



Serous otitis media is an effusion in the middle ear resulting from incomplete resolution of acute otitis media or obstruction of the eustachian tube without infection. Symptoms include hearing loss and a sense of fullness or pressure in the ear. Diagnosis is based on the appearance of the tympanic membrane and sometimes on tympanometry. Most cases resolve in 2 to 3 weeks. If there is no improvement in 1 to 3 months, some form of myringotomy is indicated, usually with insertion of a tympanostomy tube. Antibiotics and decongestants are not effective.
Serous otitis media (also called otitis media with effusion) is an effusion of the middle ear secondary to inflammation.
Normally, the middle ear is ventilated 3 to 4 times a minute as the eustachian tube opens during swallowing, and oxygen is absorbed by blood in the vessels of the middle ear mucous membrane. If patency of the eustachian tube is impaired, a relative negative pressure develops within the middle ear, sometimes leading to fluid accumulation. This fluid may cause conductive hearing loss.
Serous otitis media is a common sequela to acute otitis media or upper respiratory infection in children (often identified during a routine ear recheck) where the acute infection has resolved, but the effusion may persist for weeks to months (1). Eustachian tube obstruction may also be secondary to the following:
Inflammatory processes in the nasopharynx
Allergic rhinitis
Hypertrophic adenoids
Other obstructive lymphoid aggregations on the torus of the eustachian tube and in the Rosenmüller fossa
Benign or malignant tumors of the nasopharynx or infratemporal fossa
History of head and neck radiation
The effusion is most commonly due to inflammation, and is sterile. In some children, pathogenic bacteria may be detected in middle ear washes; however, the clinical significance of this finding is unclear (2). Rarely, a spontaneous cerebrospinal fluid (CSF) leak due to erosion through the lateral skull base may manifest as serous otitis media.
General references
1. Rosenfeld RM, Shin JJ, Schwartz SR, et al. Clinical Practice Guideline: Otitis Media with Effusion (Update). Otolaryngol Head Neck Surg. 2016;154(1 Suppl):S1-S41. doi:10.1177/0194599815623467
2. Buzatto GP, Tamashiro E, Proenca-Modena JL, et al. The pathogens profile in children with otitis media with effusion and adenoid hypertrophy. PLoS One. 2017;12(2):e0171049. Published 2017 Feb 23. doi:10.1371/journal.pone.0171049
Symptoms and Signs of Serous Otitis Media
Patients may report no symptoms, but some (or their family members) note hearing loss. Patients may experience a feeling of fullness, pressure, or popping in the ear during swallowing. Otalgia is rare.
Various possible changes to the tympanic membrane include an amber or gray color, displacement of the light reflex, mild to severe retraction, and accentuated landmarks. During air insufflation, the tympanic membrane may be immobile. An air-fluid level or bubbles of air may be visible through the tympanic membrane.

