

Central retinal artery occlusion occurs when the central retinal artery becomes blocked, usually due to an embolus. It causes sudden, painless, monocular and usually severe vision loss. Diagnosis is by history and characteristic retinal findings on funduscopy. Intraocular pressure can be decreased within the first 24 hours of occlusion to attempt to dislodge the embolus. If patients present within the first few hours of occlusion, some centers catheterize the carotid/ophthalmic artery and selectively inject thrombolytic medications.
Etiology of Retinal Artery Occlusion
Retinal artery occlusion may be due to embolism, thrombosis, or vasculitis.
Emboli may come from any of the following:
Atherosclerotic plaques
Fat
Atrial myxoma
Atherosclerotic plaques within the carotid artery are a common source of emboli leading to retinal artery occlusion and should prompt systemic vascular evaluation in patients with retinal artery occlusion. Systemic vasculitis, particularly giant cell arteritis, is an important cause of arterial occlusion that requires prompt diagnosis and treatment. Retinal artery occlusion has also been observed in other autoimmune diseases such as systemic lupus erythematosus.
Occlusion can affect a branch of the retinal artery as well as the central retinal artery.
Neovascularization (abnormal new vessel formation) of the retina or iris (rubeosis iridis) with secondary (neovascular) glaucoma occurs in approximately 15 to 20% of patients within weeks to months after occlusion (1). Vitreous hemorrhage may result from retinal neovascularization.
Risk of stroke is increased after retinal artery occlusion, particularly in the first weeks.
Etiology reference
1. Duker JS, Brown GC. Iris neovascularization associated with obstruction of the central retinal artery. Ophthalmology. 1988;95(9):1244-1250. doi: 10.1016/s0161-6420(88)33042-3
Symptoms and Signs of Retinal Artery Occlusion
Retinal artery occlusion causes sudden, painless, monocular vision loss.
The pupil may respond poorly to direct light but constricts briskly when the other eye is illuminated (relative afferent pupillary defect). -Funduscopy shows a pale, opaque fundus with a red fovea (cherry-red spot); the cherry red spot does not persist and so may not be seen if the exam is done after the acute period. Typically, the arteries are attenuated and may even appear bloodless. An embolus (eg, a cholesterol embolus, called a Hollenhorst plaque) is sometimes visible. If a major branch is occluded rather than the entire artery, fundus abnormalities and vision loss are limited to that sector of the retina.
