunosuppressed, most affected patients are healthy.
The disorder is frequently diagnosed in the summer because hypopigmented lesions become more conspicuous against tanned skin.
The diagnosis is confirmed by finding hyphae and budding cells ("spaghetti and meatballs" appearance) on potassium hydroxide wet mount of fine scale scrapings.
Treatment is with topical or oral antifungals.
Drug Information for the Topic