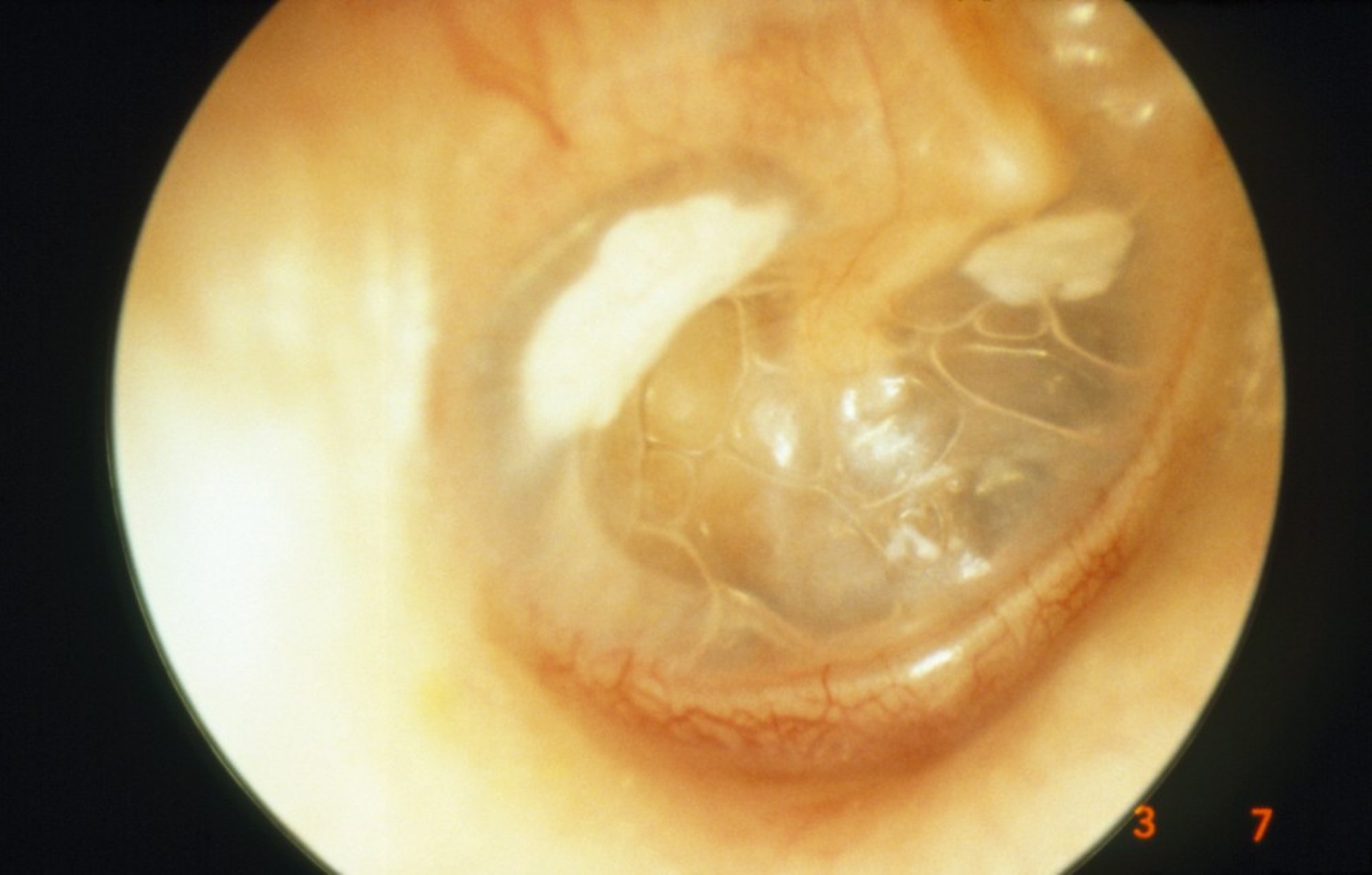
In some patients with acute serous otitis media, blebs and tympanosclerosis (white, chalky plaques on the tympanic membrane) can be seen.
TONY WRIGHT, INSTITUTE OF LARYNGOLOGY AND OTOLOGY/SCIENCE PHOTO LIBRARY
Diagnosis of Serous Otitis Media
History and physical examination
Pneumatic otoscopy and/or tympanometry
Nasopharyngeal examination
The diagnosis of serous otitis media is clinical plus pneumatic otoscopy (1). For pneumatic otoscopy, an insufflator attached to the otoscope head is used to move the tympanic membrane; fluid in the middle ear, a perforation, or tympanosclerosis inhibits this movement. Tympanometry may be performed to confirm middle ear effusion (by showing reduced mobility of the tympanic membrane). Both acute otitis media and serous otitis media are characterized by fluid in the middle ear. The key difference between acute otitis media and serous otitis media is that a bulging tympanic membrane is present in acute otitis media, but not in serous otitis media.
If an effusion persists for> 8 weeks, adults and adolescents must undergo nasopharyngeal examination to exclude malignant or benign tumors. Nasopharyngeal malignancy should be suspected, particularly in patients with unilateral serous otitis media or in patients with risk factors such as smoking. If malignancy is suspected, imaging studies should be performed.
Diagnosis reference
1. Arnold MJ. Otitis Media With Effusion in Children: Guidelines From NICE. Am Fam Physician. 2024;110(3):318-319.
Treatment of Serous Otitis Media
Observation
If unresolved, myringotomy with tympanostomy tube insertion
If recurrent in childhood, sometimes adenoidectomy
For most patients, watchful waiting is all that is required. Most cases of serous otitis media resolve spontaneously within 3 months, and surveillance at 3- to 6-month intervals is generally appropriate for children without hearing difficulties or other concerning symptoms (1). Antihistamines, and decongestants are not recommended (2). If allergic rhinitis is suspected, antihistamines and nasal glucocorticoids may be helpful. Antibiotics are not routinely recommended; however, antibiotics may be of limited benefit for short-term resolution of serous otitis media in children (3).
If serous otitis media persists for > 3 months, myringotomy may be performed (for aspiration of fluid) and a tympanostomy tube inserted, (for ventilation of the middle ear and temporary amelioration of eustachian tube obstruction). Tympanostomy tubes may also be inserted for persistent conductive hearing loss secondary to middle ear fluid that does not clear. Tympanostomy tubes can help prevent recurrences of acute otitis media and serous otitis media (4).


Image Copyright © Nucleus Medical Media. All rights reserved.
