



Addison disease is an insidious, usually progressive hypofunctioning of the adrenal cortex. It causes various symptoms, including hypotension and hyperpigmentation, and can lead to adrenal crisis with cardiovascular collapse. Diagnosis is clinical and is based on elevated plasma adrenocorticotropic hormone (ACTH) with low plasma cortisol. Treatment depends on the cause but generally includes glucocorticoids (eg, hydrocortisone) and mineralocorticoids (eg, fludrocortisone).
(See also Overview of Adrenal Function.)
Addison disease is a primary adrenal disorder. The prevalence of Addison disease appears to be highest in European countries (10 to 22 per 100,000 people) and lower in Asia (0 to 4 per 100,000 in South Korea) (1). It occurs in all age groups, about equally in each sex, and tends to become clinically apparent during metabolic stress, infection, or trauma.
General reference
1. Husebye ES, Pearce SH, Krone NP, Kämpe O. Adrenal insufficiency. Lancet. 2021;397(10274):613-629. doi:10.1016/S0140-6736(21)00136-7Adr
Etiology of Primary Adrenal Insufficiency
Approximately 90% of cases of primary adrenal insufficiency in the United States and Europe are due to autoimmune disease (1). The remainder result from destruction of the adrenal gland by granuloma (eg, tuberculosis, histoplasmosis), tumor, amyloidosis, hemorrhage, or inflammatory necrosis. Hypoadrenocorticism can also result from administration of medications that block glucocorticoid synthesis (eg, ketoconazole, etomidate).
Addison disease may coexist with diabetes mellitus or hypothyroidism in polyglandular deficiency syndrome. In children, the most common cause of primary adrenal insufficiency is congenital adrenal hyperplasia. A rarer genetic cause is adrenoleukodystrophy.
Adrenal crisis (onset of severe symptoms) may be precipitated by acute infection. Infection is a common cause, especially when there is septicemia. Other causes include trauma, surgery, and sodium loss due to excessive sweating. Even with treatment, Addison disease may cause a slight increase in mortality. It is not clear whether this increase is due to mistreated adrenal crises or long-term complications of inadvertent over-replacement.
Etiology reference
1. Bornstein SR, Allolio B, Arlt W, et al. Diagnosis and Treatment of Primary Adrenal Insufficiency: An Endocrine Society Clinical Practice Guideline. J Clin Endocrinol Metab. 2016;101(2):364-389. doi:10.1210/jc.2015-1710
Pathophysiology of Primary Adrenal Insufficiency
In adrenal insufficiency, both mineralocorticoids and glucocorticoids are deficient.
Mineralocorticoid deficiency
Because mineralocorticoids stimulate sodium reabsorption and potassium excretion, deficiency results in increased excretion of sodium and decreased excretion of potassium, chiefly in urine but also in sweat, saliva, and the gastrointestinal tract. A low serum concentration of sodium (hyponatremia) and a high concentration of potassium (hyperkalemia) result.
Urinary salt and water loss cause severe dehydration, plasma hypertonicity, acidosis, decreased circulatory volume, hypotension, and, eventually, circulatory collapse. However, when adrenal insufficiency is caused by inadequate adrenocorticotropic hormone (ACTH) production (secondary adrenal insufficiency), electrolyte levels are often normal or only mildly deranged, and the circulatory problems are less severe.
Glucocorticoid deficiency
Glucocorticoid deficiency contributes to hypotension and causes severe insulin sensitivity and disturbances in carbohydrate, fat, and protein metabolism. In the absence of cortisol, insufficient carbohydrate is formed from protein; hypoglycemia and decreased liver glycogen result. Weakness follows, due in part to deficient neuromuscular function. Resistance to infection, trauma, and other stress is decreased. Myocardial weakness and dehydration reduce cardiac output, and circulatory failure can occur.
