



Testicular torsion is an emergency condition due to rotation of the testis and consequent strangulation of its blood supply. Symptoms are acute scrotal pain and swelling, nausea, and vomiting. Diagnosis is based on physical examination and confirmed by color Doppler ultrasound. Treatment is immediate manual detorsion followed by surgical intervention.
Anomalous development of the tunica vaginalis and spermatic cord can lead to incomplete fixation of the testis to the tunica vaginalis (bell-clapper deformity—see figure ). This anomaly predisposes the testis to twisting on its cord spontaneously or after trauma. The predisposing anomaly is present in approximately 5 to 16% of males (1).
Torsion is most common between the ages of 12 and 18 years, with a secondary peak in infancy. The annual incidence of testicular torsion is 3.8 per 100,000 in males younger than 18 years (2). It is uncommon in males > age 30 years. It is more common in the left testis.
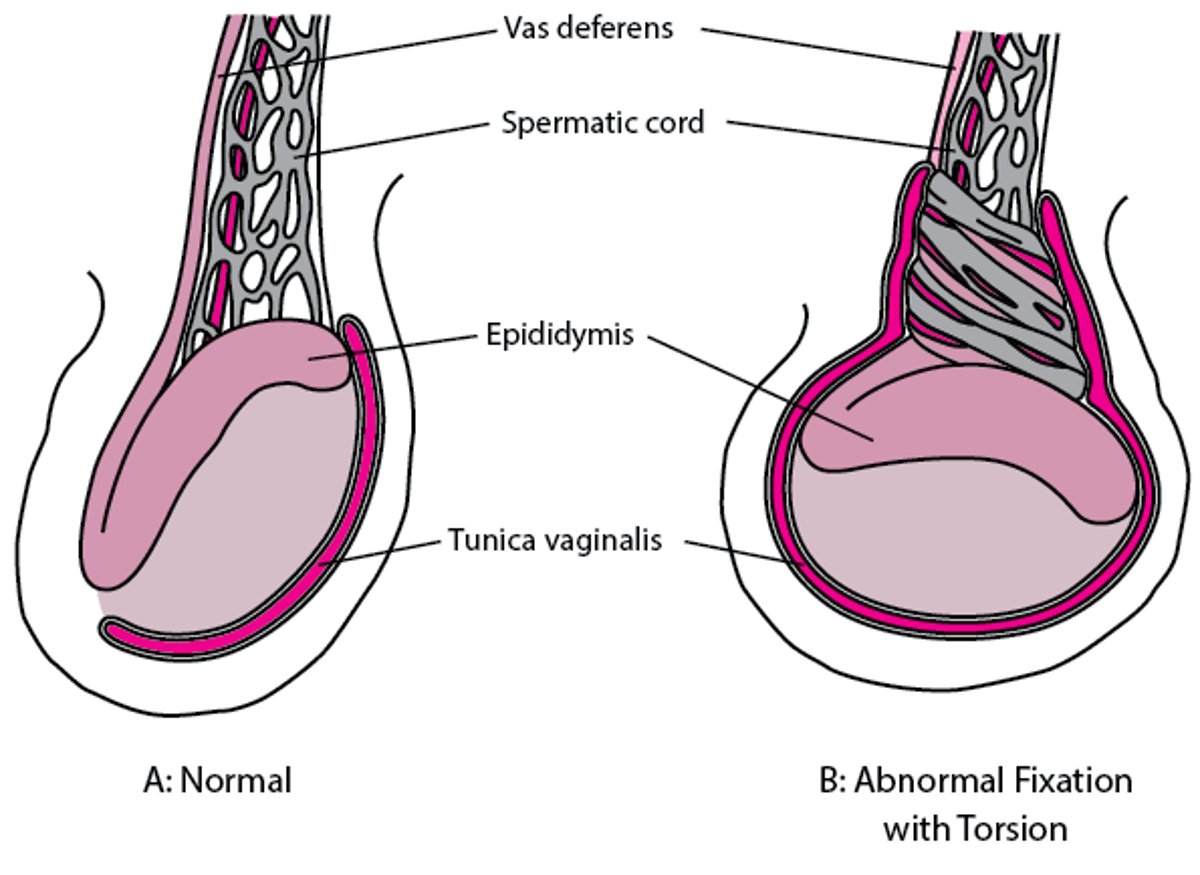
Abnormal Testicular Fixation Leading to Torsion
Typically, the anterior two-thirds of each testis is covered by the tunica vaginalis, where fluids can accumulate. The tunica vaginalis attaches to the posterolateral surface of the testes and limits their movement within the scrotum. If the fixation is too high (anterior and cephalad), the testes can move more freely and torsion is more likely. A: Fixation is normal. B: Fixation is too high, allowing the testis to rotate transversely and resulting in torsion. |

General references
1. Taghavi K, Dumble C, Hutson JM, Mushtaq I, Mirjalili SA. The bell-clapper deformity of the testis: The definitive pathological anatomy. J Pediatr Surg. 2021;56(8):1405-1410. doi:10.1016/j.jpedsurg.2020.06.023
2. Sharp VJ, Kieran K, Arlen AM. Testicular torsion: diagnosis, evaluation, and management. Am Fam Physician. 2013;88(12):835-840.
