



Malabsorption is inadequate assimilation of dietary substances due to defects in digestion, absorption, or transport.
Malabsorption can affect macronutrients (eg, proteins, carbohydrates, fats), micronutrients (eg, vitamins, minerals), or both, causing excessive fecal excretion, nutritional deficiencies, and gastrointestinal (GI) symptoms. Malabsorption may be global, with impaired absorption of almost all nutrients, or partial (isolated), with malabsorption of only specific nutrients.
Pathophysiology of Malabsorption
Digestion and absorption occur in 3 phases:
Intraluminal hydrolysis of fats, proteins, and carbohydrates by enzymes—bile salts enhance the solubilization of fat in this phase
Digestion by brush border enzymes and uptake of end products
Lymphatic transport of nutrients
The term malabsorption is commonly used when any of these phases is impaired, although impairment of phase 1 is technically maldigestion rather than malabsorption.
Digestion of fats
Pancreatic enzymes (lipase and colipase) split long-chain triglycerides into fatty acids and monoglycerides, which combine with bile acids and phospholipids to form micelles that pass through jejunal enterocytes. Absorbed fatty acids are resynthesized and combined with protein, cholesterol, and phospholipid to form chylomicrons, which are transported by the lymphatic system. Medium-chain triglycerides are absorbed directly.
Unabsorbed fats trap fat-soluble vitamins (A, D, E, K) and possibly some minerals, causing deficiency. Bacterial overgrowth results in deconjugation and dehydroxylation of bile salts, limiting the absorption of fats. Unabsorbed bile salts stimulate water secretion in the colon, causing diarrhea.
Digestion of carbohydrates
The pancreatic enzyme amylase and brush border enzymes on microvilli lyse carbohydrates and disaccharides into constituent monosaccharides. Colonic bacteria ferment unabsorbed carbohydrates into carbon dioxide, methane, hydrogen, and short-chain fatty acids (butyrate, propionate, acetate, and lactate). These fatty acids cause diarrhea. The gases cause abdominal distention and bloating.
Digestion of proteins
Gastric pepsin initiates digestion of proteins in the stomach and also stimulates release of the cholecystokinin critical to the secretion of pancreatic enzymes. Enterokinase, a brush border enzyme, activates trypsinogen into trypsin, which converts many pancreatic proteases into their active forms. Active pancreatic enzymes hydrolyze proteins into oligopeptides, which are absorbed directly or hydrolyzed into amino acids.
Etiology of Malabsorption
Malabsorption has many causes (see table ). Some malabsorptive disorders (eg, celiac disease) impair the absorption of most nutrients, vitamins, and trace minerals (global malabsorption); others (eg, pernicious anemia) are more selective.
Pancreatic insufficiency causes malabsorption if > 90% of function is lost. Increased luminal acidity (eg, Zollinger-Ellison syndrome) inhibits lipase and fat digestion. Cirrhosis and cholestasis reduce hepatic bile synthesis or delivery of bile salts to the duodenum, causing malabsorption. Other causes are discussed elsewhere in this chapter.
Acute bacterial, viral, and parasitic infections (see also Overview of Gastroenteritis) may cause transient malabsorption, probably as a result of temporary, superficial damage to the villi and microvilli.
Chronic bacterial infections of the small bowel are uncommon, apart from blind loops, systemic sclerosis, and diverticula, where small intestinal bacterial overgrowth (SIBO) can occur. Intestinal bacteria may use up dietary vitamin B12 and other nutrients, perhaps interfere with enzyme systems, and cause mucosal injury.
