



Tetanus is acute poisoning resulting from a neurotoxin produced by Clostridium tetani. Symptoms are intermittent tonic spasms of voluntary muscles. Spasm of the masseters accounts for the name lockjaw. Diagnosis is clinical. Treatment is with human tetanus immune globulin and intensive support.
(See also Overview of Anaerobic Bacteria and Overview of Clostridial Infections.)
Tetanus bacilli form durable spores that occur in soil and animal feces and remain viable for years.
According to a global study, more than 73,000 total tetanus cases occurred in 2019. Among those cases, 27,000 were in newborns (1). Worldwide in 2019, tetanus was estimated to have caused 34,700 deaths, mostly in South Asia and Sub-Saharan Africa (2), but the disease is so rarely reported that this figure is only a rough estimate. According to the World Health Organization, in 2018 about 25,000 newborns died of neonatal tetanus, which was a 97% reduction since 1988 (3). This reduction was attributed to increased infant immunization, which reached 84% worldwide in 2023.
In the United States since 1947, reported tetanus cases have declined more than 95%, and deaths resulting from tetanus have declined more than 99% (4). Sporadic cases of tetanus continue to occur. Since 2010, fewer than 40 cases have been reported each year (5).
Disease incidence is directly related to the immunization level in a population, attesting to the effectiveness of preventive efforts. In the United States, immunity levels tend to be lower in older age groups.
Patients with burns, frostbite, gangrene, crush injuries, surgical wounds, or a history of injection drug use or exposure to contaminated needles (nonsterile tattoo or body piercing) are especially prone to developing tetanus. However, tetanus may develop in trivial or even inapparent wounds. Infection may also develop postpartum in the uterus (maternal tetanus) and in a neonate's umbilicus (tetanus neonatorum) as a result of unsanitary delivery and umbilical cord care practices. Diabetes and a history of immunosuppression may be risk factors for tetanus.
General references
1. GBD 2019 Diseases and Injuries Collaborators. Global burden of 369 diseases and injuries in 204 countries and territories, 1990-2019: a systematic analysis for the Global Burden of Disease Study 2019. Lancet. 2020;396(10258):1204-1222. doi:10.1016/S0140-6736(20)30925-9
2. Centers for Disease Control and Prevention (CDC). Why CDC is Working to Prevent Tetanus Globally. 2024.
3. World Health Organization (WHO). Tetanus. 2024.
4. CDC. Tetanus Surveillance and Trends. June 10, 2025.
5. Yen LM, Thwaites CL. Tetanus. Lancet. 2019;393(10181):1657-1668. doi:10.1016/S0140-6736(18)33131-3
Pathophysiology of Tetanus
C. tetani spores usually enter through contaminated wounds. Manifestations of tetanus are caused by an exotoxin (tetanospasmin) produced when bacteria lyse. The toxin enters peripheral nerve endings, binds there irreversibly, then travels retrograde along the axons and synapses, and ultimately enters the central nervous system (CNS). As a result, release of inhibitory transmitters from nerve terminals is blocked, causing unopposed muscle stimulation by acetylcholine and generalized tonic spasticity, usually with superimposed intermittent tonic seizures. Disinhibition of autonomic neurons and loss of control of adrenal catecholamine release cause autonomic instability and a hypersympathetic state. Once bound, the toxin cannot be neutralized.
Most often, tetanus is generalized, affecting skeletal muscles throughout the body. However, tetanus is sometimes localized to muscles near an entry wound.
Pearls & Pitfalls
|
Symptoms and Signs of Tetanus
The incubation period ranges from 2 to 50 days (average, 5 to 10 days).
Symptoms of tetanus include:
Jaw stiffness (most frequent)
Dysphagia
Restlessness
Irritability
Stiff neck, arms, or legs
Opisthotonos
Headache
Sore throat
Tonic spasms
Later, patients have trismus.
Spasms
Facial muscle spasm produces a characteristic expression with a fixed smile and elevated eyebrows (risus sardonicus). Rigidity or spasm of abdominal, neck, and back muscles and sometimes opisthotonos (generalized rigidity of the body with arching of the back and neck) may occur. Sphincter spasm causes urinary retention or constipation. Dysphagia may interfere with nutrition.
Characteristic painful, generalized tonic spasms with profuse sweating are precipitated by minor disturbances such as a draft, noise, or movement. Mental status is usually clear, but coma may follow repeated spasms. During generalized spasms, patients are unable to speak or cry out because of chest wall rigidity or glottal spasm. Rarely, fractures result from sustained spasms.