A decreased blood cortisol level results in increased pituitary ACTH production and increased blood beta-lipotropin level. Beta-lipotropin has melanocyte-stimulating activity and, together with ACTH, causes the hyperpigmentation of skin and mucous membranes characteristic of Addison disease. Thus, adrenal insufficiency secondary to pituitary failure does not cause hyperpigmentation.
Symptoms and Signs of Primary Adrenal Insufficiency
Weakness, fatigue, and orthostatic hypotension are early symptoms and signs of Addison disease.
Skin hyperpigmentation is characterized by diffuse darkening of exposed and, to a lesser extent, unexposed portions of the body, especially on pressure points (bony prominences), skin folds, scars, and extensor surfaces. Black freckles are common on the forehead, face, neck, and shoulders. Bluish black discolorations of the areolae and mucous membranes of the lips, mouth, rectum, and vagina occur.

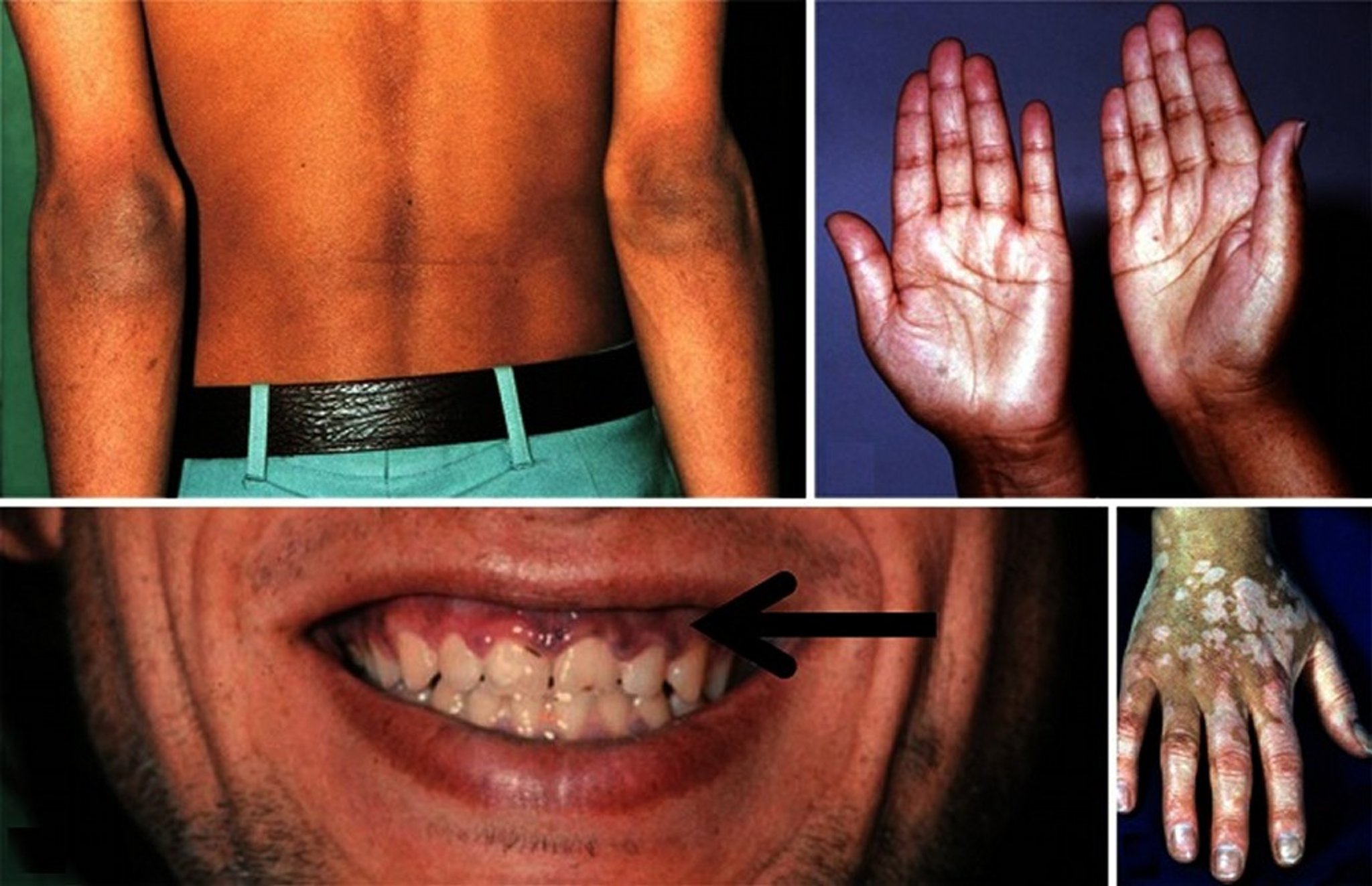
Patients with Addison disease have diffuse hyperpigmentation as well as hyperpigmentation on extensor surfaces (here the elbows) as in the top left panel. In the top right panel, hyperpigmentation of the palmar creases is visible in a patient with Addison disease. In the bottom left panel, hyperpigmented macules of the gums are visible in this patient with Addison disease. Some patients with Addison disease have vitiligo and hyperpigmentation, as seen in the bottom right panel.