Occasionally, the middle ear can be temporarily ventilated with the Valsalva maneuver or politzerization. To perform the Valsalva maneuver, patients keep their mouth closed and try to forcibly blow air out through their pinched nostrils (popping the ear). To perform politzerization, the clinician blows air with a special syringe (middle ear inflator) into one of the patient’s nostrils and blocks the other while the patient swallows. This forces the air into the eustachian tube and middle ear. Neither procedure should be performed if the patient has a cold and rhinorrhea. Patients may be instructed to gently pinch their nostrils and swallow (called auto-insufflation). This maneuver can be repeated several times throughout the day to aerate the middle ear.
Persistent or recurrent serous otitis media may require management of underlying nasopharyngeal conditions. In children, particularly adolescent boys, a nasopharyngeal angiofibroma should be ruled out; in adults, nasopharyngeal carcinoma must be ruled out. Children may benefit from adenoidectomy, including the removal of the central adenoid mass as well as lymphoid aggregations on the torus of the eustachian tube and in the Rosenmüller fossa. Antibiotics should be given for bacterial rhinitis, sinusitis, and/or nasopharyngitis. Confirmed allergens should be eliminated from the patient’s environment and allergen immunotherapy should be considered.
Susceptible young children with prolonged hearing loss due to long-standing serous otitis may require appropriate therapy to ensure age-appropriate language development. Balloon dilation of the eustachian tube has been used as an alternative to tympanostomy tube placement (5). While the patient is under general anesthesia, a specialist inserts a balloon into the eustachian tube under endoscopic guidance and briefly dilates the tube before removing the balloon. This procedure is an option for patients with recurrent serous otitis media and those who do not wish to have a tympanostomy tube placed. Caution should be used for some patients with mild eustachian tube dysfunction symptoms (eg, a sense of fullness, pressure, or popping in the ear) because this procedure can cause patulous eustachian tube dysfunction; symptoms include a sense of fullness and autophony (when patients hear their own breathing), which can cause them distress.
Because environmental pressure changes can cause painful barotrauma, scuba diving and air travel should be avoided or delayed when possible. If air travel cannot be avoided, chewing food or drinking (eg, from a bottle) may help young children. A Valsalva maneuver or politzerization (during descent of an airplane, people should pinch their nose shut, hold their mouth closed, and try to blow gently out through their nose; this maneuver forces air through the blocked eustachian tube) may help older children and adults.
For patients with a history of radiation of the head and neck, serous effusions are secondary to eustachian tube dysfunction from the radiotherapy. Caution should be exercised in these patients for myringotomy and pressure equalizing tube placement as this may cause chronic otorrhea. It is advisable to consider monitoring the effusion and have the patient wear a hearing aid if there are no recurrent infections. While some patients benefit from pressure equalizing tubes, there is a higher chance of chronic otorrhea and infections related to the tubes in patients with a history of head and neck radiation.
Treatment references
1. Rosenfeld RM, Shin JJ, Schwartz SR, et al. Clinical Practice Guideline: Otitis Media with Effusion (Update). Otolaryngol Head Neck Surg. 2016;154(1 Suppl):S1-S41. doi:10.1177/0194599815623467
2. Burton MJ, Rosenfeld RM. Extracts from The Cochrane Library: antihistamines and/or decongestants for otitis media with effusion (OME) in children. Otolaryngol Head Neck Surg. 2007;136(1):11-13. doi:10.1016/j.otohns.2006.10.039
3. Mulvaney CA, Galbraith K, Webster KE, et al. Antibiotics for otitis media with effusion (OME) in children. Cochrane Database Syst Rev. 2023;10(10):CD015254. Published 2023 Oct 23. doi:10.1002/14651858.CD015254.pub2
4. Rosenfeld RM, Keppel KL, Vaughan WK, et al. Plain Language Summary: Tympanostomy (Ear) Tubes in Children. Otolaryngol Head Neck Surg. 2022;166(2):207-216. doi:10.1177/01945998211065663
5. Poe D, Anand V, Dean M, et al. Balloon dilation of the eustachian tube for dilatory dysfunction: A randomized controlled trial. Laryngoscope. 2018;128 (5):1200–1206. doi: 10.1002/lary.26827 Epub 2017 Sep 20.
Key Points
Serous otitis media is primarily noninfectious middle ear effusion usually following acute otitis media or an upper respiratory infection.
Diagnosis is clinical; for adults and adolescents, perform a nasopharyngeal examination and sometimes imaging studies to exclude malignant or benign tumors.
Antibiotics, antihistamines, and decongestants are not helpful.
If unresolved in > 3 months, myringotomy with tympanostomy tube insertion and/or direct visualization of the nasopharynx may be needed.
Children with prolonged hearing loss may require appropriate therapy to ensure age-appropriate language development.