Spasms also interfere with respiration, causing cyanosis or fatal asphyxia.
Autonomic instability
Temperature is only moderately elevated unless a complicating infection, such as pneumonia, is present. Respiratory and pulse rates are increased. Reflexes are often exaggerated. Protracted tetanus may manifest as a very labile and overactive sympathetic nervous system, including periods of hypertension, tachycardia, and myocardial irritability.
Causes of death
Respiratory failure is the most common cause of death. Laryngeal spasm and rigidity and spasms of the abdominal wall, diaphragm, and chest wall muscles cause asphyxiation. Hypoxemia can also induce cardiac arrest, and pharyngeal spasm leads to aspiration of oral secretions with subsequent pneumonia, contributing to a hypoxemic death. Pulmonary embolism is also possible. However, the immediate cause of death may not be apparent.
Localized tetanus
In localized tetanus, there is spasticity of muscles near the entry wound but no trismus; spasticity may persist for weeks.
Cephalic tetanus is a form of localized tetanus that affects the cranial nerves. It is more common among children and may occur with chronic otitis media or after a head wound. Incidence is highest in Africa and India. All cranial nerves can be involved, especially the seventh. Cephalic tetanus may become generalized.
Tetanus neonatorum (neonatal tetanus)
Tetanus in neonates is usually generalized and frequently fatal. It often begins in an inadequately cleansed umbilical stump in children born of inadequately immunized mothers.
Onset during the first 2 weeks of life is characterized by rigidity, spasms, and poor feeding. Bilateral deafness may occur in surviving children.

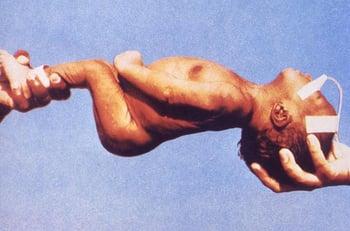
This photo shows generalized rigidity and spasm caused by tetanus in an infant in the first 2 weeks of life.
Diagnosis of Tetanus
History and physical examination
Tetanus should be considered when patients have sudden, unexplained muscle stiffness or spasms, particularly if they have a history of a recent wound or risk factors for tetanus.
Tetanus can be confused with meningoencephalitis of bacterial or viral origin, but the following combination suggests tetanus:
An intact sensorium
Normal cerebrospinal fluid
Muscle spasms
Trismus must be distinguished from peritonsillar or retropharyngeal abscess or another local cause. Phenothiazines can induce tetanus-like rigidity (eg, dystonic reaction, neuroleptic malignant syndrome).
C. tetani can sometimes be cultured from the wound, but culture is not sensitive; only 30% of patients with tetanus have positive cultures. Also, false-positive cultures can occur.
Treatment of Tetanus
Supportive care, particularly respiratory support
Wound debridement
Tetanus antitoxin
Benzodiazepines for muscle spasms
Antibiotics
Sometimes medications for autonomic dysfunction
Treatment of tetanus requires maintaining adequate ventilation.
Additional interventions include early and adequate use of human tetanus immune globulin (TIG) to neutralize nonfixed toxin; prevention of further toxin production; sedation; control of muscle spasm, hypertonicity, fluid balance, and intercurrent infection; and continuous nursing care.
IV immune globulin (IVIG), which contains tetanus antitoxin, may be used if TIG is not available (1, 2).
General principles
The patient should be kept in a quiet room.
Several principles should guide all therapeutic interventions:
Prevent further toxin release by debriding the wound and giving an antibiotic.
Neutralize unbound toxin outside the CNS with TIG.
Immunize using tetanus toxoid, taking care to inject it into a different body site than the antitoxin.
Minimize the effect of toxin already in the CNS.
Wound care
Because dirt and dead tissue promote C. tetani growth, prompt, thorough debridement, especially of deep puncture wounds, is essential.
Antimicrobial therapy (eg, with metronidazole) is not a substitute for adequate debridement and immunization but typically is given.
Antitoxin and toxoid
The benefit of human-derived antitoxin depends on how much tetanospasmin is already bound to the synaptic membranes—only free toxin is neutralized. For adults, TIG 500 units IM once appears as effective as higher doses ranging from 3000 to 6000 units and causes less discomfort. Some medical experts recommend infiltration of part of the dose locally around the wound, but its efficacy has not been proved.