© Springer Science+Business Media
Anorexia, nausea, vomiting, and diarrhea often occur. Decreased tolerance to cold, with hypometabolism, may be noted. Dizziness and syncope may occur.
The gradual onset and nonspecific nature of early symptoms often lead to an incorrect initial diagnosis of neurosis.
Weight loss, dehydration, and hypotension are characteristic of the later stages of Addison disease.
Adrenal crisis
Adrenal crisis is characterized by:
Profound asthenia (weakness)
Severe pain in the abdomen, lower back, or legs
Peripheral vascular collapse
Renal shutdown with azotemia
Body temperature may be low, although severe fever may occur, particularly when crisis is precipitated by acute infection.
A significant number of patients with partial loss of adrenal function (limited adrenocortical reserve) appear well but experience adrenal crises when under physiologic stress (eg, surgery, infection, burns, critical illness). Shock and fever may be the only signs.
Diagnosis of Primary Adrenal Insufficiency
Electrolyte levels
Serum cortisol
Plasma adrenocorticotropic hormone (ACTH)
Sometimes ACTH stimulation testing
This diagnosis is suspected in patients with subacute or chronic symptoms and signs of adrenal insufficiency or for patients in shock with findings consistent with adrenal crisis (eg, hypotension resistant to fluids and vasopressors). The diagnosis may be considered upon discovery of characteristic abnormalities of serum electrolytes, including low sodium, high potassium, low bicarbonate, and high BUN (blood urea nitrogen—see table ).


Test Results That Suggest Primary Adrenal Insufficiency (Addison Disease)
Blood Test | Result |
|---|---|
Metabolic panel | |
Serum sodium | < 135 mEq/L (< 135 mmol/L) |
Serum potassium | > 5 mEq/L (> 5 mmol/L) |
Ratio of serum sodium:potassium | < 30:1 |
Plasma glucose, fasting | < 50 mg/dL (< 2.8 mmol/L) |
Plasma bicarbonate | < 15–20 mEq/L (< 15–20 mmol/L) |
BUN (blood urea nitrogen) | > 20 mg/dL (> 7.1 mmol/L) |
Hematology | |
Hematocrit | Elevated |
White blood cell count | Low |
Lymphocytes | Relative lymphocytosis |
Eosinophils | Increased |
Imaging | |
Radiographs, CT, or MRI of adrenals | Evidence of:
|
Differential diagnosis
The varied manifestations of Addison disease can also be caused by numerous other disorders.
Hyperpigmentation can result from:
Ingestion of heavy metals (eg, iron, silver)
Chronic skin conditions
Hemochromatosis (although the hyperpigmentation of iron overload may be partly due to adrenal insufficiency caused by iron deposition in the adrenals)
Peutz-Jeghers syndrome, which is characterized by pigmentation of the buccal and rectal mucosa
Weakness resulting from Addison disease often subsides with rest. Most myopathies that cause weakness can be differentiated by their distribution, lack of abnormal pigmentation, and characteristic laboratory findings (see also Weakness).
