

Acute otitis media is a bacterial or viral infection of the middle ear, usually accompanying an upper respiratory infection. Symptoms include otalgia, often with systemic symptoms (eg, fever, nausea, vomiting, diarrhea), especially in the very young. Diagnosis is based on otoscopy. Treatment is with analgesics and sometimes antibiotics.
Acute otitis media is an infectious inflammation of the middle ear. It is different from otitis media with effusion, also called serous otitis media, which refers to an accumulation of non-infected fluid in the middle ear (ie, in the absence of acute infection).
Risk factors
Certain environmental and host factors can modulate disease risk. For example, the presence of smoking in the household is a significant risk factor for acute otitis media. Other risk factors include having a strong family history of otitis media, living in a low-resource or high air-pollution region, being bottle fed (instead of breastfed), and group attendance at a day care center.
Complications
Complications of acute otitis media are uncommon. In rare cases, bacterial middle ear infection spreads locally, resulting in acute mastoiditis, petrositis, or labyrinthitis. Intracranial spread is extremely rare; it usually causes meningitis. Brain abscess, subdural empyema, epidural abscess, lateral sinus thrombosis, or otitic hydrocephalus may occur. Even with antibiotic treatment, intracranial complications are slow to resolve, especially in immunocompromised patients.
Epidemiology of Acute Otitis Media
Acute otitis media can occur at any age; however, it is most common in very young children. There is a slight male predominance.
In one systematic review of pooled global data, the worldwide incidence of otitis media in 2021 was found to be 4959/100,000 (1). Incidence was highest in children aged < 2 years, and the largest number of episodes was in children aged 2 to 4 years. In the United States, acute otitis media is the most common diagnosis in childhood leading to acute sick visits, and the leading indication for antibiotic prescriptions in children (2). It is estimated that 50 to 85% of children in the United States will have experienced at least 1 episode of acute otitis media by 3 years of age.
The global mortality rate of acute otitis media is very low (< 0.1/100,000) (1).
Epidemiology references
1. GBD 2021 Upper Respiratory Infections Otitis Media Collaborators. Global, regional, and national burden of upper respiratory infections and otitis media, 1990-2021: a systematic analysis from the Global Burden of Disease Study 2021. Lancet Infect Dis. 2025;25(1):36-51. doi:10.1016/S1473-3099(24)00430-4
2. Gaddey HL, Wright MT, Nelson TN. Otitis Media: Rapid Evidence Review. Am Fam Physician. 2019;100(6):350-356.
Etiology of Acute Otitis Media
The primary function of the eustachian tube is as a passage to equalize air pressure and drain fluid from the middle ear into the nasopharynx. In very young children, the eustachian tube is structurally and functionally immature—the angle of the eustachian tube is more horizontal than in adults, and the angle of the tensor veli palatini muscle and the cartilaginous eustachian tube makes the opening mechanism less efficient. These physiologic factors contribute to the higher likelihood of retention of fluid in the middle ear and the subsequent development of acute otitis media in children. In older children or adults, dysfunctions of the eustachian tube can similarly lead to acute otitis media.


This illustration shows a eustachian tube in its normal closed state (main image) and in an open state (arrows; inset, upper right). The eustachian tubes connect the middle ear to the nasopharynx. They are also called the auditory tubes or pharyngotympanic tubes.
CLAUS LUNAU/SCIENCE PHOTO LIBRARY
The etiology of acute otitis media may be viral or bacterial. Viral infections are often complicated by secondary bacterial infection.
In neonates, causes of acute otitis media commonly include:
Gram-negative enteric bacilli (including Escherichia coli)
Chlamydia trachomatis
Group B streptococci
In older infants and children, organisms causing acute otitis media commonly include (1, 2):
Streptococcus pneumoniae
Moraxella catarrhalis
Nontypeable Haemophilus influenzae
Group A beta-hemolytic streptococci (eg, Streptococcus pyogenes), < 5% of cases
Pneumococcal conjugate vaccines and their evolution from 7-valent to higher-valency formulations to combat serotype shifts has led to decreases in the prevalence of Streptococcus pneumoniae-induced otitis media and relative increases in the proportions of other organisms as a cause of acute otitis media (particularly H. influenzae) (1, 3).


