



Central retinal vein occlusion is a blockage of the central retinal vein by a thrombus. It causes painless vision loss, ranging from mild to severe, and usually occurs suddenly. Diagnosis is by funduscopy. Treatments can include antivascular endothelial growth factor medications (eg, ranibizumab, bevacizumab), a dexamethasone implant, intraocular injection of triamcinolone, and laser photocoagulation.
Etiology of Retinal Vein Occlusion
Major risk factors include:
Older age
Other risk factors include:
Occlusion may also be idiopathic. The condition is uncommon among young people. Occlusion may affect a branch of the retinal vein or the central retinal vein.
Neovascularization (abnormal new vessel formation) of the retina or iris (rubeosis iridis) occurs in approximately 16% of patients with central retinal vein occlusion (1) and can result in secondary (neovascular) glaucoma, which can occur weeks to months after occlusion. Vitreous hemorrhage may result from retinal neovascularization.
Etiology reference
1. The Central Vein Occlusion Study Group. Natural history and clinical management of central retinal vein occlusion. Arch Ophthalmol. 1997;115(4):486-91. doi: 10.1001/archopht.1997.01100150488006
Symptoms and Signs of Retinal Vein Occlusion
Painless vision loss is usually sudden, but it can also occur gradually over a period of days to weeks. Vision loss is usually monocular, although bilateral central vein occlusion occurs infrequently and can cause bilateral vision loss. Funduscopy reveals hemorrhages throughout the retina, engorged (dilated) and tortuous retinal veins, and, usually, significant retinal edema. These changes are typically diffuse if obstruction involves the central retinal vein and are limited to one quadrant if obstruction involves only a branch of the central retinal vein.

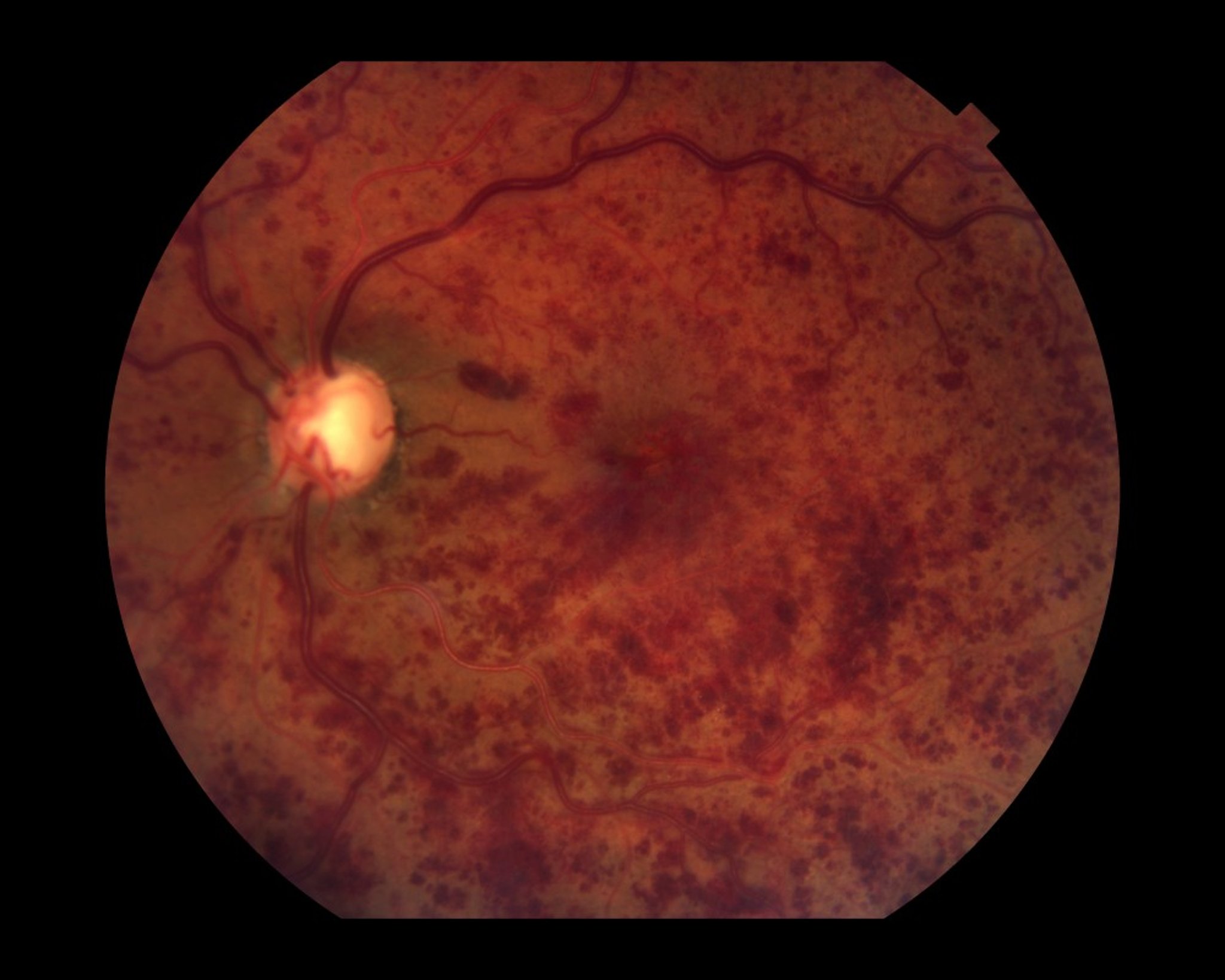
In central retinal vein occlusion, retinal veins appear dilated and tortuous. The fundus may appear congested and edematous. Numerous retinal hemorrhages are also characteristic.