Causes of Malabsorption
Mechanism | Cause |
|---|---|
Inadequate gastric mixing, rapid emptying, or both | Billroth II gastrectomy Gastrocolic fistula Gastroenterostomy |
Insufficient digestive agents | Autoimmune metaplastic atrophic gastritis Biliary obstruction and cholestasis Cholestyramine-induced bile acid loss Pancreatic resection Sucrase-isomaltase deficiency |
Abnormal milieu | Abnormal motility secondary to diabetes, systemic sclerosis, hypothyroidism, or hyperthyroidism Small intestinal bacterial overgrowth (eg, due to blind loops, diverticula in the small intestine) Zollinger-Ellison syndrome (low duodenal pH) |
Acutely abnormal epithelium | Acute intestinal infections Alcohol Neomycin |
Chronically abnormal epithelium | Ischemia Radiation enteritis |
Intestinal resection (eg, for Crohn disease, volvulus, intussusception, or infarction) Jejunoileal bypass for obesity | |
Impaired transport | Blocked lacteals due to lymphoma or tuberculosis Intrinsic factor deficiency (as in pernicious anemia) |
Symptoms and Signs of Malabsorption


The effects of unabsorbed substances, especially in global malabsorption, include diarrhea, steatorrhea, abdominal bloating, and gas. Other symptoms result from nutritional deficiencies. Patients often lose weight despite adequate food intake.
Chronic diarrhea is the most common symptom and is what usually prompts evaluation of the patient. Steatorrhea—fatty stool, the hallmark of malabsorption—occurs when > 7 g/day of fat are excreted. Steatorrhea causes foul-smelling, pale, bulky, and greasy stools.
Severe vitamin and mineral deficiencies occur in advanced malabsorption; symptoms are related to the specific nutrient deficiency (see table ). Vitamin B12 deficiency may occur in blind loop syndrome or after extensive resection of the distal ileum or stomach. Iron deficiency may be the only symptom in a patient with mild malabsorption.
Symptoms of Malabsorption
Symptom | Malabsorbed Nutrient |
|---|---|
Anemia (hypochromic, microcytic) | Iron |
Anemia (macrocytic) | Vitamin B12, folate |
Bleeding, bruising, petechiae | Vitamins K and C |
Carpopedal spasm | Calcium, magnesium |
Edema | Protein |
Glossitis | Vitamins B1, B2, B3, B6, and B12, folate, niacin, iron |
Night blindness | Vitamin A |
Pain in limbs, bones, pathologic fractures | Potassium, magnesium, calcium, vitamin D |
Peripheral neuropathy | Vitamins B1, B6, B12 |
Amenorrhea may result from undernutrition and is an important manifestation of celiac disease in young women.
Diagnosis of Malabsorption
Diagnosis typically clinically apparent from a detailed patient history
Blood tests to screen for consequences of malabsorption
Stool fat testing to confirm malabsorption (if unclear)
Cause diagnosed with endoscopy, contrast radiography, or other tests based on findings
Malabsorption is suspected in a patient with chronic diarrhea, weight loss, and anemia. The etiology is sometimes obvious. For example, patients with malabsorption due to chronic pancreatitis usually have had prior bouts of acute pancreatitis. Patients with celiac disease can present with classic lifelong diarrhea exacerbated by gluten products and may have dermatitis herpetiformis. Patients with cirrhosis and pancreatic cancer can present with jaundice. Abdominal distention, excessive flatus, and watery diarrhea occurring 30 to 90 minutes after carbohydrate ingestion suggest deficiency of a disaccharidase enzyme, usually lactase. Previous extensive abdominal operations suggest short bowel syndrome.