Patients who have giant cell arteritis are typically 55 years or older and may have a headache, a tender and palpable temporal artery, jaw claudication, fatigue, or a combination.
Diagnosis of Retinal Artery Occlusion
History and physical examination
Sometimes, color fundus photography and fluorescein angiography

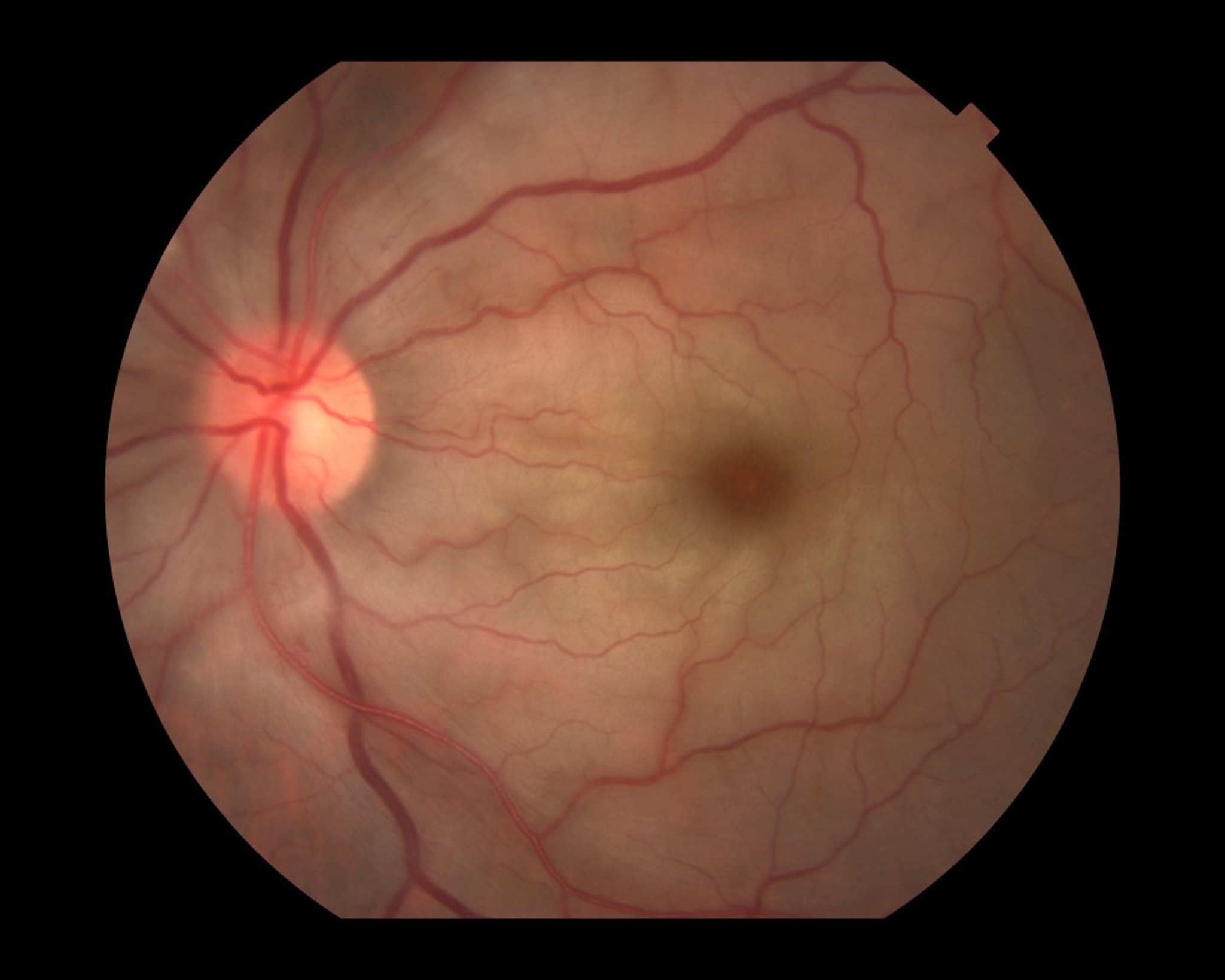
In acute central retinal artery occlusion, diffuse retinal edema makes the retina appear pale and the arteries become attenuated. The underlying perfused choroid shows through the thin fovea, giving the classic cherry-red spot appearance.
Paul Whitten/SCIENCE PHOTO LIBRARY
The diagnosis is suspected when a patient has acute, painless, severe, vision loss (usually monocular). Funduscopy is usually confirmatory. Fluorescein angiography is often done and shows absence of perfusion in the affected artery. However, if patients present with acute transient monocular vision loss thought to be due to a thromboembolic event, imaging tests take unnecessary time and should be deferred if the diagnosis is clear.The diagnosis is suspected when a patient has acute, painless, severe, vision loss (usually monocular). Funduscopy is usually confirmatory. Fluorescein angiography is often done and shows absence of perfusion in the affected artery. However, if patients present with acute transient monocular vision loss thought to be due to a thromboembolic event, imaging tests take unnecessary time and should be deferred if the diagnosis is clear.
Once the diagnosis is made, carotid Doppler ultrasound and echocardiography should be performed to identify an embolic source so that further embolization can be prevented.
If giant cell arteritis is suspected (eg, in patients older than 50 years, particularly those who have symptoms such as headache, scalp tenderness, jaw pain, fever, fatigue, and unintended weight loss), erythrocyte sedimentation rate, C-reactive protein, and platelet count should be performed immediately. These tests may not be necessary if an embolic plaque is visible in the central retinal artery.
Because risk of stroke is increased, some centers rapidly evaluate patients similarly to those who have had stroke or transient ischemic attack.
Treatment of Retinal Artery Occlusion
Reduction of intraocular pressure
Pearls & Pitfalls
|
If acute thromboembolism is suspected, the patient should be referred immediately to a specialized stroke center because there is an increased risk of other cerebrovascular events.