Symptoms and Signs of Testicular Torsion
Immediate symptoms are rapid onset of severe local pain, nausea, and vomiting, followed by scrotal edema and induration. Fever and urinary frequency may be present. The testis is tender and may be elevated and horizontal. The contralateral testis may also be horizontal because the anatomic defect is usually bilateral. The cremasteric reflex is usually absent on the affected side. Sometimes, torsion can spontaneously resolve and then recur, which may appear to suggest a less acute onset (1). Usually, however, the onset and resolution of pain is very rapid with each episode.
Symptoms and signs reference
1. Mellick LB, Sinex JE, Gibson RW, et al. A systematic review of testicle survival time after a torsion event. Pediatr Emerg Care. 2019;35(12):821-825. doi: 10.1097/PEC.0000000000001287
Diagnosis of Testicular Torsion
History and physical examination
Often color Doppler ultrasound
Torsion must be rapidly identified. Similar symptoms result mainly from epididymitis. With epididymitis, pain and swelling are usually less acute and initially localized to the epididymis. However, in both conditions, generalized swelling and tenderness often develop, making it difficult to distinguish torsion from epididymitis. A clinical diagnosis of torsion is usually sufficient to proceed to treatment.
An equivocal diagnosis may be resolved by immediate imaging if available. Color Doppler ultrasound of the scrotum is preferred. Radioisotope scrotal scanning is also diagnostic but takes longer and therefore is clinically less useful.
Treatment of Testicular Torsion
Manual detorsion
Surgery: Urgently if detorsion is unsuccessful, otherwise electively
Immediate manual detorsion without imaging can be attempted during the initial examination; its success is variable. Because testes usually rotate inward, for detorsion the testis is rotated in an outward direction (eg, for the left testis, detorsion is clockwise when viewed from the front—underneath the testis; a mnemonic is "Stand at the foot and open the book."). More than one rotation may be needed to resolve the torsion; pain relief guides the procedure.
If detorsion fails, immediate surgery is indicated, because exploration within a few hours offers the only hope of testicular salvage. Testicular salvage drops rapidly from 80 to 100% at 6 to 8 hours to near zero at 12 hours. Fixation of the contralateral testis is also done to prevent torsion on that side. When manual detorsion is successful, bilateral testicular fixation is done electively.
Key Points
Testicular torsion typically causes rapid onset of severe scrotal pain, nausea, and vomiting, followed by scrotal edema and induration.
Neither urinary frequency nor fever excludes testicular torsion, but the cremasteric reflex is usually absent.
Treat patients with suggestive clinical findings; reserve imaging studies for cases with equivocal findings.
Rotate the affected testicle outward and, if not successful, arrange for immediate surgery.
More Information
The following English-language resource may be useful. Please note that The Manual is not responsible for the content of this resource.
American Urological Association Curriculum on Acute Scrotum: This case-study offering from the association's medical school curriculum covers the differential diagnosis of acute scrotum with a concentration on 6 conditions: epididymitis, hernia, scrotal trauma, testicular torsion, testicular tumor, and torsion of testicular appendices.