Etiology references
1. Shaikh N. Otitis Media in Young Children. N Engl J Med. 2025;392(14):1418-1426. doi:10.1056/NEJMcp2400531
2. Lieberthal AS, Carroll AE, Chonmaitree T, et al. The diagnosis and management of acute otitis media. Pediatrics. 2013;131(3):e964-e999. doi:10.1542/peds.2012-3488
3. Marom T. Burden of upper respiratory infections and otitis media. Lancet Infect Dis. 2025;25(1):3-5. doi:10.1016/S1473-3099(24)00532-2
Symptoms and Signs of Acute Otitis Media
The usual initial symptom is otalgia (earache), often with hearing loss. Infants may simply be cranky or have difficulty feeding or sleeping. Fever, nausea, vomiting, and diarrhea often occur in young children. Otoscopic examination can show a bulging, erythematous tympanic membrane with indistinct landmarks and displacement of the light reflex. Air insufflation (pneumatic otoscopy) shows reduced mobility of the tympanic membrane. Spontaneous perforation of the tympanic membrane causes serosanguineous or purulent otorrhea, typically rapidly relieving the pain.

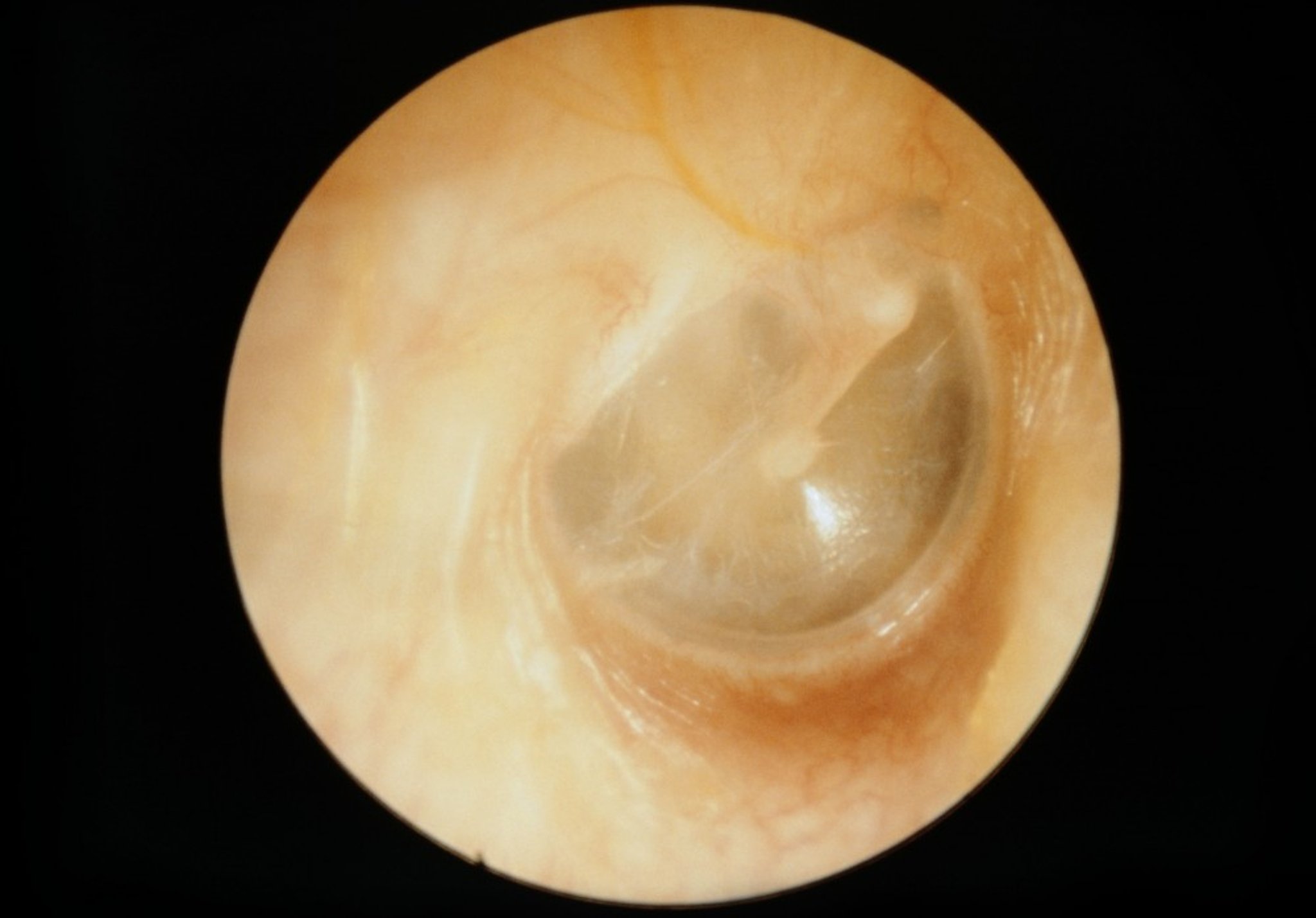
The normal right tympanic membrane is pearly in color and has visible, distinct landmarks.
