



Leishmaniasis is an infection caused by a species of Leishmania. Manifestations include cutaneous, mucosal, and visceral syndromes. Cutaneous leishmaniasis causes chronic skin lesions ranging from nodules to large ulcers that can persist for months to years but eventually heal with scarring. Mucosal leishmaniasis affects nasopharyngeal tissues and can cause gross mutilation of the nose and palate. Visceral leishmaniasis causes irregular fever, hepatosplenomegaly, pancytopenia, and polyclonal hypergammaglobulinemia with high mortality in untreated patients. Diagnosis is by demonstrating parasites in smears or cultures and increasingly by polymerase chain reaction–based assays at reference centers. Serologic testing can be helpful in diagnosing visceral leishmaniasis. Oral miltefosine is used to treat all 3 syndromes. Treatment of mucosal leishmaniasis is with liposomal amphotericin B and pentavalent antimonials; azoles may be used depending on the Leishmania species, and reconstructive surgery may be necessary in severe cases. Treatment of visceral leishmaniasis is with liposomal amphotericin B depending on the infecting Leishmania species and the geographic area of acquisition. A variety of topical and systemic treatments is available for cutaneous leishmaniasis depending on the causative species and clinical manifestations. Alternatives include oral azoles, amphotericin B deoxycholate, or pentavalent antimonials (sodium stibogluconate or meglumine antimoniate) if disease was acquired in areas where Leishmania species are likely to be susceptible.
Leishmaniasis in humans is caused by approximately 21 of the 30 Leishmania species that are morphologically indistinguishable but can be differentiated by laboratory analysis (1).
Leishmaniasis is not a rare disease. Incidence is estimated to be between 700,000 to 1 million new cases annually worldwide. Poor housing and inadequate domestic sanitation, malnutrition, and migration or population displacement of nonimmune hosts to endemic areas are key risk factors for the development of infection (2).
Leishmania promastigotes are transmitted to vertebrate hosts by sandflies (Phlebotomus [Old World], Lutzomyia [New World]). Vector sandflies are infected by inoculating infected humans or animals. Rarely, infection can be spread congenitally or sexually or by blood transfusion or shared needles (and needle-stick injuries).
Animal reservoirs vary with the Leishmania species and geographic location and include dogs, other canines, rodents, and other animals (see also Sand Flies of Animals). In the Indian subcontinent, humans are the reservoir for L. donovani.
General references
1. CDC: Leishmaniasis. Accessed March 24, 2025.
2. World Health Organization (WHO): Leishmaniasis. Accessed February 12, 2025.
Pathophysiology of Leishmaniasis
The first step in the life cycle is infection of a human host after inoculation by a female sandfly; extracellular promastigotes are injected into the bloodstream and phagocytized by host macrophages. Inside these cells, they transform into amastigotes.

