



Herpes zoster is infection that results when varicella-zoster virus reactivates from its latent state in a posterior dorsal root ganglion. Symptoms usually begin with pain along the affected dermatome, followed within 2 to 3 days by a vesicular eruption that is usually diagnostic. Treatment is with antiviral medications, ideally given within 72 hours after skin lesions appear.
(See Overview of Herpesvirus Infections.)
Chickenpox and herpes zoster are caused by the varicella-zoster virus (human herpesvirus type 3); chickenpox is the acute, primary infection phase of the virus, and herpes zoster (shingles) represents reactivation of virus from the latent phase after (usually) long periods of dormancy in the nerve ganglia. People above the age of 50 who have had chickenpox in childhood are at increased risk of herpes zoster.
Herpes zoster is not an uncommon disease. In 1 systematic review, the global cumulative incidence of herpes zoster ranged from 2.9 to 19.5 cases per 1000 people (1). Incidence is broadly similar in the United States, at a rate of approximately 2 to 9 cases per 1000 people annually (2). There is a lifetime risk of 32% for developing the disease, but this risk is increased to as high as 50% in adults by age 85; the incidence rises sharply with age (3).
Herpes zoster inflames the sensory root ganglia, the skin of the associated dermatome, and sometimes the posterior and anterior horns of the gray matter, meninges, and dorsal and ventral roots. Herpes zoster frequently occurs in adults over 50 and people living with HIV and is more frequent and severe in patients who are immunocompromised due to defects in cell-mediated immunity.
Other factors have been purported to be associated with an increased risk of herpes zoster. One meta-analysis of 62 studies found that the risk is increased in women, people with autoimmune diseases (eg, rheumatoid arthritis, systemic lupus erythematosus) likely related to use of immunosuppressive agents in these patients, those with certain comorbidities (eg, asthma, diabetes, and COPD), and those with recent physical trauma, while Black people were found to have a reduced risk of contracting herpes zoster compared to white people (4).
General references
1. van Oorschot D, Vroling H, Bunge E, Diaz-Decaro J, Curran D, Yawn B. A systematic literature review of herpes zoster incidence worldwide. Hum Vaccin Immunother. 2021;17(6):1714-1732. doi:10.1080/21645515.2020.1847582
2. Centers for Disease Control and Prevention. Clinical Overview of Shingles (Herpes Zoster). June 27, 2024. Accessed October 18, 2025.
3. Leung J, Harrington T, Dooling K. Zoster. Centers for Disease Control and Prevention. Centers for Disease Control and Prevention. May 9, 2024. Accessed October 18, 2025.
4. Kawai K, Yawn BP. Risk Factors for Herpes Zoster: A Systematic Review and Meta-analysis. Mayo Clin Proc. 2017;92(12):1806-1821. doi:10.1016/j.mayocp.2017.10.009
Symptoms and Signs of Herpes Zoster
Lancinating, dysesthetic, or other pain develops in the involved site, typically followed within 2 to 3 days by a rash, usually crops of vesicles on an erythematous base (1). Affected sites usually encompass 1 or more adjacent dermatomes in the thoracic or lumbar region, although a few satellite lesions may also appear. Lesions are typically unilateral and do not cross the midline of the body. Affected areas are usually hyperesthetic often with a burning or throbbing sensation, and pain (from neuronal activation) may be severe. Lesions usually continue to form for about 3 to 5 days.