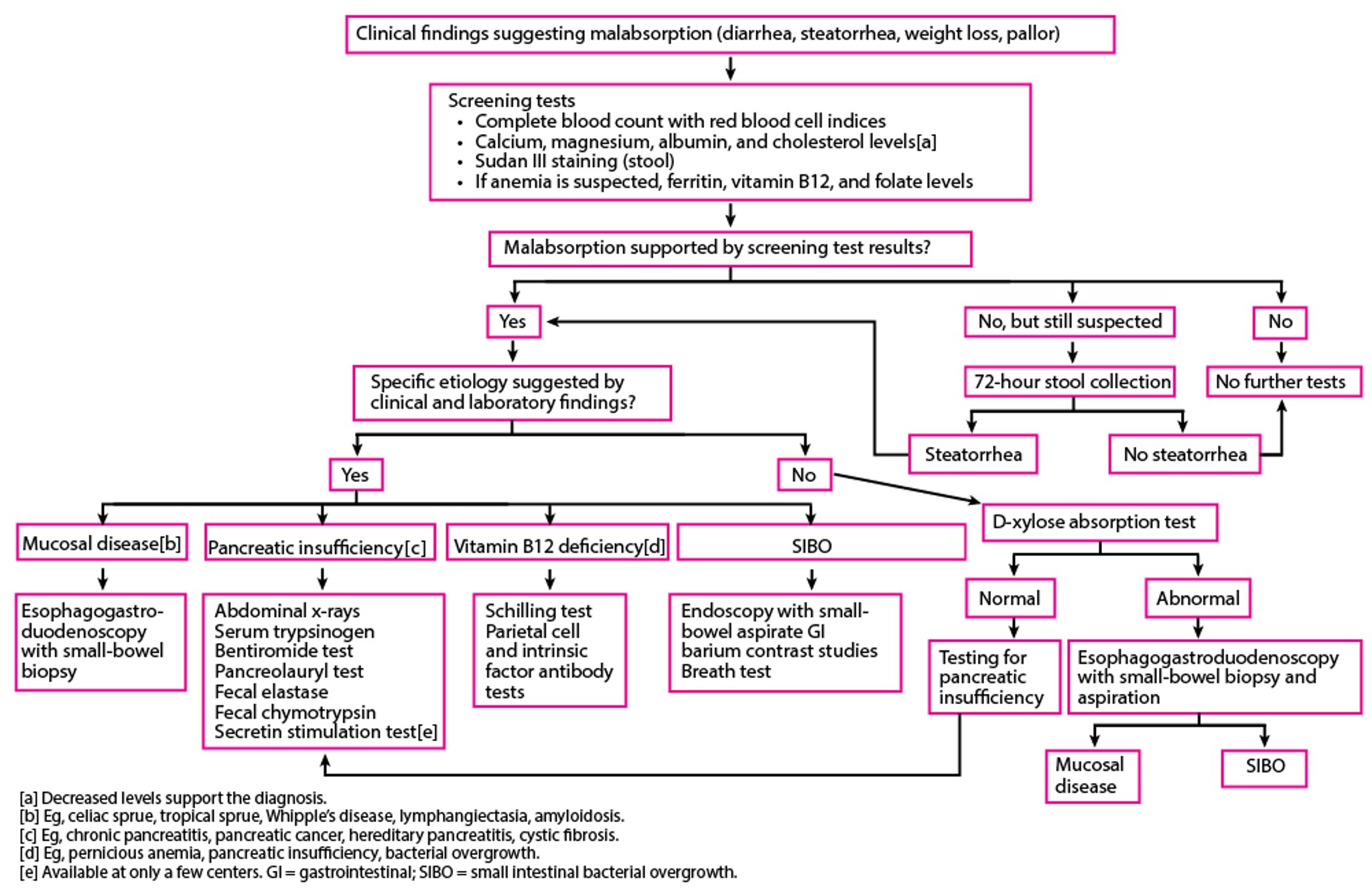
If the history suggests a specific cause, testing should be directed to that condition (see figure ).
If no cause is readily apparent, blood tests can be used as screening tools (eg, complete blood count, red blood cell indices, ferritin, vitamin B12, folate, calcium, albumin, cholesterol, prothrombin time). Test results may suggest a diagnosis and direct further investigation.
Suggested Evaluation for Malabsorption

Macrocytic anemia should prompt measurement of serum folate and B12 levels. Folate deficiency is common in mucosal disorders involving the proximal small bowel (eg, celiac disease, tropical sprue, Whipple disease). Low B12 levels can occur in pernicious anemia, chronic pancreatitis, small intestinal bacterial overgrowth (SIBO), and terminal ileal disease. A combination of low B12 and high folate levels is suggestive of SIBO, because intestinal bacteria use vitamin B12 and synthesize folate.
Microcytic anemia suggests iron deficiency, which may occur with celiac disease. Albumin is a general indicator of nutritional state. Low albumin can result from poor intake, decreased synthesis in cirrhosis, or protein wasting. Low serum carotene (a precursor of vitamin A) suggests malabsorption if intake is adequate.
