



Breast symptoms (eg, masses, nipple discharge, pain) are common, accounting for millions of medical visits every year. Although the great majority of symptoms have benign causes, breast cancer is always a concern. Because breast cancer is common and may mimic benign disorders, the approach to all breast symptoms and findings is to exclude conclusively or confirm cancer.
Evaluation
History
History includes the following:
Presence and type of pain
Presence and color of nipple discharge
Relation of symptoms to menses and pregnancy
Presence of skin changes
Use of hormonal contraceptives or menopausal hormone therapy
Date and results of last mammogram or other breast imaging study
Personal or family history of breast cancer
Breast examination
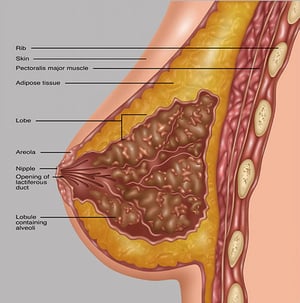
Each breast is inspected for irregularities in shape (bulging, irregular contour), nipple abnormalities (inversion, retraction, discharge, crusting), and skin changes (dimpling, retraction, edema, erythema, scaling, ulceration—see figure for usual positions). A size difference between breasts is common and is not considered an abnormality, unless the patient reports that this is a recent change (because this may be due to breast edema).
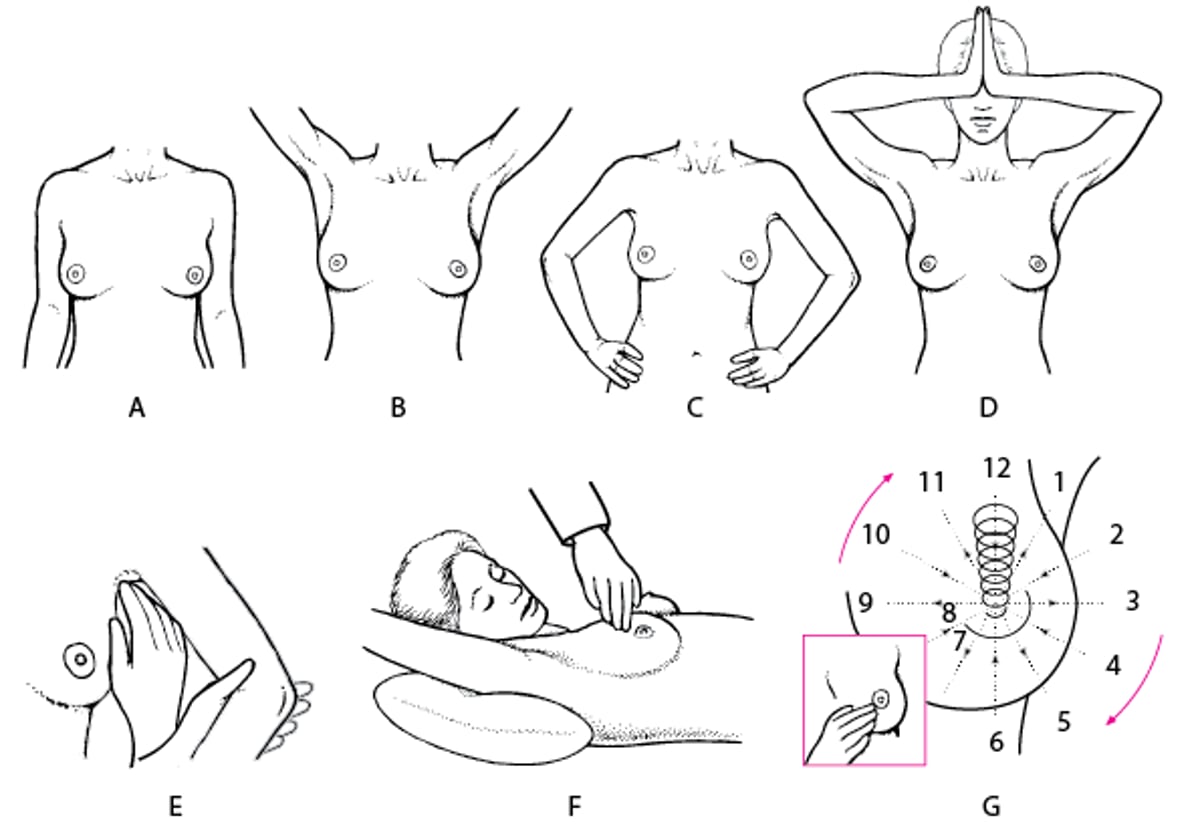
Examining the patient in more than one position may help detect abnormalities. An underlying cancer is sometimes detected by having the patient press both hands against the hips or the palms together in front of the forehead (see figure ). In these positions, the pectoral muscles are contracted, and a subtle dimpling of the skin may appear if a growing tumor has entrapped one of the Cooper ligaments (vertical cutaneous ligaments that attach to the chest wall and support the shape of the breast).