CLINICA CLAROS/SCIENCE PHOTO LIBRARY

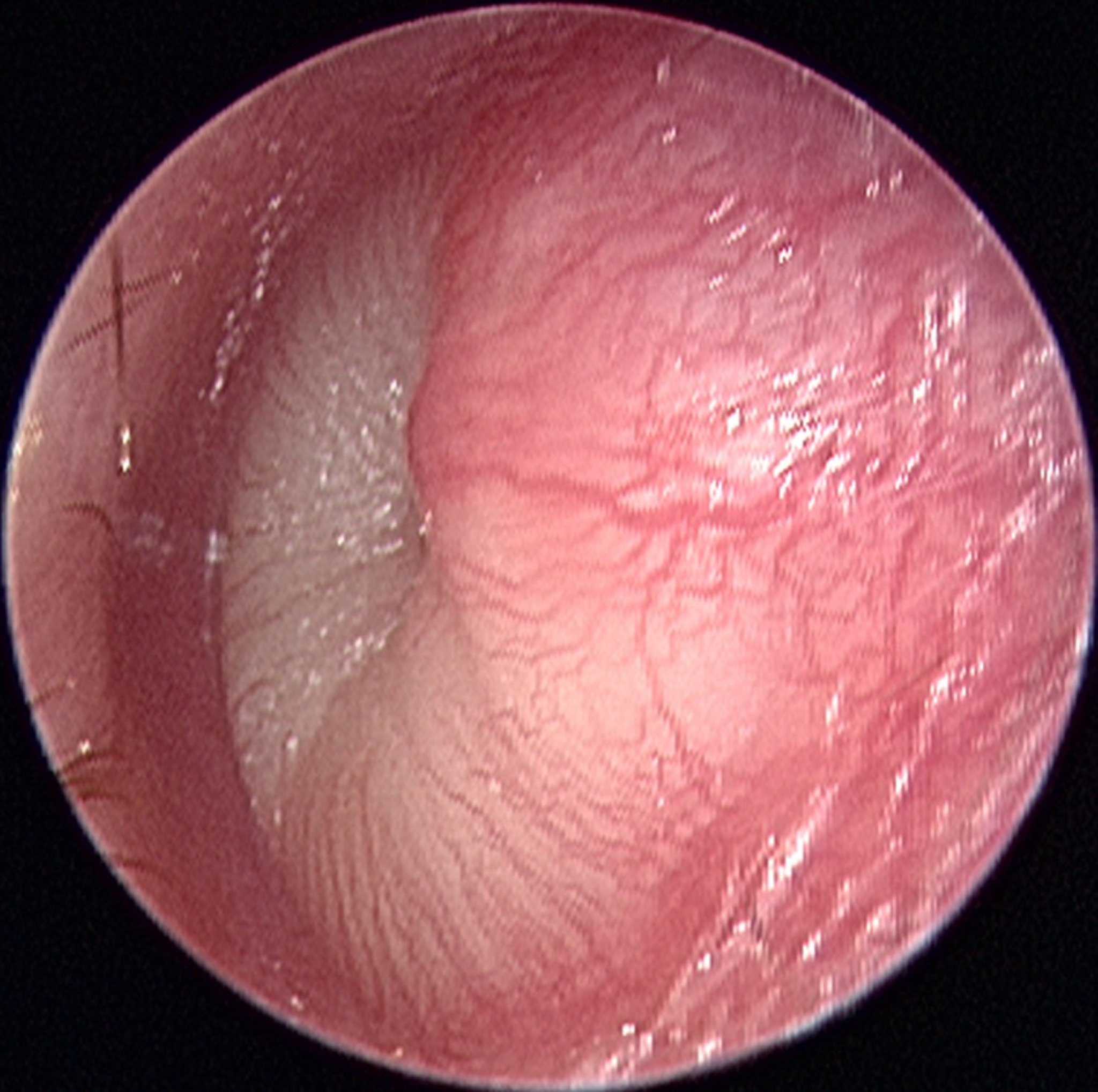
The left tympanic membrane in acute otitis media (bottom) is bulging and erythematous and has indistinct landmarks, obscured because of the bulging tympanic membrane.