Confirming malabsorption
Tests to confirm malabsorption are appropriate when symptoms are vague and the etiology is not apparent. Most tests for malabsorption assess fat malabsorption because it is relatively easy to measure. Confirmation of carbohydrate malabsorption is not helpful once steatorrhea is documented. Tests for protein malabsorption are rarely used because fecal nitrogen is difficult to measure.
Direct measurement of fecal fat from a 72-hour stool collection is the gold standard test for establishing steatorrhea but unnecessary with gross steatorrhea of obvious cause. However, this test is available routinely in only a few centers. Stool is collected for a 3-day period during which the patient consumes ≥ 100 g fat/day. Total fat in the stool is measured. Fecal fat > 7 g/day is abnormal. Although severe fat malabsorption (fecal fat ≥ 40 g/day) suggests pancreatic insufficiency or small-bowel mucosal disease, this test cannot determine the specific cause of malabsorption. Some test results include a fractional fat excretion that is defined as the average grams of stool fat excreted per day divided by the average grams of fat consumed per day. A fractional fat excretion of > 7% indicates fat malabsorption. Because the test is messy, unpleasant, and time-consuming, it is unacceptable to most patients and difficult to do.
Sudan III staining of a stool smear is a simple and direct, but nonquantitative, screening test for fecal fat. Acid steatocrit is a gravimetric assay performed on a single stool sample. Near-infrared reflectance analysis (NIRA) simultaneously tests stool for fat, nitrogen, and carbohydrates. These tests are not widely available in the United States.
Measurement of elastase and chymotrypsin in the stool can also help differentiate pancreatic and intestinal causes of malabsorption; both are decreased in pancreatic exocrine insufficiency, whereas both are normal in intestinal causes.
The D-xylose absorption test can be performed if the etiology is not obvious; however, it is currently rarely used because of the advent of advanced endoscopic and imaging tests. Although it can noninvasively assess intestinal mucosal integrity and help differentiate mucosal from pancreatic disease, an abnormal D-xylose test result requires an endoscopic examination with biopsies of the small-bowel mucosa. As a result, small-bowel biopsy has replaced this test to establish intestinal mucosal disease.
D-xylose is absorbed by passive diffusion and does not require pancreatic enzymes for digestion. A normal D-xylose test result in the presence of moderate to severe steatorrhea indicates pancreatic exocrine insufficiency rather than small-bowel mucosal disease. SIBO can cause abnormal results because the enteric bacteria metabolize pentose, thus decreasing the D-xylose available for absorption.
After fasting, the patient is given D-xylose in water orally. Urine is collected over 5 hours, and a venous sample is obtained after 1 hour. Low serum (< 20 mg/dL or 1.33 mmol/L) or urine (< 4 g) D-xylose indicates abnormal absorption. Falsely low levels can also occur in renal diseases, portal hypertension, ascites, or delayed gastric emptying time.
Diagnosing the cause of malabsorption
More specific diagnostic tests (eg, upper endoscopy, colonoscopy, barium radiography) are indicated to diagnose several causes of malabsorption.
Upper endoscopy with small-bowel biopsy is performed when mucosal disease of the small bowel is suspected or if the D-xylose test result is abnormal in a patient with massive steatorrhea. Endoscopy allows visual assessment of small-bowel mucosa and helps direct biopsies to affected areas. Aspirate from the small bowel can be sent for bacterial culture and colony count to document bacterial overgrowth if there is clinical suspicion.
Video capsule endoscopy can be used to look for diseases of the distal small intestine that are beyond the reach of a regular endoscope.
Histologic features on small-bowel biopsy (see table ) can establish the specific mucosal disease.