Paul Whitten/SCIENCE PHOTO LIBRARY
Diagnosis of Retinal Vein Occlusion
Funduscopy
Color fundus photography
Fluorescein angiography
Optical coherence tomography
The diagnosis is suspected in patients with painless vision loss (usually in one eye,) particularly those with risk factors. Funduscopy, and if necessary, fluorescein angiography confirm the diagnosis. Optical coherence tomography is used to determine the degree of macular edema and its response to treatment. Patients with a central retinal vein occlusion are evaluated for hypertension and glaucoma and tested for diabetes. Younger patients are tested for increased blood viscosity (with a complete blood count and clotting factors as deemed necessary).
Treatment of Retinal Vein Occlusion
For macular edema, intraocular injection of antivascular endothelial growth factor (anti-VEGF) medications, dexamethasone implant, and/or triamcinolone acetonide
For some cases of macular edema with branch retinal vein occlusion, focal laser photocoagulation
Panretinal laser photocoagulation if neovascularization develops
Treatment for branch retinal vein occlusion in patients with macular edema that involves the fovea is usually intraocular injection of an anti-VEGF medication (eg, ranibizumab, aflibercept, high-dose aflibercept, bevacizumab, or faricimab), intraocular injection of triamcinolone, or a slow-release dexamethasone implant (1). These treatments can also be used to treat central retinal vein occlusion in patients with macular edema. With these treatments, vision improves significantly in 50% of patients with macular edema from branch retinal vein occlusion (2).
Focal laser photocoagulation can be used for branch retinal vein occlusion with macular edema (3) but is less effective than intraocular injection of an anti-VEGF medication or a dexamethasone implant. Focal laser photocoagulation is typically not effective for the treatment of macular edema due to a central retinal vein occlusion.
If retinal or anterior segment neovascularization develops secondary to central or branch retinal vein occlusion, panretinal laser photocoagulation should be done promptly to decrease vitreous hemorrhage and prevent neovascular glaucoma.
Treatment references
1. Danzig CJ, Dinah C, Ghanchi F, et al. Faricimab Treat-and-Extend Dosing for Macular Edema Due to Retinal Vein Occlusion: 72-Week Results from the BALATON and COMINO Trials. Ophthalmol Retina. 2025;9(9):848-859. doi:10.1016/j.oret.2025.03.005
2. Kim M, Lee DH, Byeon SH, et al. Comparison of intravitreal bevacizumab and dexamethasone implant for the treatment of macula oedema associated with branch retinal vein occlusion. Br J Ophthalmol. 2015;99(9):1271-1276. doi: 10.1136/bjophthalmol-2014-306236
3. The Branch Vein Occlusion Study Group. Argon laser photocoagulation for macular edema in branch vein occlusion. Am J Ophthalmol. 1984;98(3):271-282. doi: 10.1016/0002-9394(84)90316-7
Prognosis for Retinal Vein Occlusion
Most patients have some visual deficit. In mild cases, there can be spontaneous improvement to near-normal vision over a variable period of time. Visual acuity at presentation is a good indicator of final vision. If visual acuity is at least 20/40, visual acuity will likely remain good, occasionally near normal. If visual acuity is worse than 20/200, it will remain at that level or worsen in 80% of patients (1). Central retinal vein occlusions rarely recur.
Prognosis reference
1. La Spina C, De Benedetto U, Parodi MB, et al. Practical management of retinal vein occlusions. Ophthalmol Ther. 2012;1(1):3. doi: 10.1007/s40123-012-0003-y
Key Points
Retinal vein occlusion involves blockage by a thrombus.
Patients have painless loss of vision that is typically sudden and may have risk factors (eg, older age, hypertension).
Funduscopy characteristically demonstrates macular edema with dilated veins and hemorrhages; additional tests include color fundus photography, fluorescein angiography, and optical coherence tomography.
Treat patients who have macular edema with an intraocular injection of an anti-VEGF medication (ranibizumab, aflibercept, or bevacizumab) or intraocular injection of a dexamethasone implant or triamcinolone.
Focal laser photocoagulation is useful in some cases of macular edema secondary to a branch retinal vein occlusion, and panretinal laser photocoagulation should be done for retinal or anterior segment neovascularization.
Drug Information for the Topic