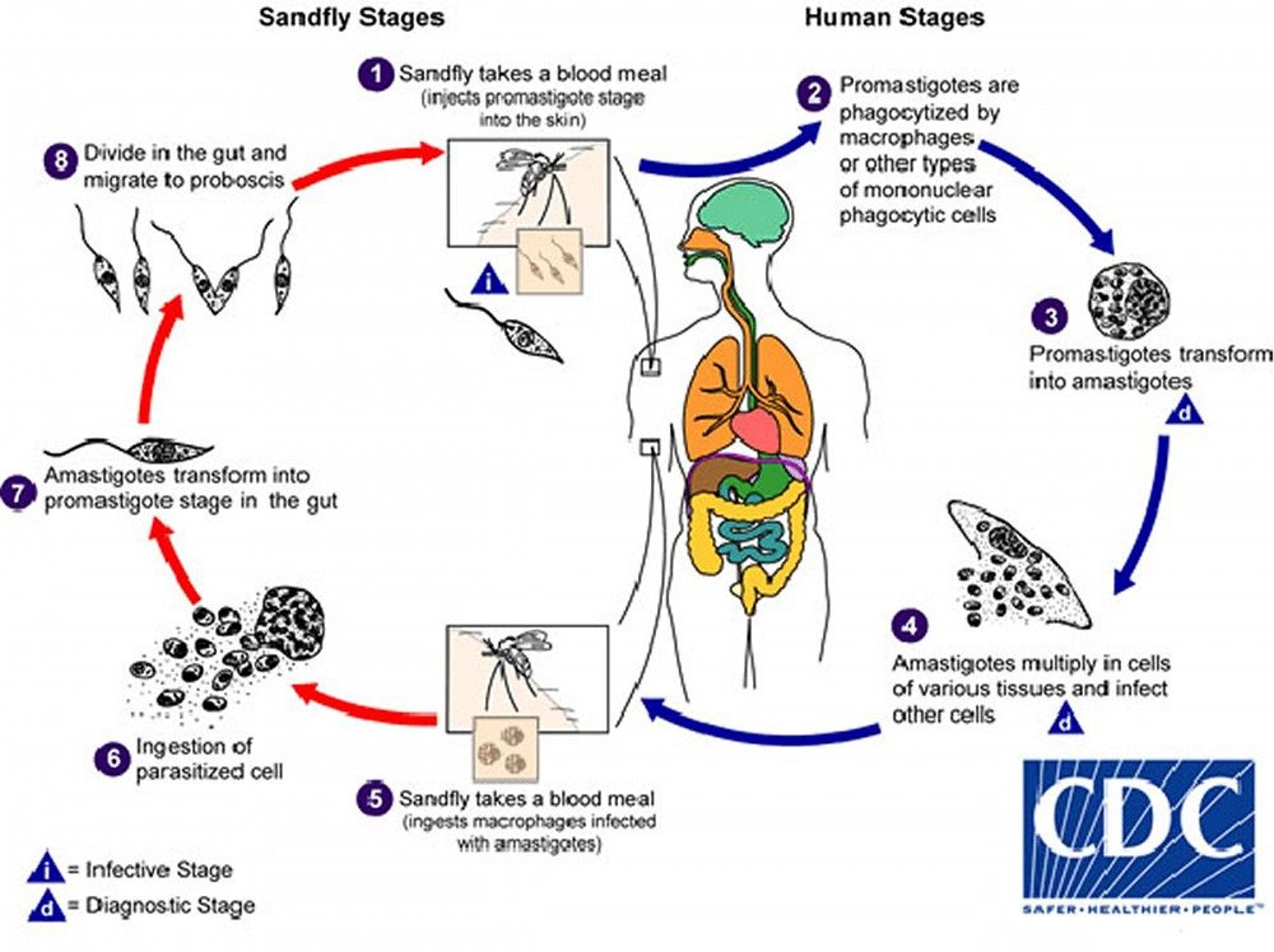
1. Leishmaniasis is transmitted by the bite of infected female phlebotomine sandflies. During a blood meal, the sandflies inject metacyclic promastigotes (the infective stage) from their proboscis.
2. Promastigotes are phagocytized by macrophages and other mononuclear phagocytic cells.
3. In these cells, promastigotes transform into amastigotes (the tissue stage).
4. Amastigotes multiply by simple division and infect other mononuclear phagocytic cells.
5–6. During a blood meal on an infected host, sandflies become infected by ingesting macrophages infected with amastigotes.
7. In the midgut of the sandflies, amastigotes transform into promastigotes.
8. There, they multiply, develop, and migrate to the proboscis.
Image from the Centers for Disease Control and Prevention, Global Health, Division of Parasitic Diseases and Malaria.