Small-Bowel Mucosal Histology in Certain Malabsorptive Disorders
Disorder | Histologic Characteristics |
|---|---|
Normal | Fingerlike villi with a villous:crypt ratio of about 4:1 Columnar epithelial cells with numerous regular microvilli (brush border) Mild round cell infiltration in the lamina propria |
Celiac disease (untreated) | Virtual absence of villi and elongated crypts Increased intraepithelial lymphocytes and round cells (especially plasma cells) in the lamina propria Cuboidal epithelial cells with scanty, irregular microvilli |
Dilation and ectasia of the intramucosal lymphatics | |
Range from minimal changes in villous height and moderate epithelial cell damage to virtual absence of villi and elongated crypts with lymphocyte infiltration in the lamina propria | |
Lamina propria densely infiltrated with periodic acid-Schiff–positive macrophages Villous structure possibly obliterated in severe lesions |
Small-bowel contrast imaging (eg, small-bowel follow-through, enteroclysis, CT enterography, magnetic resonance enterography) can detect anatomic conditions that predispose to bacterial overgrowth. These include jejunal diverticula, fistulas, surgically created blind loops and anastomoses, ulcerations, and strictures. These imaging studies may also detect mucosal abnormalities. Abdominal flat plate radiographs may show pancreatic calcifications indicative of chronic pancreatitis. Barium contrast studies of the small bowel are neither sensitive nor specific but may show findings suggestive of mucosal disease (eg, dilated small-bowel loops, thinned or thickened mucosal folds, coarse fragmentation of the barium column). CT, magnetic resonance cholangiopancreatography (MRCP), and endoscopic retrograde cholangiopancreatography can establish the diagnosis of chronic pancreatitis.
Tests for pancreatic insufficiency (eg, secretin stimulation test, bentiromide test, pancreolauryl test, serum trypsinogen, fecal elastase, fecal chymotrypsin) are performed if history is suggestive but are not sensitive for mild pancreatic disease.
Breath tests help diagnose bacterial overgrowth. The glucose-hydrogen and lactulose-hydrogen breath tests are most commonly used. These tests are performed to measure the exhaled hydrogen and methane produced by the bacterial degradation of carbohydrates. In patients with disaccharidase deficiencies, enteric bacteria degrade nonabsorbed carbohydrates in the colon, increasing exhaled hydrogen. The hydrogen breath tests have replaced bacterial cultures of aspirates taken during endoscopy for diagnosis of SIBO. The lactose-hydrogen breath test is useful only to confirm lactase deficiency and is not used as an initial diagnostic test in the evaluation of malabsorption.
The Schilling test is performed to assess malabsorption of vitamin B12. The 4 stages of this test are used to determine whether the deficiency results from pernicious anemia, pancreatic exocrine insufficiency, bacterial overgrowth, or ileal disease.
Stage 1: The patient is given 1 mcg of radiolabeled cyanocobalamin orally concurrent with 1000 mcg of nonlabeled cobalamin IM to saturate hepatic binding sites. A 24-hour urine collection is analyzed for radioactivity; urinary excretion of < 8% of the oral dose indicates malabsorption of cobalamin.
Stage 2: If stage 1 is abnormal, the test is repeated with the addition of intrinsic factor. Pernicious anemia is present if intrinsic factor normalizes absorption.
Stage 3: Stage 3 is performed after adding pancreatic enzymes; normalization in this stage indicates cobalamin malabsorption secondary to pancreatic insufficiency.
Stage 4: Stage 4 is performed after antimicrobial therapy with anaerobic coverage; normalization after antibiotics suggests SIBO.
Cobalamin deficiency secondary to ileal disease or ileal resection results in abnormalities in all stages.
Tests for less common causes of malabsorption include serum gastrin (Zollinger-Ellison syndrome), intrinsic factor and parietal cell antibodies (pernicious anemia), sweat chloride (cystic fibrosis), lipoprotein electrophoresis (abetalipoproteinemia), and serum cortisol (Addison disease).
To diagnose bile acid malabsorption, which may occur with diseases of the terminal ileum (eg, Crohn disease, extensive resection of terminal ileum), patients can be given a therapeutic trial of a bile acid binding resin (eg, cholestyramine). Alternatively, the selenium-75–labeled homocholic acid taurine (SeHCAT) test can be performed. In this test, selenium-75–labeled synthetic bile acid is given orally and, after 7 days, the retained bile acid is measured with a whole-body scan or gamma camera. If bile acid absorption is abnormal, retention is less than 5%. The SeHCAT test is not available in many countries, including the United States.
Drug Information for the Topic