© Springer Science+Business Media


DR P. MARAZZI/SCIENCE PHOTO LIBRARY
Severe headache, confusion, or focal neurologic signs may occur with intracranial spread of infection. Facial paralysis or vertigo suggests local extension to the fallopian canal or labyrinth.
Diagnosis of Acute Otitis Media
History and physical examination alone
The diagnosis of acute otitis media usually is clinical, based on the presence of acute (within 48 hours) onset of pain, bulging of the tympanic membrane and, particularly in children, signs of middle ear effusion detected by pneumatic otoscopy (1).
Unless fluid is obtained during tympanocentesis, myringotomy, or spontaneous tympanic membrane perforation, cultures are usually not performed.
Diagnosis reference
1. Lieberthal AS, Carroll AE, Chonmaitree T, et al. The diagnosis and management of acute otitis media. Pediatrics. 2013;131(3):e964-e999. doi:10.1542/peds.2012-3488
Treatment of Acute Otitis Media
Analgesics
Sometimes antibiotics
Rarely myringotomy
The treatment of acute otitis media primarily involves the administration of adequate analgesia. The decision to treat with antibiotics is largely based on the severity of infection, age of the child, and laterality of the condition. Rarely surgical procedures may be required to decompress the middle ear.
Analgesia should be provided to all children diagnosed with acute otitis media (1). Oral analgesics, such as acetaminophen or ibuprofen, may be used; weight-based doses are used for children (). Oral analgesics, such as acetaminophen or ibuprofen, may be used; weight-based doses are used for children (2).
Initial observation is an option for children aged 6 to 23 months with nonsevere unilateral acute otitis media or children ≥ 24 months with nonsevere unilateral or bilateral acute otitis media (1). Observation as initial management for acute otitis media in properly selected children does not increase suppurative complications. Some cases can resolve spontaneously; higher remittance rates are seen in resource-rich settings (1, 3).
Pediatric organizations have recommended initial antibiotics for certain children, such as the following (see table ) (1):
Those who are younger or more severely ill
Those with recurrent acute otitis media (eg, ≥ 4 episodes in 6 months)
Those with bilateral disease
High-dose amoxicillin is generally the preferred antibiotic (see table High-dose amoxicillin is generally the preferred antibiotic (see table). The duration of treatment is typically 10 days for children < 2 years and 7 days for older children (1). Cases of otitis media are considered resistant when patients have not improved after 48 to 72 hours of treatment, have had a previous resistant infection, have used amoxicillin in the previous 30 days, or have concurrent purulent conjunctivitis. Antibiotics may provide modest symptom relief a few days after administration and appear to reduce abnormal tympanometry findings at 2 to 4 weeks (). Cases of otitis media are considered resistant when patients have not improved after 48 to 72 hours of treatment, have had a previous resistant infection, have used amoxicillin in the previous 30 days, or have concurrent purulent conjunctivitis. Antibiotics may provide modest symptom relief a few days after administration and appear to reduce abnormal tympanometry findings at 2 to 4 weeks (3). Other children, provided there is good follow-up, can safely be observed for 48 to 72 hours and given antibiotics only if no improvement is seen; if follow-up by phone is planned, a prescription can be given at the initial visit to save time and expense. The decision to observe should be discussed with the caregiver and be made on a case-by-case basis.