The amastigotes may remain localized in the skin or spread to the mucosa of the nasopharynx or disseminate to bone marrow, the spleen, the liver, and occasionally other organs, resulting in 3 major clinical forms of leishmaniasis:
Cutaneous
Mucosal
Visceral
Cutaneous leishmaniasis
Cutaneous leishmaniasis is the most commonly diagnosed form of leishmaniasis. It is also known as oriental or tropical sore, Delhi or Aleppo boil, uta or chiclero ulcer, or forest yaws. The major causative species are the following:
L. major, L. aethiopica, and L. tropica in southern Europe, Asia, and Africa
L. mexicana complex (L. mexicana, L. amazonensis, and L. venezuelensis) in Mexico and Central and South America
Viannia subgenus (L. braziliensis, L. guyanensis, L. panamensis, and L. peruviana) in Central and South America
Cases have occurred among United States military personnel serving in Iraq and Afghanistan and among travelers to endemic areas in Central and South America, Israel, and elsewhere. Uncommonly, L. braziliensis spreads widely in the skin causing disseminated cutaneous leishmaniasis.
L. donovani typically causes visceral leishmaniasis in the Indian subcontinent, but it also causes cutaneous leishmaniasis in Sri Lanka.
Rarely, L. infantum can cause cutaneous leishmaniasis in the Western hemisphere.
Mucosal leishmaniasis
Mucosal leishmaniasis (mucocutaneous leishmaniasis, espundia) is caused mainly by Viannia subgenus but occasionally by other Leishmania species. Mucosal leishmaniasis is most commonly found south and west of the Amazon basin, specifically in parts of Bolivia, Peru, and Brazil.
The parasites are thought to spread from the initial skin lesion through the lymphatics and blood to nasopharyngeal tissues.
Symptoms and signs of mucosal leishmaniasis typically develop months to years after the appearance of the skin lesion.
Visceral leishmaniasis
Visceral leishmaniasis (kala-azar, Dumdum fever) is typically caused by L. donovani or L. infantum (also called L. chagasi in Latin America) and occurs in India, Africa (particularly the Sudan), Central Asia, the Mediterranean basin, South and Central America, and infrequently China. Most cases occur in northeastern India.
Parasites disseminate from the site of the sandfly bite in the skin to regional lymph nodes, the spleen, the liver, and bone marrow and cause systemic symptoms.
Subclinical infections are common; only a minority of infected patients develop progressive visceral disease. Symptomatic infection with L. infantum is more common among children than adults.
Visceral leishmaniasis is an opportunistic infection in patients with advanced HIV infection or other immunocompromising conditions.
Symptoms and Signs of Leishmaniasis
In cutaneous leishmaniasis, a well-demarcated skin lesion develops at the site of a sandfly bite, usually within several weeks to months. Multiple lesions may occur after multiple infective bites or with disseminated spread. Their appearance varies. The initial lesion is often a papule or nodular plaque that slowly enlarges, ulcerates centrally, and develops a raised, erythematous border where intracellular parasites are concentrated. Ulcers are typically painless and cause no systemic symptoms unless secondarily infected. Lesions heal spontaneously after several months but may persist for years. They often cause atrophic scarring, leaving a depressed, burn-like scar.
Lymphadenopathy or lymphangitis may occur.
Disease course depends on the infecting Leishmania species and the host’s immune status.


The classic lesion of cutaneous leishmaniasis is a well-demarcated skin lesion with central ulceration and a raised and erythematous border.
© Springer Science+Business Media
Diffuse cutaneous leishmaniasis, a rare syndrome, results in widespread nodular skin lesions resembling those of lepromatous leprosy. It results from cell-mediated anergy (lack of immune responsiveness in the host) to the organism.
Mucosal leishmaniasis, also called mucocutaneous leishmaniasis, due to Viannia subgenus species typically starts with one or more primary cutaneous ulcers. Spread to the mucosa via lymphatics and the bloodstream probably occurs early in infection.
The skin lesions heal spontaneously, but progressive mucosal lesions may not become apparent for months to years. Typically, patients have nasal stuffiness, epistaxis, discharge, and pain. Over time, the infection may progress, resulting in gross mutilation of the nose, palate, oral pharynx, or face.