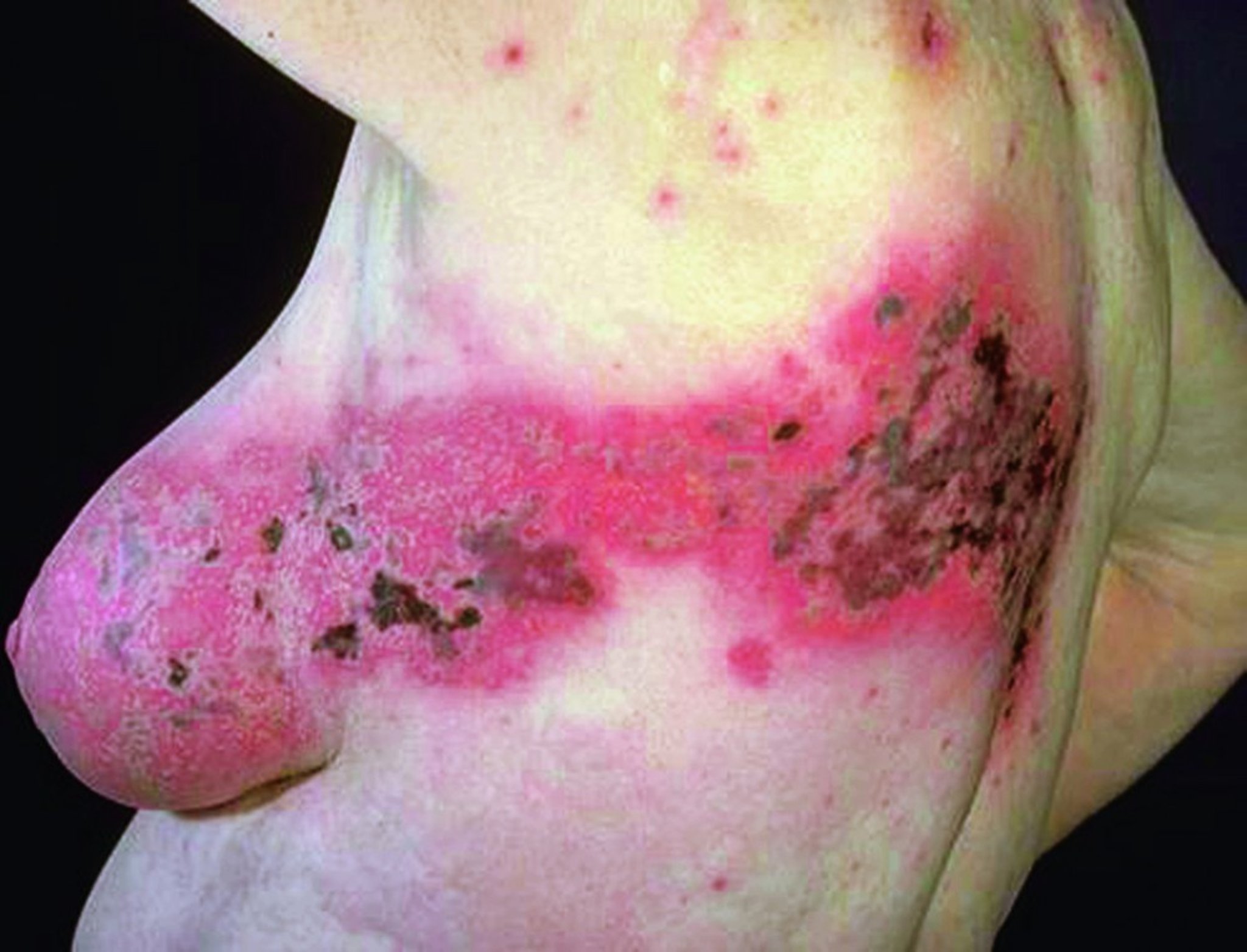
The cutaneous viral infection follows neural dermatomes and is accompanied by burning, erythema, blistering, and necrosis.
© Springer Science+Business Media


Image depicts cutaneous thoracic herpes zoster of the right dorsal region of an affected individual, with rash comprised of vesicular eruptions (blisters).
Photo courtesy of Karen McKoy, MD.


This photo shows the dermatomal band of erythema with superimposed grouped and scattered vesicles due to herpes zoster infection.
© Springer Science+Business Media
Herpes zoster may disseminate to other regions of the skin and to visceral organs, especially in patients who are immunocompromised.
Geniculate zoster (Ramsay Hunt syndrome, herpes zoster oticus) results from involvement of the geniculate ganglion. Ear pain, facial paralysis, and sometimes vertigo occur. Vesicles erupt in the external auditory canal, and taste may be lost in the anterior two-thirds of the tongue.
Ophthalmic herpes zoster results from involvement of the gasserian ganglion, with pain and vesicular eruption around the eye and on the forehead, in the V1 distribution of the ophthalmic division of cranial nerve V (trigeminal). Ocular disease can be severe. Vesicles on the tip of the nose (Hutchinson sign) indicate involvement of the nasociliary branch and a higher risk of severe ocular disease. However, the eye may be involved in the absence of lesions on the tip of the nose. An ophthalmology consultation should be sought if feasible in V1 distribution zoster.


Herpes zoster in V2 (maxillary branch) and V3 (mandibular branch) distributions of the trigeminal nerve.
© Springer Science+Business Media


The rash of herpes zoster usually shows up along the path of the nerve that is involved. In this photo, the path of the branches of part of the trigeminal nerve demarcates the rash sharply from surrounding normal skin, that is, between where the vesicles (bumps) appear and where they do not. The appearance of a vesicle on the tip of the nose indicates an increased risk of severe ocular involvement.
© Springer Science+Business Media
Intraoral zoster is uncommon but may produce a sharp unilateral distribution of lesions. No intraoral prodromal symptoms occur.
Herpes zoster–induced rash must be differentiated from the rash caused by that of herpes simplex, which is much more common and carries a much higher rate of recurrence (2).