Antibiotics for Otitis Media
Antibiotic | Comments |
|---|---|
Initial treatment | |
AmoxicillinAmoxicillin | Given orally Preferred unless the child has one of the following:
High-dose regimen for possible resistant organisms |
Penicillin-allergic* | |
CefdinirCefdinir | Given orally |
CefuroximeCefuroxime | Usually given orally, IV may be considered for severe cases |
CefpodoximeCefpodoxime | — |
CeftriaxoneCeftriaxone | Given IV or IM Considered particularly for children who have severe vomiting or will not swallow antibiotic liquids |
Resistant cases† | |
Amoxicillin/clavulanateAmoxicillin/clavulanate | Given orally Preferred; dose based on amoxicillin component (usually high-dose regimens)Preferred; dose based on amoxicillin component (usually high-dose regimens) Caution required to make sure not to exceed the maximum daily dose of clavulanate |
CeftriaxoneCeftriaxone | Given IV or IM Can use even if oral cephalosporin is ineffective Considered if adherence is likely to be poor |
ClindamycinClindamycin | 2nd-line alternative, consider using with a cephalosporin |
Treatment duration is typically 10 days for children < 2 years and 7 days for older children unless otherwise specified. Antibiotics are given orally unless otherwise specified. | |
* Cross reactivity of 2nd- and 3rd-generation cephalosporins with penicillin is very low. | |
† Cases are treated as resistant when patients have not improved after 48 to 72 hours of treatment, have had a previous resistant infection, have used amoxicillin in the previous 30 days, or have concurrent purulent conjunctivitis.† Cases are treated as resistant when patients have not improved after 48 to 72 hours of treatment, have had a previous resistant infection, have used amoxicillin in the previous 30 days, or have concurrent purulent conjunctivitis. | |
Data from Lieberthal AS, Carroll AE, Chonmaitree T, et al. The diagnosis and management of acute otitis media. Pediatrics. 2013;e964–99. | |
Guidelines for Using Antibiotics in Children With Acute Otitis Media*
Age | Otorrhea | Severe symptoms† (unilateral or bilateral) | Bilateral disease | Unilateral disease, no severe symptoms |
|---|---|---|---|---|
< 6 months‡ | Antibiotics | Antibiotics | Antibiotics | Antibiotics |
6 months to 2 years | Antibiotics | Antibiotics | Antibiotics | Antibiotics or observe 48 to 72 hours§ |
≥ 2 years | Antibiotics | Antibiotics | Antibiotics or observe 48 to 72 hours§ | Antibiotics or observe 48 to 72 hours§ |
* These guidelines apply only to children who meet the diagnostic criteria for acute otitis media (eg, acute [within 48 hours] onset of pain, bulging of the tympanic membrane, and signs of middle ear effusion detected by pneumatic otoscopy). | ||||
† Symptoms include temperature ≥ 39° C rectally any time within previous 24 hours, moderate to severe otalgia for > 48 hours, or clinician’s judgment that child is seriously ill. | ||||
‡ The guidelines in the Pediatrics article from which this table was derived do not include this age group, in which observation has not been thoroughly studied. Thus, it is reasonable to continue to treat with antibiotics. | ||||
§ Decision making should be shared with parents. Observation is appropriate only if phone or office follow-up can be assured within 48 to 72 hours; antibiotics are started if no improvement. | ||||
Modified from Lieberthal AS, Carroll AE, Chonmaitree T, et al. The diagnosis and management of acute otitis media. Pediatrics. 2013;e964–99. | ||||
In adults, topical intranasal vasoconstrictors, such as phenylephrine or oxymetazoline, may improve eustachian tube function and drainage of middle ear fluid, although the efficacy of these preparations has not been clearly shown. To avoid rebound congestion, these preparations should not be used In adults, topical intranasal vasoconstrictors, such as phenylephrine or oxymetazoline, may improve eustachian tube function and drainage of middle ear fluid, although the efficacy of these preparations has not been clearly shown. To avoid rebound congestion, these preparations should not be used> 3 days.