This photo shows a patient with mucosal leishmaniasis with significant erythema and nodularity of the nasal passage and accompanying erosion of the nasal septum.
Image courtesy of Dr. A. Canese via the Public Health Image Library of the Centers for Disease Control and Prevention.
In visceral leishmaniasis, the clinical manifestations usually develop gradually over weeks to months after inoculation of the parasite but can be acute. Irregular fever, hepatosplenomegaly, pancytopenia, and polyclonal hypergammaglobulinemia with a reversed albumin:globulin ratio occur. In some patients, there are twice-daily temperature spikes. Transaminitis may occur. Cutaneous skin lesions rarely occur. Some patients may present with fever, anorexia, diarrhea, and malaise.
Emaciation and death occur within months to years in patients with progressive infections. Those with asymptomatic, self-resolving infections and survivors (after successful treatment) are resistant to further attacks unless cell-mediated immunity is impaired (eg, by advanced HIV infection). Relapse may occur years after initial infection.


This photo shows a young boy with visceral leishmaniasis (kala-azar) exhibiting clinical features of hepatosplenomegaly and muscle wasting.
A. CRUMP, TDR, WHO/SCIENCE PHOTO LIBRARY
Post kala-azar dermal leishmaniasis (PKDL) may develop after treatment for visceral leishmaniasis in patients in eastern Africa (Sudan, Ethiopia, Kenya) and in India, Nepal, and Bangladesh (1). It is characterized by flat or nodular cutaneous lesions that contain many parasites.
In patients in eastern Africa, lesions develop within 3 to 6 months of therapy and spontaneously resolve a few months to a year later. In patients in India and adjacent countries, skin lesions typically develop 2 to 7 years after therapy ends and can last for many years. PKDL lesions are thought to be a reservoir for the spread of infection in these areas.


This photo depicts diffuse nodular infiltrates on the face of a man with post kala-azar dermal leishmaniasis (PKDL); lesions are especially prominent on the nose.
ANDY CRUMP / SCIENCE PHOTO LIBRARY
Symptoms and signs references
1. Kumar P, Chatterjee M, Das NK. Post Kala-Azar Dermal Leishmaniasis: Clinical Features and Differential Diagnosis. Indian J Dermatol. 2021;66(1):24-33. doi:10.4103/ijd.IJD_602_20
Diagnosis of Leishmaniasis
Light microscopy of Wright-Giemsa–stained or Giemsa-stained tissue samples, touch preparations, or aspirates
Laboratory testing, including serologic testing (antibody titers) for visceral leishmaniasis
Culture (special media required)
Polymerase chain reaction (PCR)–based assays
Leishmaniasis should be suspected in any patient with characteristic chronic cutaneous lesions and a history of exposure, ie, travel to or immigration from an endemic area.
Organisms causing simple cutaneous leishmaniasis can be differentiated from those capable of causing mucosal leishmaniasis based on the geographic area of acquisition, specific DNA probes, or analysis of cultured parasites.
Biopsy specimens from lesions can be examined histologically to identify the presence of Leishmania amastigotes and to assess the inflammatory response. Assessment is usually performed via light microscopy of Wright-Giemsa–stained or Giemsa-stained tissue samples (1). Immunohistochemistry of leishmanial antigens may be demonstrable in tissue samples and are helpful adjuncts for diagnosis.
Serologic tests can help diagnose visceral leishmaniasis; high titers of antibodies to a recombinant leishmanial antigen (rk39) are present in most immunocompetent patients with visceral leishmaniasis. However, antibodies may be absent in patients with HIV co-infection or other immunocompromising conditions. Serologic tests for antileishmanial antibodies do not distinguish between active and quiescent infections because they are not sensitive or specific and are not helpful in the diagnosis of cutaneous leishmaniasis (1). Antibody tests are more useful in detecting visceral leishmaniasis. Additionally, pancytopenia, hypergammaglobulinemia with high total protein, and reduced albumin:globulin ratios may be seen in patients with visceral leishmaniasis (1).