Patients with adrenal insufficiency may develop hypoglycemia after fasting because of decreased gluconeogenesis and often show weight loss, which is not fully understood, but due at least in part to extracellular volume deficiency. Hypoglycemia as a presenting feature is more common in neonates and children. In contrast, patients with hypoglycemia due to oversecretion of insulin usually have increased appetite with weight gain, and have normal adrenal function.
Low serum sodium due to Addison disease must be differentiated from that of edematous patients with heart or liver disease (particularly those taking diuretics), the dilutional hyponatremia of the syndrome of inappropriate antidiuretic hormone (SIAD), and salt-losing nephropathy. Unlike those with Addison disease, these patients are not likely to have hyperpigmentation, hyperkalemia, and increased BUN.
Testing
Adrenal insufficiency is diagnosed based on laboratory tests, beginning with morning serum cortisol and plasma ACTH levels (see table ).
Elevated ACTH (≥ 50 pg/mL [≥ 11 pmol/L]) with low cortisol (< 5 mcg/dL [< 138 nmol/L]) is diagnostic of primary adrenal insufficiency, particularly in patients who are severely stressed or in shock. It is important to note that even in the presence of ACTH levels within the normal range, very low cortisol levels are abnormal and require further evaluation.
Low ACTH (< 5 pg/mL [< 1.1 pmol/L] ) and low cortisol suggest secondary adrenal insufficiency.
If ACTH and cortisol levels are equivocal and adrenal insufficiency is clinically suspected—particularly in a patient who is about to undergo major surgery—provocative testing is required.
If there is insufficient time to evaluate adrenal function (eg, emergency surgery), the patient should be given hydrocortisone empirically (eg, 100 mg IV or IM). Provocative testing is done subsequently.
Provocative testing
Primary adrenal insufficiency is diagnosed by showing failure of exogenous ACTH to increase serum cortisol.
Secondary adrenal insufficiency is diagnosed by a prolonged ACTH stimulation test, glucagon stimulation test, or insulin tolerance test.
If adrenal crisis is suspected, confirmation of primary adrenal insufficiency by ACTH stimulation testing is deferred until the patient has recovered.
In ACTH stimulation testing, cosyntropin (synthetic ACTH) 250 mcg IV or IM is administered. Patients taking glucocorticoids or spironolactone should not take them on the day of the test.
The patient's serum cortisol levels are measured at baseline and 30 and 60 minutes after administration of cosyntropin. Normal preinjection serum cortisol levels vary somewhat depending on the laboratory assay (the normal range should be verified for the laboratory used), but typically range from 5 to 25 mcg/dL (138 to 690 nmol/L). Patients with primary adrenal insufficiency have low or low-normal preinjection values that do not rise above a peak value of 15 to 18 mcg/dL (414 to 497 nmol/L) at 30 minutes.
If peak cortisol levels are < 18 mcg/dL (500 nmol/L) at 30 or 60 minutes, adrenal insufficiency is likely (the exact threshold value is assay-dependent) (1).
A subnormal response to cosyntropin may also occur in secondary adrenal insufficiency. However, because pituitary failure may cause adrenal atrophy (and hence failure to respond to ACTH), if pituitary disease is suspected, the patient may need to be primed with long-acting ACTH 1 mg IM once a day for 3 days before the ACTH stimulation test. After such priming, there should be a normal response to the test with a rise in serum cortisol to > 20 mcg/dL (> 552 nmol/L), although this threshold is assay dependent.
A prolonged ACTH stimulation test (sampling for 24 hours) may be used to diagnose secondary (or tertiary, ie, hypothalamic) adrenal insufficiency. Cosyntropin 1 mg IM is given, and cortisol is measured at baseline and then at intervals after injection for 24 hours, typically at 1, 6, 12, and 24 hours. With secondary adrenal insufficiency, cortisol levels are subnormal levels at 30 and 60 minutes but gradually rise to normal over 24 hours. However, this test is rarely used as reliance is very much on plasma ACTH levels.