Antitoxin of animal origin is far less preferable because it does not maintain the patient’s serum antitoxin level well and risk of serum sickness is considerable. If horse serum must be used, the usual dose is 50,000 units IM or IV. (CAUTION: See Skin testing.)
If necessary, IVIG or antitoxin can be injected directly into the wound, but this injection is not as important as good wound care.
Tetanus infection does not confer immunity, so unless their vaccination history indicates completion of a full primary series, patients should receive a full primary tetanus vaccination series using an age-appropriate preparation (see Prevention of Tetanus). Antitoxin and vaccine should be injected into different body sites to avoid neutralizing the vaccine.
Management of muscle spasms
Medications are used to manage spasms.
Benzodiazepines are the standard of care to control rigidity and spasms. They block reuptake of an endogenous inhibiting neurotransmitter, gamma-aminobutyric acid (GABA), at the GABAA receptor.
Diazepam can help control seizures, counter muscle rigidity, and induce sedation. Dosage varies and requires meticulous titration and close observation.
Diazepam has been used most extensively, but midazolam is water soluble and preferred for prolonged therapy. Midazolam reduces risk of lactic acidosis due to propylene glycol solvent, which is required for diazepam and lorazepam, and reduces risk of long-acting metabolites accumulating and causing coma.
Benzodiazepines may not prevent reflex spasms, and effective respiration may require neuromuscular blockade with vecuronium or other paralytic medications and mechanical ventilation. Pancuronium has been used but may worsen autonomic instability. Vecuronium does not cause adverse cardiovascular effects but is short-acting.
Intrathecal baclofen (a GABAA agonist) is effective in treating reflex spasms but has no clear advantage over benzodiazepines. Coma and respiratory depression requiring ventilatory support are potential adverse effects.
Dantrolene can be given initially by infusion and thereafter for up to 60 days. Hepatotoxicity and expense limit its use.
Management of autonomic dysfunction
Morphine may be given by continuous infusion to control autonomic dysfunction, especially cardiovascular. Severe bradycardia may require pacemaker placement.
Beta-blockade is used to control episodes of hypertension and tachycardia, but use of long-acting medications such as propranolol is not recommended. Sudden cardiac death is a complication of tetanus, and beta-blockade can increase risk. Esmolol, a short-acting beta-blocker, has been used successfully. Blockade of the parasympathetic nervous system with high-dose IV atropine markedly reduces excessive sweating and secretions and manages bradycardia. Use of clonidine, an alpha adrenergic receptor agonist, has been associated with decreased mortality (3).
Magnesium sulfate given by IV continuous infusion at doses that maintain serum levels between 4 to 8 mEq/L has a stabilizing effect, eliminating catecholamine stimulation (4). Patellar tendon reflex is used to assess overdosage. Serum magnesium levels and electrical cardiac activity need to be closely monitored throughout the infusion period.
Tidal volume may be impaired, so ventilatory support must be available.
Other medications that act on the autonomic nervous system and may prove useful include:
Pyridoxine, which lowers mortality in neonates
Valproic acid, which blocks GABA-aminotransferase, inhibiting GABA catabolism
Angiotensin-converting enzyme inhibitors, which inhibit angiotensin II and reduce norepinephrine release from nerve endings
Dexmedetomidine (a potent alpha-2 adrenergic agonist)
Adenosine, which reduces presynaptic norepinephrine release and antagonizes the inotropic effect of catecholamines
Glucocorticoids are of unproven benefit; their use is not recommended.
Antibiotics
The role of antibiotic therapy is minor compared with wound debridement and general support.
Metronidazole is the recommended antibiotic.
Supportive care
In moderate or severe cases, patients should be intubated. Mechanical ventilation is essential when neuromuscular blockade is required to control muscle spasms that impair respirations.
IV hyperalimentation avoids the hazard of aspiration secondary to gastric tube feeding. Because constipation is usual, stools should be kept soft. A rectal tube may control distention. Bladder catheterization is required if urinary retention occurs.
Chest physiotherapy, frequent turning, and forced coughing are essential to prevent pneumonia. Analgesia with opioids is often needed.