PCR-based assays of aspirates from bone marrow, the spleen, or lymph nodes help diagnose visceral leishmaniasis. In cases of cutaneous leishmaniasis, PCR assays can be performed on punch biopsies, aspirates, or touch preparations from skin lesions to aid in diagnosis. In mucosal leishmaniasis, parasites are usually more difficult to find or isolate in culture from biopsies of lesions than in cutaneous leishmaniasis.
The leishmanin skin test that detects a delayed-type hypersensitivity response to leishmanial antigens is not available in the United States. It is typically positive in patients with cutaneous and mucosal leishmaniasis but negative in those with active visceral leishmaniasis.
The Centers for Disease Control and Prevention (CDC) in the United States offers specialized diagnostic services for leishmaniasis. For further information, see the CDC's Infectious Diseases Laboratories: Leishmania species Identification.
Diagnosis reference
1. Aronson N, Herwaldt BL, Libman M, et al: Diagnosis and treatment of leishmaniasis: Clinical Practice Guidelines by the Infectious Diseases Society of America (IDSA) and the American Society of Tropical Medicine and Hygiene (ASTMH). Clin Infect Dis. 2016;63(12):e202-e264. doi:10.1093/cid/ciw670
Treatment of Leishmaniasis
Oral miltefosine for mucosal, visceral, and cutaneous leishmaniasis
Liposomal amphotericin B IV or sometimes parenteral paromomycin and pentamidine for visceral leishmaniasis
Topical paromomycin, heat therapy, cryotherapy, and/or intralesional injection of a pentavalent antimonial (variable availability) for cutaneous leishmaniasis
Oral azoles (eg, ketoconazole, itraconazole) or intralesional, IV, or IM amphotericin B deoxycholate or pentavalent antimonials (sodium stibogluconate, meglumine antimoniate) may have benefit if the infecting Leishmania species is likely to be susceptible
Treatment of leishmaniasis depends on many factors, including the following (1):
Clinical syndrome
Infecting Leishmania species
Geographic location of acquisition
Organism's likelihood of susceptibility to antileishmanial drugs
Age and immune status of the host
Detailed recommendations for treatment are available (2, 3).
Pentavalent antimonials are not readily available in the United States. Meglumine antimoniate is available in the United States only under an individual investigational new drug protocol via the U.S. Food and Drug Administration (FDA). Sodium stibogluconate is no longer available from the Centers for Disease Control and Prevention but may be available in some countries.
Cutaneous leishmaniasis
Cutaneus leishmaniasis is treated with topical formations of paromomycin (especially in Old World cutaneous leishmaniasis), heat therapy, cryotherapy, and/or intralesional injection of a pentavalent antimonial (where available).
If a lesion is small, spontaneously healing, and not caused by a Leishmania species associated with mucosal leishmaniasis, it can be closely followed, rather than treated.
Topical treatment is an option for small, uncomplicated lesions. Intralesional injection of sodium stibogluconate has been used for many years for simple cutaneous leishmaniasis in Europe and Asia; it is not currently available in the United States for intralesional use.
Other topical options include heat therapy, which requires a specialized system for administration, and cryotherapy; both can be painful and are practical only when used to treat small lesions.
Topical paromomycin can be used as an ointment that contains 15% paromomycin and 12% methylbenzethonium chloride in soft white paraffin. This medication is used around the world, but in the United States it may need to be requested through compounding pharmacies.