Gwen Shockey/SCIENCE PHOTO LIBRARY

Gwen Shockey/SCIENCE PHOTO LIBRARY

Gwen Shockey/SCIENCE PHOTO LIBRARY
Gwen Shockey/SCIENCE PHOTO LIBRARY
Gwen Shockey/SCIENCE PHOTO LIBRARY
Gwen Shockey/SCIENCE PHOTO LIBRARY
Breast Examination
Positions include the patient seated or standing (A) with arms at sides; (B) with arms raised over the head, elevating the pectoral fascia and breasts; (C) with hands pressed firmly against hips; or (D) with palms pressed together in front of the forehead, contracting the pectoral muscles. (E) Palpation of axilla; arm supported as shown, relaxing the pectoral muscles. (F) Patient supine with pillow under the shoulder and with the arm raised above the head on the side being examined. (G) Palpation of breast in a circular pattern from the nipple outward. |



This photo shows a large, erythematous mass on the upper aspect of the right breast. The mass was later diagnosed as cancer.
DR M.A. ANSARY/SCIENCE PHOTO LIBRARY
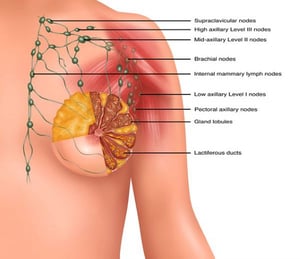
The axillary and supraclavicular lymph nodes are most easily examined with the patient seated or standing (see figure ). Supporting the patient’s arm during the axillary examination allows the arm to be fully relaxed so that nodes deep within the axilla can be palpated.
The breast is palpated with the patient seated and again with the patient supine, the ipsilateral arm above the head, and a pillow under the ipsilateral shoulder (see figure ). Having the patient roll to one side, so that the breast on the examined side falls medially, may help differentiate breast and chest wall tenderness because the chest wall can be palpated separately from breast tissue.


This photo shows a close-up of a retracted or inverted nipple of the breast in an adult female patient. This condition may be a clue to breast cancer, or it may not be due to any underlying disease.
SCIENCE PHOTO LIBRARY
The breast should be palpated with the palmar surfaces of the second, third, and fourth fingers, moving systematically in a small circular pattern from the nipple to the outer edges (see figure ). Precise location and size (estimated or measured with a caliper or measuring tape) of any abnormality should be noted; some clinicians use a paper or digital drawing of the breast for documentation. A written description of the consistency and mobility of the abnormality and degree to which it can be distinguished from surrounding breast tissue should also be included.
Clinicians apply pressure, moving clockwise, to the areola to check for a discharge and, if a discharge is elicited, to determine its source (eg, whether it is multiductal). If discharge is present, it is examined to determine whether it is bloody or blood-tinged. A bright light and magnifying lens can help determine whether nipple discharge is uniductal or multiductal.
Red flags
The following findings are of particular concern:
A mass or thickening that feels distinctly different from other breast tissue
A mass that is fixed to the skin or chest wall
A persistent mass
Changes in the shape of a breast or persistent breast swelling
Peau d'orange (pitting, puckering, reddening, thickening, or dimpling in the skin of the breast)
Scaly skin around the nipple
Changes in the nipple (eg, retraction)
A unilateral nipple discharge, especially if it is bloody and/or occurs spontaneously
Testing
Imaging tests are used for
Screening: Testing of asymptomatic women to detect early cancer
Diagnosis: Evaluation of breast abnormalities (eg, masses, nipple discharge)
Women should be screened for breast cancer (1). All professional societies and groups agree on this concept, although they differ on the recommended age at which to start screening and the frequency of screening.
Screening mammography recommendations for average-risk women vary, but generally, screening starts between ages 40 and 50 and is repeated every year or two until age 75 or until life expectancy is < 10 years (see table ). Screening for breast cancer is discussed in detail separately.
Recommendations for Breast Cancer Screening Mammography in Women With Average Risk
USPSTF | ACS | ACP | ACOG | ACR | NCCN |
|---|---|---|---|---|---|
— | 40-44 | 40-49 | — | — | — |
40 | 45 | 50 | 40 | 40 | 40 |
2 | 45-54: Annually until age 54 ≥ 55: 1-2 years | 2 | 1-2 | 1 | 1 |
75 | Life expectancy < 10 years | 75* | 75* | Limited life expectancy | 75* |
* Women age > 75: Screening may be done based on shared decision-making taking into consideration health status and life expectancy. | |||||
ACOG = American College of Obstetricians and Gynecologists; ACP = American College of Physicians; ACR = American College of Radiology; ACS = American Cancer Society; NCCN = National Comprehensive Cancer Network; USPSTF = US Preventive Services Task Force. | |||||
In mammography, low-dose x-rays of both breasts are taken in 1 (oblique) or 2 views (oblique and craniocaudal).
Breast tomosynthesis (3-dimensional mammography), used for both screening and diagnosis, is done with digital mammography, increases the rate of cancer detection slightly, and decreases the rate of recall imaging; this test is helpful for women with dense breast tissue. However, the test exposes women to almost twice as much radiation as traditional mammography.
Diagnostic mammography is used to do the following:
Evaluate masses, pain, and nipple discharge
Determine size and location of a lesion and provide images of surrounding tissues and lymph nodes
Guide biopsy
After surgery, image the breast to check for recurrence
Diagnostic mammography requires more views than screening mammography. Views include magnified views and spot compression views, which provide better visualization of suspect areas.
Ultrasonography can be used to do the following:
Provide initial imaging of breast abnormalities detected in women < 30 years old
Identify abnormal axillary nodes that may require core biopsy
Evaluate abnormalities detected by MRI or mammography (eg, determine whether they are solid or cystic)
Guide biopsy needle into abnormal breast tissue
MRI can be used to do the following:
Evaluate abnormal findings on breast examination or other imaging studies
Before surgery, accurately determine tumor size, chest wall involvement, and number of tumors, especially in women with dense breast tissue
Identify abnormal axillary lymph nodes (to help stage breast cancer)
Evaluation reference
1. The American College of Obstetricians and Gynecologists: Practice bulletin no. 179: Breast cancer screening. Obstet Gynecol 130 (1), 241–243, 2017. doi: 10.1097/AOG.0000000000002151