Serum cortisol levels are similar for the first hour in both the short (30 to 60 minutes) and prolonged ACTH stimulation tests. However, in primary adrenal insufficiency there is no further rise in cortisol levels after 60 minutes. In secondary and tertiary adrenal insufficiency, cortisol levels continue to rise for ≥ 24 hours.
In the glucagon stimulation test, plasma ACTH and cortisol levels fail to rise in response to glucagon in patients with secondary adrenal insufficiency.
In the insulin tolerance test,, ACTH and cortisol fail to rise in response to enough intravenous regular insulin to cause a reduction in blood glucose to a critical level. The tolerance test carries a risk for hypoglycemic seizure and is not recommended in patients suspected of having severe adrenal insufficiency unless undertaken after a period of glucocorticoid replacement.
Confirmatory Serum Testing for Primary Adrenal Insufficiency (Addison Disease)
Test | Result |
|---|---|
Plasma ACTH | High (≥ 50 pg/mL [≥ 11 pmol/L]) |
Serum cortisol | Low (< 5 mcg/dL [< 138 nmol/L]) |
ACTH stimulation test | Subnormal (ie, 30-minute cortisol should be < 15–18 mcg/dL [< 414–497 nmol/L], according to the assay) |
Prolonged (24-hour) ACTH stimulation test | Cortisol should be subnormal at 1 hour and should not rise further at 24 hours |
ACTH = adrenocorticotropic hormone. | |
Testing for etiology
In areas where granulomatous causes are less likely, the cause is usually assumed to be autoimmune, unless there is evidence otherwise. Adrenal autoantibodies can be assessed. In autoimmune Addison disease, adrenal antibodies are often positive, at least initially.
Where granulomatous causes are more likely, tuberculosis is a common cause, so a chest radiograph should be done; if doubt exists, CT or MRI of the adrenals is helpful. In patients with autoimmune disease, the adrenals are atrophied, whereas in patients with tuberculosis or other granulomas, the adrenals are enlarged (initially) with frequent calcification. Bilateral adrenal hyperplasia, particularly in children and young adults, suggests a genetic enzyme defect. Adrenal hemorrhage is usually obvious on CT scanning.
Diagnosis reference
1. Bornstein SR, Allolio B, Arlt W, et al. Diagnosis and Treatment of Primary Adrenal Insufficiency: An Endocrine Society Clinical Practice Guideline. J Clin Endocrinol Metab. 2016;101(2):364-389. doi:10.1210/jc.2015-1710
Treatment of Primary Adrenal Insufficiency
Hydrocortisone or prednisolone
Fludrocortisone
Dose increase during intercurrent illness
Normally, cortisol is secreted maximally in the early morning and minimally at night. Thus, hydrocortisone (identical to cortisol) is given in 2 or 3 divided doses with a typical total daily dose of 15 to 25 mg (1). One regimen gives half the total in the morning, and the remaining half split between lunchtime and early evening (eg, 10 mg, 5 mg, 5 mg). Others give two-thirds of the dose in the morning and one-third in the evening. Doses immediately before bed should generally be avoided because they may cause insomnia. Alternatively, prednisolone 4 to 5 mg orally in the morning and possibly an additional 2.5 mg orally in the evening may be used. In some patients in whom divided doses fail to approximate the body's normal circadian rhythm of cortisol release, slow-release forms of hydrocortisone may provide more physiological availability of cortisol.
Additionally, fludrocortisone 0.1 to 0.2 mg orally once a day is recommended to replace aldosterone. The easiest way to adjust the fludrocortisone dosage is to titrate it to normalize blood pressure and serum potassium levels. Normal hydration and absence of orthostatic hypotension are evidence of adequate replacement therapy. In some patients, fludrocortisone causes hypertension, which is treated by reducing the dosage or starting a nondiuretic antihypertensive. Adequate doses of fludrocortisone should be given even if use requires the addition of antihypertensives.