Systemic therapy is used in patients who have the following:
Infection by L. braziliensis or related organisms associated with mucosal leishmaniasis
Complex cutaneous leishmaniasis with multiple, large, widespread, or disfiguring lesions
Compromised cell-mediated immunity
In the United States, systemic options include liposomal amphotericin B, miltefosine, and amphotericin B deoxycholate. Outside the United States, pentavalent antimonials (sodium stibogluconate and meglumine antimoniate) may be used if infection was acquired in areas where antimony-resistance is not prevalent. Liposomal amphotericin B and amphotericin B deoxycholate are typically given in the regimens used for visceral leishmaniasis.
Although not approved for cutaneous infection, liposomal amphotericin B may have merit in select cases.
Miltefosine, which has the advantage of oral administration, can be effective for cutaneous leishmaniasis in adults and adolescents, particularly when caused by L. braziliensis, L. guyanensis, or L. panamensis (2). Adverse effects include nausea, vomiting, transient elevations in aminotransferases, and dizziness. Miltefosine is contraindicated during pregnancy and breastfeeding (chestfeeding); patients of childbearing age who are taking this drug must use effective birth control measures.
Pentavalent antimonials should be used only if the infecting Leishmania species is likely to be susceptible. Meglumine antimoniate is used in French-speaking countries and in Latin America. Adverse effects include nausea, vomiting, malaise, elevated amylase and/or liver enzymes, and cardiotoxicity (arrhythmias, myocardial depression, heart failure, ECG changes, cardiac arrest). The incidence of adverse effects increases with age. The drug is stopped if patients develop cardiotoxicity.
Alternatives include azoles (eg, ketoconazole, itraconazole, fluconazole) if the infecting Leishmania species is likely to be susceptible. Azoles have limited effectiveness, but success has been reported with higher daily doses in some areas (4).
Diffuse cutaneous leishmaniasis is relatively resistant to treatment.
Mucosal leishmaniasis
The optimal treatment is uncertain.
Studies suggest that both liposomal amphotericin B and oral miltefosine are often effective, but data are limited. Miltefosine can be used in adults and adolescents (2). Adverse effects of miltefosine include nausea, vomiting, transient elevations in aminotransferases, and dizziness; the drug is contraindicated during pregnancy and breastfeeding (chestfeeding); patients of childbearing age who are taking this drug must use effective birth control measures.
Although not approved for mucosal infection, liposomal amphotericin B may have merit in select cases.
Historically, pentavalent antimonials have been used in Latin America.
Intralesional, IV, or IM amphotericin B deoxycholate, which is highly effective but generally more toxic than liposomal amphotericin B, is an alternative if the infecting Leishmania species is likely to be susceptible.
Other alternatives include azoles (eg, ketoconazole, itraconazole, fluconazole) if the infecting Leishmania species is likely to be susceptible. Azoles have limited effectiveness, but success has been reported with higher daily doses in some areas (4).
Reconstructive surgery may be required if mucosal leishmaniasis grossly distorts the nose or palate, but surgery should be delayed for 12 months after successful chemotherapy to avoid losing grafts because of relapses.
Visceral leishmaniasis
Liposomal amphotericin B and miltefosine can be used to treat visceral leishmaniasis; other lipid-associated amphotericin preparations may be effective but have been less well studied.
Oral miltefosine can be used to treat immunocompetent patients who acquired L. donovani in India or adjacent areas of South Asia, who are > 12 years of age, who weigh > 30 kg, and who are not pregnant or breastfeeding (2).
Pentavalent antimonials can be used to treat visceral leishmaniasis acquired in Latin America or other areas of the world where the infection is not resistant to these drugs (most notably South Asia where resistance is high). Parenteral paromomycin and pentamidine have been used for this purpose.
Intralesional, IV, or IM amphotericin B deoxycholate, which is highly effective but generally more toxic than liposomal amphotericin B, is an alternative if the infecting Leishmania species is likely to be susceptible.
Relapses are common among patients with immunocompromising conditions. Antiretroviral drugs can help restore immune function in patients infected with HIV, reducing the likelihood of relapse. Secondary prophylaxis with an antileishmanial drug may help prevent relapses in patients with advanced HIV infection with CD4 counts < 200/mcL.