In children, neither vasoconstrictors nor antihistamines are not routinely used. One large meta-analysis concluded that the evidence was very uncertain regarding the benefits or harms of decongestants or antihistamines (4).


Image Copyright © Nucleus Medical Media. All rights reserved.
Surgical procedures to decompress the ear may be required in selected cases. For example, myringotomy may be performed by a specialist for a bulging tympanic membrane, particularly if severe or persistent pain, fever, vomiting, or diarrhea is present. Tympanometry is used to monitor tympanic membrane movement; the patient's hearing and tympanic membrane appearance and movement are monitored until normal. If facial nerve palsy or weakness occurs in patients with acute otitis media, patients must be urgently referred to a specialist for possible myringotomy and placement of a tympanostomy tube as well as intravenous antibiotics.
Treatment references
1. Lieberthal AS, Carroll AE, Chonmaitree T, et al. The diagnosis and management of acute otitis media. Pediatrics. 2013;131(3):e964-e999. doi:10.1542/peds.2012-3488
2. de Sévaux JLH, Damoiseaux RA, van de Pol AC, et al. Paracetamol (acetaminophen) or non-steroidal anti-inflammatory drugs, alone or combined, for pain relief in acute otitis media in children. . Paracetamol (acetaminophen) or non-steroidal anti-inflammatory drugs, alone or combined, for pain relief in acute otitis media in children.Cochrane Database Syst Rev. 2023;8(8):CD011534. Published 2023 Aug 18. doi:10.1002/14651858.CD011534.pub3
3. Venekamp RP, Sanders SL, Glasziou PP, et al. Antibiotics for acute otitis media in children. Cochrane Database Syst Rev. 2023;11(11):CD000219. Published 2023 Nov 15. doi:10.1002/14651858.CD000219.pub5
4. Darlison P, Moresco L, Nussbaumer-Streit B, et al; supported by Cochrane Sweden and Cochrane Austria. Decongestants and antihistamines for acute otitis media in children. Cochrane Database Syst Rev. 2025;11(11):CD015839. Published 2025 Nov 27. doi:10.1002/14651858.CD015839.pub2
Prevention of Acute Otitis Media
Routine childhood vaccination against pneumococci (with pneumococcal conjugate vaccine), H. influenzae type B, and influenza decreases the incidence of acute otitis media (1, 2, 3).
Infants should not sleep with a bottle, and elimination of household smoking may decrease incidence. Prophylactic antibiotics are not recommended for children who have recurrent episodes of acute otitis media.
Recurrent acute otitis media and recurrent serous otitis media may be prevented by the insertion of tympanostomy tubes.
Prevention references
1. Fortanier AC, Venekamp RP, Hoes AW, et al. Does pneumococcal conjugate vaccination affect onset and risk of first acute otitis media and recurrences? A primary care-based cohort study. Vaccine. 2019;37(11):1528-1532. doi:10.1016/j.vaccine.2019.01.064
2. Norhayati MN, Ho JJ, Azman MY. Influenza vaccines for preventing acute otitis media in infants and children. Cochrane Database Syst Rev. 2017;10(10):CD010089. Published 2017 Oct 17. doi:10.1002/14651858.CD010089.pub3
3. Sigurdsson S, Eythorsson E, Hrafnkelsson B, et al. Reduction in All-Cause Acute Otitis Media in Children <3 Years of Age in Primary Care Following Vaccination With 10-Valent Pneumococcal Haemophilus influenzae Protein-D Conjugate Vaccine: A Whole-Population Study. Clin Infect Dis. 2018;67(8):1213-1219. doi:10.1093/cid/ciy233
Key Points
Analgesics should be given to all patients.
Antibiotics should be used in selected patients, based on patient age, severity of illness, and availability of follow-up.
Antihistamines and decongestants are not recommended for children.
Nasal decongestants and antihistamines may help adults; antihistamines may benefit those with an allergic etiology.
Drug Information for the Topic