Immediate treatment is indicated if occlusion occurred within 24 hours of presentation. Ocular massage with intermittent pressure on the closed eye or reduction of intraocular pressure with ocular hypotensive medications (eg, topical timolol 0.5%, acetazolamide 500 mg IV or orally) may dislodge an embolus and allow it to enter a smaller branch of the artery, thus reducing the area of retinal ischemia. Anterior chamber paracentesis is sometimes used to reduce intraocular pressure and increase perfusion. Immediate treatment is indicated if occlusion occurred within 24 hours of presentation. Ocular massage with intermittent pressure on the closed eye or reduction of intraocular pressure with ocular hypotensive medications (eg, topical timolol 0.5%, acetazolamide 500 mg IV or orally) may dislodge an embolus and allow it to enter a smaller branch of the artery, thus reducing the area of retinal ischemia. Anterior chamber paracentesis is sometimes used to reduce intraocular pressure and increase perfusion.
Some centers have tried infusing thrombolytics into the carotid artery to dissolve the obstructing clot. In collaboration with an acute stroke team, early administration of IV tissue plasminogen activator (tPA) can be considered in selected patients; evidence remains limited and decisions are individualized (1, 2).
Multiple case series have suggested that hyperbaric oxygen may improve visual outcome in central retinal artery occlusion (3).
Surgical or laser-mediated embolectomy is available but not commonly done. These treatments are sometimes shown to be effective in small case series, but none have strong evidence to support efficacy (4).
Patients with occlusion secondary to giant cell arteritis should receive high-dose systemic glucocorticoids.
Treatment references
1. Dumitrascu OM, Newman NJ, Biousse V. Thrombolysis for Central Retinal Artery Occlusion in 2020: Time Is Vision! J Neuroophthalmol. 2020;40(3):333-345. doi:10.1097/WNO.0000000000001027
2. Ryan SJ, Jørstad ØK, Skjelland M, et al. A Randomized Trial of Tenecteplase in Acute Central Retinal Artery Occlusion. N Engl J Med. 2026;394(5):442-450. doi:10.1056/NEJMoa2508515
3. Masters TC, Westgard BC, Hendriksen SM, et al. CASE SERIES OF HYPERBARIC OXYGEN THERAPY FOR CENTRAL RETINAL ARTERY OCCLUSION. Retin Cases Brief Rep. 2021;15(6):783-788. doi:10.1097/ICB.0000000000000895
4. Chen C, Singh G, Madike R, Cugati S. Central retinal artery occlusion: a stroke of the eye. Eye (Lond). 2024;38(12):2319-2326. doi:10.1038/s41433-024-03029-w
Prognosis for Retinal Artery Occlusion
Patients with a branch artery occlusion may maintain good to fair vision, but with central artery occlusion, vision loss is often profound, even with treatment. Once retinal infarction occurs (as quickly as 90 minutes after the occlusion [1]), vision loss is permanent.
If underlying giant cell arteritis is diagnosed and treated promptly, the vision in the uninvolved eye can often be protected and some vision may be recovered in the affected eye.
Prognosis reference
1. Hayreh SS, Zimmerman MB, Kimura A, et al. Central retinal artery occlusion. Retinal survival time. Exp Eye Res. 2004;78(3):723-736. doi: 10.1016/s0014-4835(03)00214-8
Key Points
Central or branch retinal artery occlusion can be caused by an embolus (eg, due to atherosclerosis or endocarditis), thrombosis, or giant cell arteritis.
Painless, severe loss of vision affects part or all of the visual field.
Confirm the diagnosis by doing funduscopy (typically showing a pale, opaque fundus with a red fovea and arterial attenuation).
Immediately refer patients with acute thromboembolic events to a specialized stroke center.
Reserve color fundus photography and fluorescein angiography for diagnostic confirmation only if diagnosis not apparent, and search for an embolic source by doing Doppler ultrasound and echocardiography.Reserve color fundus photography and fluorescein angiography for diagnostic confirmation only if diagnosis not apparent, and search for an embolic source by doing Doppler ultrasound and echocardiography.
Treat immediately if possible with ocular hypotensive medications (eg, topical timolol or IV or oral acetazolamide), intermittent digital massage over the closed eyelid, anterior chamber paracentesis, or hyperbaric oxygen if available.Treat immediately if possible with ocular hypotensive medications (eg, topical timolol or IV or oral acetazolamide), intermittent digital massage over the closed eyelid, anterior chamber paracentesis, or hyperbaric oxygen if available.
Drug Information for the Topic