Supportive measures (eg, adequate nutrition, transfusions, antibiotics for secondary bacterial infection) are often necessary for patients with visceral leishmaniasis.
Treatment references
1. Pan American Health Organization. Guideline for the treatment of leishmaniasis in the Americas. Second edition. Washington, DC: PAHO; 2022. doi:10.37774/9789275125038
2. Aronson N, Herwaldt BL, Libman M, et al. Diagnosis and treatment of leishmaniasis: Clinical Practice Guidelines by the Infectious Diseases Society of America (IDSA) and the American Society of Tropical Medicine and Hygiene (ASTMH). Clin Infect Dis. 2016;63(12):e202-e264. doi:10.1093/cid/ciw670
3. Centers for Disease Control and Prevention (CDC). Clinical Care of Leishmaniasis. Accessed February 11, 2025.
4. Galvão EL, Rabello A, Cota GF. Efficacy of azole therapy for tegumentary leishmaniasis: A systematic review and meta-analysis. PLoS One. 2017;12(10):e0186117. Published 2017 Oct 9. doi:10.1371/journal.pone.0186117
Prevention of Leishmaniasis
For prevention of leishmaniasis, the following may help:
Treatment of leishmaniasis in a geographic area where humans are the reservoir
Reduction of the vector population by spraying residual insecticide (one that has prolonged duration of action) in sites of domestic transmission
Personal protective measures including insect repellants on exposed skin and protective clothing
Control of nonhuman reservoirs
Avoidance of sharing needles and taking precautions against needle-stick injuries
Safe blood transfusions
Education about the risks of congenital and sexual transmission
Travelers to endemic areas should use insect repellents containing DEET (diethyltoluamide) on exposed skin. Insect screens, bed nets, and clothing are more effective if treated with permethrin because the small sandflies can penetrate mechanical barriers.
Pregnant patients in endemic regions should avoid sandflies, seek early diagnosis, be given prompt, pregnancy-appropriate therapy (liposomal amphotericin B).
Vaccines are not currently available; however, several vaccine trials are underway (1).
Prevention reference
1. Mas A, Hurtado-Morillas C, Martínez-Rodrigo A, et al. A Tailored Approach to Leishmaniases Vaccination: Comparative Evaluation of the Efficacy and Cross-Protection Capacity of DNA vs. Peptide-Based Vaccines in a Murine Model. Int J Mol Sci. 2023;24(15):12334. Published 2023 Aug 2. doi:10.3390/ijms241512334
Key Points
Leishmaniasis is present globally and is transmitted by of sandfly bites.
The parasites may remain localized in the skin (cutaneous leishmaniasis), spread to the mucosa (mucosal leishmaniasis), or disseminate systemically to the liver, spleen, and bone marrow (visceral leishmaniasis).
Diagnose using Wright-Giemsa– or Giemsa-stained smears, cultures, or polymerase chain reaction-based assays; serologic tests can help diagnose visceral leishmaniasis.
Treat small, uncomplicated skin lesions with locally applied heat or cryotherapy, topical paromomycin, or outside the United States with intralesional sodium stibogluconate.
Systemic treatment options for complex cutaneous leishmaniasis, mucosal leishmaniasis, and visceral leishmaniasis include liposomal amphotericin B, miltefosine, and amphotericin B deoxycholate; pentavalent antimonials may be used if infection is acquired in areas where the infecting Leishmania species is likely to be susceptible.
Drug resistance to pentavalent antimonials is common in South Asia and adjacent countries and is emerging in other areas.
More Information
The following English-language resource may be useful. Please note that The Manual is not responsible for the content of this resource.
Centers for Disease Control and Prevention (CDC): Clinical Testing and Diagnosis for Leishmaniasis
Drug Information for the Topic