Intercurrent illnesses (eg, infections) are potentially serious and should be vigorously treated; the patient’s hydrocortisone dose should be doubled during the illness. If nausea and vomiting preclude oral therapy, parenteral therapy is necessary. Patients should be instructed when to take supplemental prednisolone or hydrocortisone and taught to self-administer parenteral hydrocortisone for urgent situations. A preloaded syringe with 100 mg hydrocortisone should be available to the patient for intramuscular or subcutaneous administration. Identification giving the diagnosis and glucocorticoid dose may help in case of adrenal crisis that renders the patient unable to communicate.
When salt loss is severe, as in very hot climates, the dose of fludrocortisone may need to be increased.
In patients with coexisting diabetes mellitus and Addison disease, the hydrocortisone dose usually should not be > 30 mg/day. Higher doses of hydrocortisone increase insulin requirements.
Treatment of adrenal crisis
Therapy should be instituted immediately upon suspicion of adrenal crisis. (CAUTION: In adrenal crisis, a delay in instituting glucocorticoid therapy, particularly if there is hypoglycemia and hypotension, may be fatal.) If the patient is acutely ill, confirmation by an ACTH stimulation test should be postponed until the patient has recovered, but a single blood sample for measurement for cortisol and ACTH should be obtained.
Hydrocortisone 100 mg is injected IV over 30 seconds and repeated every 6 to 8 hours for the first 24 hours. Immediate intravascular volume expansion is done by giving 1 L of a 5% dextrose in 0.9% saline solution over 1 to 2 hours. Additional 0.9% saline is given IV until hypotension, dehydration, and hyponatremia have been corrected. Serum potassium may fall during rehydration, requiring replacement. Mineralocorticoids are not required when high-dose hydrocortisone is given. Subsequently, hydrocortisone 50 or 100 mg IM every 6 hours can be given.
As an alternative, some centers use a hydrocortisone infusion, giving 1 to 2 mg hydrocortisone per hour with measurement of serum cortisol. Restoration of blood pressure and general improvement should occur within 1 hour after the initial dose of hydrocortisone. Inotropic agents may be needed until the effects of hydrocortisone are achieved.
A total dose of 150 mg hydrocortisone is usually given over the second 24-hour period if the patient has improved markedly, and 75 mg is given on the third day. Maintenance oral doses of hydrocortisone (15 to 20 mg) and fludrocortisone (0.1 mg) are given daily thereafter, as described above.
Recovery depends on treatment of the cause of adrenal crisis (eg, infection, trauma, metabolic stress) and adequate hydrocortisone therapy.
For patients with some residual adrenal function who develop adrenal crisis when under stress, hydrocortisone treatment is the same, but fluid requirements may be much lower.
Pearls & Pitfalls
|
Treatment of complications
Fever occasionally accompanies the rehydration process. An oral antipyretic may be given.
Complications of glucocorticoid therapy may include psychotic reactions. If psychotic reactions occur, then the hydrocortisone dose can be reduced to the lowest level consistent with maintaining blood pressure and good cardiovascular function. Antipsychotics may be temporarily required, but use should not be prolonged.
Treatment reference
1. Bornstein SR, Allolio B, Arlt W, et al. Diagnosis and Treatment of Primary Adrenal Insufficiency: An Endocrine Society Clinical Practice Guideline. J Clin Endocrinol Metab. 2016;101(2):364-389. doi:10.1210/jc.2015-1710
Key Points
Addison disease is primary adrenal insufficiency.
Weakness, fatigue, and hyperpigmentation (generalized darkening or focal black spots involving skin and mucous membranes) are typical.
Low serum sodium, high serum potassium, and high BUN occur.
Usually, plasma adrenocorticotropic hormone (ACTH) is high and serum cortisol levels are low.
Replacement doses of hydrocortisone and fludrocortisone are given; doses should be increased during intercurrent illness.
Drug Information for the Topic