Postherpetic neuralgia
Up to 6% of patients with herpes zoster experience another outbreak (3), although this percentage may be higher in immunocompromised hosts. However, many patients, particularly older patients, have localized pain with variable intensity lasting > 3 months from the last crusted lesion in the involved distribution (postherpetic neuralgia).
Symptoms and signs references
1. Cohen JI. Clinical practice: Herpes zoster. N Engl J Med. 2013;369(3):255-263. doi:10.1056/NEJMcp1302674
2. Johnson JR. Recurrent Herpes Zoster. J Infect Dis. 2021;224(3):554. doi:10.1093/infdis/jiaa732
3. Yawn BP, Wollan PC, Kurland MJ, St Sauver JL, Saddier P. Herpes zoster recurrences more frequent than previously reported. Mayo Clin Proc 86(2):88-93, 2011. doi:10.4065/mcp.2010.0618
Pearls & Pitfalls
|
The pain of postherpetic neuralgia may be sharp and intermittent or constant and may be debilitating. It may persist for months or years or permanently.
Diagnosis of Herpes Zoster
History and physical examination
Sometimes, molecular tests (polymerase chain reaction [PCR]) or culture
Herpes zoster is suspected in patients with the characteristic rash (ie, dermatomal distribution) and sometimes even before the rash appears, if patients have typical pain in a dermatomal distribution. Diagnosis is usually based on the virtually pathognomonic rash.
If the diagnosis is equivocal, virus can be detected by culture or PCR. Antigen detection from a biopsy sample can also be used to detect herpes zoster.
Detecting multinucleate giant cells with a Tzanck test can confirm infection with a herpesvirus but not differentiate the type of virus, because the Tzanck test is positive in both herpes zoster and herpes simplex. Differentiation is instead clinical, as herpes simplex virus (HSV) may cause nearly identical lesions, but unlike herpes zoster, HSV tends to recur and is not dermatomal.
Treatment of Herpes Zoster
Symptomatic treatment
Antivirals (acyclovir, famciclovir, valacyclovir), especially for patients who are immunocompromised
Wet compresses are soothing, but systemic analgesics are often necessary.
For treatment of ophthalmic herpes zoster, an ophthalmologist should be consulted. For treatment of otic herpes zoster, an otolaryngologist should be consulted.
Antiviral therapy
Treatment with oral antivirals decreases the severity and duration of the acute eruption and decreases the rate of serious complications in patients who are immunocompromised. A Cochrane review concluded oral acyclovir does not reduce the risk of proceeding on to postherpetic neuralgia, and that evidence for other antivirals was insufficient as to whether they may reduce the incidence of postherpetic neuralgia (1). In patients who are immunocompetent, antiviral therapy is often reserved for those who are ≥ 50 years, in whom benefit is greatest, although some experts recommend treating all patients with zoster (2, 3). Treatment is also indicated in patients with severe pain, facial rash suggestive of otic or ophthalmic herpes zoster, and in patients who are immunocompromised.
Treatment of herpes zoster should start as soon as possible, ideally during the prodrome, and is less likely to be effective if given >72 hours after onset of skin lesions, especially in the absence of newly forming lesions (3). Normal duration of treatment is between 7 to 10 days. Famciclovir and valacyclovir have better bioavailability with oral dosing than acyclovir, and therefore for herpes zoster, they are generally preferred. A Cochrane review concluded that evidence is uncertain as to whether the administration of glucocorticoids prevents postherpetic neuralgia 6 months after the onset of zoster (4).
For less severely immunocompromised patients, oral famciclovir, valacyclovir, or acyclovir is a reasonable option; famciclovir and valacyclovir are preferred. For patients who are severely immunocompromised, IV acyclovir is recommended. Some experts recommend treatment beyond 7 to 10 days, lasting until all lesions are crusted, for immunocompromised patients (including children), and potentially switching to oral regimens once the patient is clinically improved (5).
Although data concerning the safety of acyclovir and valacyclovir during pregnancy are reassuring, the safety of antiviral therapy during pregnancy is not firmly established. Because congenital varicella can result from maternal varicella but rarely results from maternal zoster, the potential benefit of treatment of pregnant patients should outweigh possible risks to the fetus. Pregnant patients with severe rash, severe pain, or ophthalmic zoster can be treated, preferably with acyclovir, because there is longer experience with its use in pregnancy as compared to other medications, although valacyclovir remains an option. There are few data regarding the safety of famciclovir in pregnancy, so it is not generally recommended in pregnant women (6).
Management of postherpetic neuralgia
Management of postherpetic neuralgia can be particularly difficult. Postherpetic neuralgia can considerably impact quality of life, especially in older patients. Treatments include gabapentin, pregabalin, tricyclic antidepressants, topical capsaicin or lidocaine ointment, and botulinum toxin injection (7). Opioid analgesics may be necessary. Intrathecal methylprednisolone may be of benefit.