Treatment references
1. Rodrigo C, Fernando D, Rajapakse S. Pharmacological management of tetanus: an evidence-based review. Crit Care. 2014;18(2):217. Published 2014 Mar 26. doi:10.1186/cc13797
2. Govindaraj GM, Riyaz A. Current practice in the management of tetanus. Crit Care. 2014;18(3):145. Published 2014 May 27. doi:10.1186/cc13894
3. Gregorakos L, Kerezoudi E, Dimopoulos G, Thomaides T. Management of blood pressure instability in severe tetanus: the use of clonidine. Intensive Care Med. 1997;23(8):893-895. doi:10.1007/s001340050428
4. Thwaites CL, Yen LM, Cordon SM, et al. Effect of magnesium sulphate on urinary catecholamine excretion in severe tetanus. Anaesthesia. 2008;63(7):719–725. doi:10.1111/j.1365-2044.2008.05476.x
Prognosis for Tetanus
The case fatality rate of patients with tetanus varies widely between resource-rich and resource-poor nations. With use of modern supportive care, including mechanical ventilation, most patients recover.
Untreated neonates and adults have a high mortality rate (1).
Mortality is highest at the extremes of age and in injection drug users.
The prognosis is poorer if the incubation period is short and symptoms progress rapidly or if treatment is delayed. The course tends to be milder when there is no demonstrable focus of infection.
Prognosis reference
1. Centers for Disease Control and Prevention (CDC): Why CDC is Working to Prevent Global Tetanus. May 16, 2024. Accessed August 15, 2025.
Prevention of Tetanus
Tetanus is preventable by vaccination. Vaccination is strongly recommended for all infants, children, adolescents, and adults. Tetanus is rare in high-income countries but remains common in low-income countries with suboptimal vaccination initiatives (1).
See Diphtheria-Pertussis-Tetanus Vaccine for more information, including indications, contraindications and precautions, dose and administration, and adverse effects.
See Tetanus-Diphtheria Vaccine for more information, including indications, contraindications and precautions, dose and administration, and adverse effects.
Because tetanus infection does not confer immunity, patients who have recovered from clinical tetanus should be vaccinated unless they have completed a full primary series.
Patients who have a wound that poses an increased risk of tetanus should be given prophylaxis depending on wound type and vaccination history; tetanus immune globulin also may be indicated (see table ).
Tetanus Prophylaxis in Routine Wound Management
History of Adsorbed Tetanus Toxoid | Clean, Minor Wounds | All Other Wounds* | ||
|---|---|---|---|---|
DTaP, Tdap, or Td† | TIG‡ | DTaP, Tdap, or Td† | TIG‡ | |
Unknown or < 3 doses | Yes | No | Yes | Yes |
≥ 3 doses | Yes if ≥ 10 years since last dose | No | Yes if ≥ 5 years since last dose | No |
* Such as (but not limited to) wounds contaminated with dirt, feces, soil, or saliva; penetrating or puncture wounds; crush injuries; compound fractures; avulsions; necrotic or gangrenous wounds; and wounds resulting from burns or frostbite. | ||||
† DTaP is recommended for children < 7 years of age. For patients ≥ 11 years of age who have not previously received a dose of Tdap, a single dose of Tdap should be given. Patients ≥ 7 years of age who are not fully immunized against pertussis, tetanus, or diphtheria should receive one dose of Tdap for wound management and as part of the catch-up series. | ||||
‡ People with HIV infection or severe immunodeficiency who have contaminated wounds should also receive TIG, regardless of their tetanus immunization history. | ||||
DTaP = diphtheria and tetanus toxoids, acellular pertussis (for children); Td = tetanus and diphtheria toxoids adsorbed; Tdap = tetanus and diphtheria toxoids, acellular pertussis; TIG = tetanus immune globulin (human). | ||||
Adapted from Centers for Disease Control and Prevention: Clinical Guidance for Wound Management to Prevent Tetanus. June 10, 2025. Accessed August 15, 2025. | ||||
Prevention reference
1. Yen LM, Thwaites CL. Tetanus. Lancet. 2019;393(10181):1657-1668. doi:10.1016/S0140-6736(18)33131-3
Key Points
Tetanus is caused by a toxin produced by Clostridium tetani in contaminated wounds.
Tetanus toxin blocks release of inhibitory neurotransmitters, causing generalized muscle stiffness with intermittent spasms; seizures and autonomic instability may occur.
Prevent further toxin release by debriding the wound and giving an antibiotic (eg, metronidazole), and neutralize unbound toxin with human tetanus immune globulin.
Give IV benzodiazepines for muscle spasm, and use neuromuscular blockade and mechanical ventilation as needed for respiratory insufficiency due to muscle spasm.
Mortality is high in untreated neonates and adults.
Prevent tetanus by following routine immunization recommendations.
Drug Information for the Topic