Treatment references
1. Chen N, Li Q, Yang J, Zhou M, Zhou D, He L. Antiviral treatment for preventing postherpetic neuralgia. Cochrane Database Syst Rev. 2014;2014(2):CD006866. Published 2014 Feb 6. doi:10.1002/14651858.CD006866.pub3
2. Balfour HH Jr. Antiviral drugs. N Engl J Med. 1999;340(16):1255-1268. doi:10.1056/NEJM199904223401608
3. Cohen JI. Clinical practice: Herpes zoster. N Engl J Med. 2013;369(3):255-263. doi:10.1056/NEJMcp1302674
4. Jiang X, Li Y, Chen N, Zhou M, He L. Corticosteroids for preventing postherpetic neuralgia. Cochrane Database Syst Rev. 2023;12(12):CD005582. Published 2023 Dec 5. doi:10.1002/14651858.CD005582.pub5
5. ClinicalInfo.HIV.gov. Guidelines for the Prevention and Treatment of Opportunistic Infections in Children With and Exposed to HIV. Accessed October 18, 2025.
6. Pasternak B, Hviid A. Use of acyclovir, valacyclovir, and famciclovir in the first trimester of pregnancy and the risk of birth defects. JAMA. 2010;304(8):859-866. doi:10.1001/jama.2010.1206
7. Johnson RW, Rice AS. Clinical practice. Postherpetic neuralgia. N Engl J Med. 2014;371(16):1526-1533. doi:10.1056/NEJMcp1403062
Prevention of Herpes Zoster
A recombinant zoster vaccine is recommended for adults ≥ 50 years whether they have had herpes zoster or been given the older, live-attenuated vaccine or not; 2 doses of the recombinant zoster vaccine are given 2 to 6 months apart. The recombinant zoster vaccine is also recommended for adults ≥ 19 years who are or will be immunodeficient or immunosuppressed because of disease or therapy, including those with a prior history of varicella, varicella vaccine, or herpes zoster. The recombinant vaccine appears to provide much better and longer-lasting protection than the older, single-dose, live-attenuated zoster vaccine (which is a higher-dose version of the varicella vaccine). In a large clinical trial, the recombinant zoster vaccine was found to be approximately 97% effective at preventing herpes zoster (1). In 1 longitudinal cohort, vaccine effectiveness was sustained 4 years post-vaccination (2).
A postmarketing observational study of insurance claims-based data observed a slightly increased risk of Guillain-Barré syndrome during the 42 days following vaccination with the recombinant zoster vaccine (3). In the United States, the Food and Drug Administration determined that, while there is an association with Guillain-Barre syndrome, (1) available evidence is insufficient to establish a causal relationship (2) and the benefits of vaccination outweigh the associated risks; as a result, some clinicians avoid recombinant zoster vaccine in patients with a prior history of Guillain-Barre syndrome (see FDA Requires a Warning About Guillain-Barré Syndrome (GBS) be Included in the Prescribing Information for Shingrix).
Prevention references
1. Lal H, Cunningham AL, Godeaux O, et al. Efficacy of an adjuvanted herpes zoster subunit vaccine in older adults. N Engl J Med. 372(22):2087-96, 2015. PMID: 25916341. doi: 10.1056/NEJMoa1501184
2. Tseng HF, Sy LS, Ackerson BK, et al. Effectiveness of the Adjuvanted Recombinant Zoster Vaccine in Adults ≥50 Years in the United States. Clin Infect Dis. Published online June 23, 2025. doi:10.1093/cid/ciaf329
3. Goud R, Lufkin B, Duffy J, et al. Risk of Guillain-Barré Syndrome Following Recombinant Zoster Vaccine in Medicare Beneficiaries. JAMA Intern Med. 2021;181(12):1623-1630. doi:10.1001/jamainternmed.2021.6227
Key Points
Herpes zoster is caused by reactivation of the varicella-zoster virus (the cause of chickenpox) from its latent phase.
A painful rash, usually crops of vesicles on an erythematous base, develops on 1 or more adjacent dermatomes.
Antivirals (acyclovir, famciclovir, valacyclovir) are beneficial, especially for patients who are immunocompromised.
Analgesics are often necessary.
Adults ≥ 50 years and adults ≥ 19 years who are immunocompromised and at risk for zoster should be given recombinant zoster vaccine whether they have had herpes zoster or not.
Up to 6% of patients may have another outbreak of zoster.
Many, particularly older patients, have persistent or recurrent pain for months or years following zoster (postherpetic neuralgia).
Drug Information for the Topic





